Screening (medicine)
.jpg)
Screening, in medicine, is a strategy used in a population to identify an unrecognized disease in individuals without signs or symptoms. This can include individuals with pre-symptomatic or unrecognized symptomatic disease. As such, screening tests are somewhat unique in that they are performed on persons apparently in good health.
Screening interventions are designed to identify disease in a community early, thus enabling earlier intervention and management in the hope to reduce mortality and suffering from a disease. Although screening may lead to an earlier diagnosis, not all screening tests have been shown to benefit the person being screened; overdiagnosis, misdiagnosis, and creating a false sense of security are some potential adverse effects of screening. For these reasons, a test used in a screening program, especially for a disease with low incidence, must have good sensitivity in addition to acceptable specificity.[1]
Several types of screening exist: universal screening involves screening of all individuals in a certain category (for example, all children of a certain age). Case finding involves screening a smaller group of people based on the presence of risk factors (for example, because a family member has been diagnosed with a hereditary disease). Screening interventions are not designed to be diagnostic, and often have significant rates of both false positive and false negative results.
Principles of screening
World Health Organization guidelines, often referred to as Wilson's Criteria were published in 1968, but are still applicable today.[2]
- The condition should be an important health problem.
- There should be a treatment for the condition.
- Facilities for diagnosis and treatment should be available.
- There should be a latent stage of the disease.
- There should be a test or examination for the condition.
- The test should be acceptable to the population.
- The natural history of the disease should be adequately understood.
- There should be an agreed policy on whom to treat.
- The total cost of finding a case should be economically balanced in relation to medical expenditure as a whole.
- Case-finding should be a continuous process, not just a "once and for all" project.
Types of screening
.jpg)
- Mass screening : Mass screening means, the screening of a whole population or a subgroup. It is offered to all, irrespective of the risk status of the individual.
- High risk or selective screening : High risk screening is conducted among risk populations only.
- Multiphasic screening : It is the application of two or more screening tests to a large population at one time instead of carrying out separate screening tests for single diseases.
- When done thoughtfully and based on research, identification of risk factors can be a strategy for medical screening.[3]
Examples of screening
Common screening programmes
In many countries there are population-based screening programmes. In some countries, such as the UK, these operate at a national level. Common screening programmes include:
- Cancer screening
- Pap smear or liquid-based cytology to detect potentially precancerous lesions and prevent cervical cancer
- Mammography to detect breast cancer
- Colonoscopy and fecal occult blood test to detect colorectal cancer
- Dermatological check to detect melanoma
- PPD test to screen for exposure to tuberculosis
- Beck Depression Inventory to screen for depression
- SPAI-B, the Liebowitz Social Anxiety Scale and Social Phobia Inventory to screen for social anxiety disorder
- Alpha-fetoprotein, blood tests and ultrasound scans for pregnant women to detect fetal abnormalities
- Bitewing radiographs to screen for interproximal dental caries
- Ophthalmoscopy or digital photography and image grading for diabetic retinopathy
- Ultrasound scan for abdominal aortic aneurysm
- Screening of potential sperm bank donors
- Screening for metabolic syndrome
- Screening for potential hearing loss in newborns
School-based screening
Most public school systems in the United States screen students periodically for hearing and vision deficiencies and dental problems. Screening for spinal and posture issues such as scoliosis is sometimes carried out, but is controversial as scoliosis (unlike vision or dental issues) is found in only a very small segment of the general population and because students must remove their shirts for screening. Many states no longer mandate scoliosis screenings, or allow them to be waived with parental notification.
Medical equipment used in screening
Medical equipment used in screening tests is usually different from equipment used in diagnostic tests as screening tests are used to indicate the likely presence or absence of a disease or condition in people not presenting symptoms; while diagnostic medical equipment is used to make quantitative physiological measurements to confirm and determine the progress of a suspected disease or condition. Medical screening equipment must be capable of fast processing of many cases, but may not need to be as precise as diagnostic equipment.
Limitations of screening
Screening can detect medical conditions at an early stage before symptoms present while treatment is more effective than for later detection. In the best of cases lives are saved. Like any medical test, the tests used in screening are not perfect. The test result may incorrectly show positive for those without disease (false positive), or negative for people who have the condition (false negative). Limitations of screening programmes can include:
- Screening can involve cost and use of medical resources on a majority of people who do not need treatment.
- Adverse effects of screening procedure (e.g. stress and anxiety, discomfort, radiation exposure, chemical exposure).
- Stress and anxiety caused by a false positive screening result.
- Unnecessary investigation and treatment of false positive results.
- Stress and anxiety caused by prolonging knowledge of an illness without any improvement in outcome.
- A false sense of security caused by false negatives, which may delay final diagnosis.
