Tietze syndrome
| Tietze syndrome | |
|---|---|
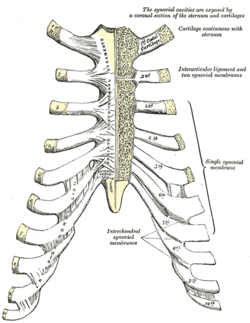 Sternocostal and interchondral articulations. Anterior view. (Costal cartilages visible on diagram.) | |
| Classification and external resources | |
| ICD-10 | M94.0 |
| ICD-9 | 733.6 |
| DiseasesDB | 13112 |
| Patient UK | Tietze syndrome |
| MeSH | D013991 |
Tietze syndrome is a benign inflammation of one or more of the costal cartilages. It was first described in 1921 by the German surgeon Alexander Tietze (1864–1927).[1][2]
Though thought to be the same conditions, Tietze syndrome is not the same as costochondritis.[3] Tietze syndrome is differentiated from costochondritis by swelling of the costal cartilages, which does not appear in costochondritis. Like costochondritis, it was at one time thought to be associated with, or caused by, a viral infection acquired during surgery. This is now known not to be the case, as most sufferers have not had recent surgery.
Signs and symptoms
The main presentation of the syndrome is significant, acute pain in the chest, along with tenderness and some swelling of the cartilages affected, which is commonly palpable on examination. Perceived pain is often exacerbated with respiration.[4] Although many times it can be extremely painful, to the point of being debilitating, Tietze's Syndrome is considered to be a benign condition that generally resolves in 12 weeks. However, it can often be a chronic condition. The pain can be identical to a heart attack and can cause hyper ventilating, anxiety attacks, passing out, panic attacks and temporary numbness/paralysis.
Many cases of heart attack victims have been re-considered and improperly diagnosed, due to the identical nature of the symptoms. In females, it is often misdiagnosed as mastalgia. Costochondritis symptoms are similar to Tietze's, the prime difference being that the pain radiates to the arms and shoulders in the latter.
Cause
While the true causes of Tietze's Syndrome are not well understood, it often results from a physical strain or minor injury, such as repeated coughing, sneezing, vomiting, or impacts to the chest. It has even been known to occur after hearty bouts of laughter. It can occur by over exerting or by an injury in the chest and breast.
Psychological stress can exacerbate Tietze's Syndrome, but there is no evidence to suggest that it is a direct cause.
Patients who have had radiation therapy to the chest/breast will often experience this syndrome which can occur shortly after therapy or years later. It is found more often in teens than adults.
Differential diagnosis
Although patients will often mistake the pain of Tietze's Syndrome for a myocardial infarction (heart attack), the syndrome does not progress to cause harm to any organs.
It is important to rule out a heart attack, as the symptoms can be similar. After assessment, providers often reassure patients that their symptoms are not associated with a heart attack, although they may need to treat the pain, which in some cases can be severe enough to cause significant but temporary disability to the patient.
References
External links
- Tietze's Syndrome Info site
- Overview at About.com
- NetDoctor
- Overview at Mayo Clinic
- Costochondritis and Tietze Syndrome
- Costochondritis at WebMD
- Clinical presentation and chiropractic treatment of Tietze syndrome at National University of Health Sciences
- Tietze’s Syndrome in the emergency department: A rare etiology of atraumatic chest pain at Scientific Research
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||