Reproductive rights
| Rights |
|---|
| Theoretical distinctions |
| Human rights |
| Rights by claimant |
| Other groups of rights |
| Part of a series on | ||||||||
| Feminism | ||||||||
|---|---|---|---|---|---|---|---|---|
|
History
|
||||||||
|
||||||||
|
|
||||||||
|
By country |
||||||||
|
Lists and categories
|
||||||||
| Feminism portal | ||||||||
| Part of a series on |
| Feminist philosophy |
|---|
| Major works |
| Major theorists |
| Key concepts |
Reproductive rights are legal rights and freedoms relating to reproduction and reproductive health.[1] The World Health Organization defines reproductive rights as follows:
Reproductive rights rest on the recognition of the basic right of all couples and individuals to decide freely and responsibly the number, spacing and timing of their children and to have the information and means to do so, and the right to attain the highest standard of sexual and reproductive health. They also include the right of all to make decisions concerning reproduction free of discrimination, coercion and violence.[2]
Reproductive rights may include some or all of the following: the right to legal and safe abortion; the right to birth control; freedom from coerced sterilization and contraception; the right to access good-quality reproductive healthcare; and the right to education and access in order to make free and informed reproductive choices.[3] Reproductive rights may also include the right to receive education about sexually transmitted infections and other aspects of sexuality, and protection from gender-based practices such as female genital mutilation (FGM).[1][3][4][5]
Reproductive rights began to develop as a subset of human rights at the United Nation's 1968 International Conference on Human Rights.[4] The resulting non binding Proclamation of Teheran was the first international document to recognize one of these rights when it stated that: "Parents have a basic human right to determine freely and responsibly the number and the spacing of their children."[4][6] States, though, have been slow in incorporating these rights in internationally legally binding instruments. Thus, while some of these rights have already been recognized in hard law, that is, in legally binding international human rights instruments, others have been mentioned only in non binding recommendations and, therefore, have at best the status of soft law in international law, while a further group is yet to be accepted by the international community and therefore remains at the level of advocacy.[7]
Issues related to reproductive rights are some of the most vigorously contested rights' issues worldwide, regardless of the population's socioeconomic level, religion or culture.[8]
The issue of reproductive rights is frequently presented as being of vital importance in discussions and articles by population concern organizations such as Population Matters.[9]
Reproductive rights are a subset of sexual and reproductive health and rights.
History
Proclamation of Teheran
In 1945, the United Nations Charter included the obligation "to promote... universal respect for, and observance of, human rights and fundamental freedoms for all without discrimination as to race, sex, language, or religion". However, the Charter did not define these rights. Three years later, the UN adopted the Universal Declaration of Human Rights (UDHR), the first international legal document to delineate human rights; the UDHR does not mention reproductive rights. Reproductive rights began to appear as a subset of human rights in the 1968 Proclamation of Teheran, which states: "Parents have a basic human right to determine freely and responsibly the number and the spacing of their children".[6]
This right was affirmed by the UN General Assembly in the 1969 Declaration on Social Progress and Development which states "The family as a basic unit of society and the natural environment for the growth and well-being of all its members, particularly children and youth, should be assisted and protected so that it may fully assume its responsibilities within the community. Parents have the exclusive right to determine freely and responsibly the number and spacing of their children."[4][10] The 1975 UN International Women's Year Conference echoed the Proclamation of Teheran.
Cairo Programme of Action
The twenty-year "Cairo Programme of Action" was adopted in 1994 at the International Conference on Population and Development (ICPD) in Cairo. The non binding Programme of Action asserted that governments have a responsibility to meet individuals' reproductive needs, rather than demographic targets. It recommended that family planning services be provided in the context of other reproductive health services, including services for healthy and safe childbirth, care for sexually transmitted infections, and post-abortion care. The ICPD also addressed issues such as violence against women, sex trafficking, and adolescent health.[11] The Cairo Program is the first international policy document to define reproductive health,[11] stating:
Reproductive health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity, in all matters relating to the reproductive system and its functions and processes. Reproductive health therefore implies that people are able to have a satisfying and safe sex life and that they have the capability to reproduce and the freedom to decide if, when and how often to do so. Implicit in this last condition are the right of men and women to be informed [about] and to have access to safe, effective, affordable and acceptable methods of family planning of their choice, as well as other methods for regulation of fertility which are not against the law, and the right of access to appropriate health-care services that will enable women to go safely through pregnancy and childbirth and provide couples with the best chance of having a healthy infant [para. 72].[1]
Unlike previous population conferences, a wide range of interests from grassroots to government level were represented in Cairo. 179 nations attended the ICPD and overall eleven thousand representatives from governments, NGOs, international agencies and citizen activists participated.[11] The ICPD did not address the far-reaching implications of the HIV/AIDS epidemic. In 1999, recommendations at the ICPD+5 were expanded to include commitment to AIDS education, research, and prevention of mother-to-child transmission, as well as to the development of vaccines and microbicides.[12]
The Cairo Programme of Action was adopted by 184 UN member states. Nevertheless, many Latin American and Islamic states made formal reservations to the programme, in particular, to its concept of reproductive rights and sexual freedom, to its treatment of abortion, and to its potential incompatibility with Islamic law.[13]
Beijing Platform
The 1995 Fourth World Conference on Women in Beijing, in its non-binding Declaration and Platform for Action, supported the Cairo Programme's definition of reproductive health, but established a broader context of reproductive rights:
The human rights of women include their right to have control over and decide freely and responsibly on matters related to their sexuality, including sexual and reproductive health, free of coercion, discrimination and violence. Equal relationships between women and men in matters of sexual relations and reproduction, including full respect for the integrity of the person, require mutual respect, consent and shared responsibility for sexual behavior and its consequences [para. 96].[1]