Screening for dementia in the English NHS is controversial because it could cause undue anxiety in patients and support services would be stretched. A GP reported "The main issue really seems to be centred around what the consequences of a such a diagnosis is and what is actually available to help patients."[4]
Analysis of screening
To many people, screening instinctively seems like an appropriate thing to do, because catching something earlier seems better. However, no screening test is perfect. There will always be the problems with incorrect results and other issues listed above.
Before a screening program is implemented, it should ideally be looked at to ensure that putting it in place would do more good than harm. The best studies for assessing whether a screening test will increase a population's health are rigorous randomized controlled trials.
When studying a screening program using case-control or, more usually, cohort studies, various factors can cause the screening test to appear more successful than it really is. A number of different biases, inherent in the study method, will skew results.
Screening can certainly improve outcomes, but this must be confirmed with proper statistical analysis, not simplistic comparison of numbers.
Lead time bias
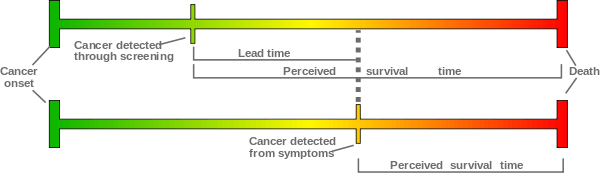
The intention of screening is to diagnose a disease earlier than it would be without screening. Without screening the disease may be discovered later, when symptoms appear.
Even if in both cases a person will die at the same time, because we diagnosed the disease earlier with screening the survival time since diagnosis is longer with screening; but life span has not been prolonged, and there will be added anxiety as the patient must live with knowledge of the disease for longer.
Looking at statistics of survival time since diagnosis, screening will show an increase (this gain is called lead time). If we do not think about what survival time actually means in this context, we might attribute success to a screening test that does nothing but advance diagnosis; comparing statistics of mortality due to a disease in a screened and unscreened population gives more meaningful information.
Length time bias

Many screening tests involve the detection of cancers. It is often hypothesized that slower-growing tumors have better prognoses than tumors with high growth rates. Screening is more likely to detect slower-growing tumors (due to longer pre-clinical sojourn time), which may be less deadly. Thus screening may tend to detect cancers that would not have killed the patient or even been detected prior to death from other causes.
Selection bias
Not everyone will partake in a screening program. There are factors that differ between those willing to get tested and those who are not.
If people with a higher risk of a disease are more likely to be screened, for instance women with a family history of breast cancer are more likely than other women to join a mammography program, then a screening test will look worse than it really is: negative outcomes among the screened population will be higher than for a random sample.
Selection bias may also make a test look better than it really is. If a test is more available to young and healthy people (for instance if people have to travel a long distance to get checked) then fewer people in the screening population will have negative outcomes than for a random sample, and the test will seem to make a positive difference.
Overdiagnosis
Screening may identify abnormalities that would never cause a problem in a person's lifetime. An example of this is prostate cancer screening; it has been said that "more men die with prostate cancer than of it".[5] Autopsy studies have shown that a high proportion of elderly men who have died of other causes are found to have had prostate cancer.
Aside from issues with unnecessary treatment (prostate cancer treatment is by no means without risk), overdiagnosis makes a study look good at picking up abnormalities, even though they are sometimes harmless.
Overdiagnosis occurs when all of these people with harmless abnormalities are counted as "lives saved" by the screening, rather than as "healthy people needlessly harmed by overdiagnosis".
Avoidance of bias
The best way to minimise these biases is to use a randomized controlled trial. These need to be very large, and very strict in terms of research procedure. Such studies take a long time and are expensive, but provide the best information for evidence-based medicine.
See also
- Fetal screening
- General medical examination
- Genetic testing
- Medical test
- Newborn screening
- Pedodontics
- Scoliosis
- UK National Screening Committee
References
- UK National Screening Committee. Criteria for appraising the viability, effectiveness and appropriateness of a screening programme. 2009. Last accessed April 22, 2009.
- Raffle, Angela E., and J. A. Muir Gray. Screening - Evidence and practice. Oxford University Press, 2007.
- Health Knowledge Interactive Learning Module on Screening by Angela Raffle. Last accessed January 18, 2010.
- Health Screening Guidelines for Adults,Children and Newborns
- ↑ http://emedicine.medscape.com/article/773832-overview#aw2aab6b5
- ↑ Wilson JMG, Jungner G. (1968) Principles and practice of screening for disease (large pdf). WHO Chronicle Geneva:World Health Organization. 22(11):473. Public Health Papers, #34.
- ↑ Wald, N J; Hackshaw, A K; Frost, C D (1999). "When can a risk factor be used as a worthwhile screening test?". BMJ 319 (7224): 1562–1565. doi:10.1136/bmj.319.7224.1562. ISSN 0959-8138.
- ↑ "GPs hit by widespread complaints from patients 'unhappy' over dementia screening". Pulse. 22 November 2013. Retrieved 22 November 2013.
- ↑ The Complete Book of Men's Health. Men's Health Books. Rodale Books. 2000. ISBN 9781579542986.