The Beijing Platform demarcated twelve interrelated critical areas of the human rights of women that require advocacy. The Platform framed women's reproductive rights as "indivisible, universal and inalienable human rights."[14]
The Yogyakarta Principles
The Yogyakarta Principles on the Application of International Human Rights Law in relation to Sexual Orientation and Gender Identity, proposed by a group of experts in November 2006[15] but not yet incorporated by States in international law,[16] declares in its Preamble that "the international community has recognized the rights of persons to decide freely and responsibly on matters related to their sexuality, including sexual and reproductive health, free from coercion, discrimination, and violence." In relation to reproductive health, Principle 9 on "The Right to Treatment with Humanity while in Detention" requires that "States shall... [p]rovide adequate access to medical care and counseling appropriate to the needs of those in custody, recognizing any particular needs of persons on the basis of their sexual orientation and gender identity, including with regard to reproductive health, access to HIV/AIDS information and therapy and access to hormonal or other therapy as well as to gender-reassignment treatments where desired."[17] Nonetheless, African, Caribbean and Islamic Countries, as well as the Russian Federation, have objected to the use of these principles as Human Rights standards.[18]
Other
The first legal textbook on reproductive rights law, Cases on Reproductive Rights and Justice by Melissa Murray and Kristin Luker, was published in 2015 by Foundation Press.[19]
Human rights
Since most existing legally binding international human rights instruments do not explicitly mention sexual and reproductive rights, a broad coalition of NGOs, civil servants, and experts working in international organizations have been promoting a reinterpretation of those instruments to link the realization of the already internationally recognized human rights with the realization of reproductive rights.[20] An example of this linkage is provided by the 1994 Cairo Programme of Action:
reproductive rights embrace certain human rights that are already recognized in national laws, international human rights documents and other relevant United Nations consensus documents. These rights rest on the recognition of the basic right of all couples and individuals to decide freely and responsibly the number, spacing and timing of their children and to have the information and means to do so, and the right to attain the highest standard of sexual and reproductive health. It also includes the right of all to make decisions concerning reproduction free of discrimination, coercion and violence as expressed in human rights documents. In the exercise of this right, they should take into account the needs of their living and future children and their responsibilities towards the community.[21]
Similarly, Amnesty International has argued that the realisation of reproductive rights is linked with the realisation of a series of recognised human rights, including the right to health, the right to freedom from discrimination, the right to privacy, and the right not to be subjected to torture or ill-treatment.[3] However, not all states have accepted the inclusion of reproductive rights in the body of internationally recognized human rights. At the Cairo Conference, several states made formal reservations either to the concept of reproductive rights or to its specific content. Ecuador, for instance, stated that:
With regard to the Programme of Action of the Cairo International Conference on Population and Development and in accordance with the provisions of the Constitution and laws of Ecuador and the norms of international law, the delegation of Ecuador reaffirms, inter alia, the following principles embodied in its Constitution: the inviolability of life, the protection of children from the moment of conception, freedom of conscience and religion, the protection of the family as the fundamental unit of society, responsible paternity, the right of parents to bring up their children and the formulation of population and development plans by the Government in accordance with the principles of respect for sovereignty. Accordingly, the delegation of Ecuador enters a reservation with respect to all terms such as "regulation of fertility", "interruption of pregnancy", "reproductive health", "reproductive rights" and "unwanted children", which in one way or another, within the context of the Programme of Action, could involve abortion.[13]
Similar reservations were made by Argentina, Dominican Republic, El Salvador, Honduras, Malta, Nicaragua, Paraguay, Peru and the Holy See. Islamic Countries, such as Brunei, Djibouti, Iran, Jordan, Kuwait, Libya, Syria, United Arab Emirates, and Yemen made broad reservations against any element of the programme that could be interpreted as contrary to the Sharia. Guatemala even questioned whether the conference could legally proclaim new human rights.[22]
Women's rights
| Part of a series on | ||||||||
| Feminism | ||||||||
|---|---|---|---|---|---|---|---|---|
|
History
|
||||||||
|
||||||||
|
|
||||||||
|
By country |
||||||||
|
Lists and categories
|
||||||||
| Feminism portal | ||||||||
The United Nations Population Fund (UNFPA) and the World Health Organization (WHO) advocate for reproductive rights with a primary emphasis on women's rights. In this respect the UN and WHO focus on a range of issues from access to family planning services, sex education, menopause, and the reduction of obstetric fistula, to the relationship between reproductive health and economic status.
The reproductive rights of women are advanced in the context of the right to freedom from discrimination and the social and economic status of women. The group Development Alternatives with Women for a New Era (DAWN) explained the link in the following statement:
Control over reproduction is a basic need and a basic right for all women. Linked as it is to women's health and social status, as well as the powerful social structures of religion, state control and administrative inertia, and private profit, it is from the perspective of poor women that this right can best be understood and affirmed. Women know that childbearing is a social, not a purely personal, phenomenon; nor do we deny that world population trends are likely to exert considerable pressure on resources and institutions by the end of this century. But our bodies have become a pawn in the struggles among states, religions, male heads of households, and private corporations. Programs that do not take the interests of women into account are unlikely to succeed...[4]
Women's reproductive rights have long retained key issue status in the debate on overpopulation.[9]
"The only ray of hope I can see – and it's not much – is that wherever women are put in control of their lives, both politically and socially; where medical facilities allow them to deal with birth control and where their husbands allow them to make those decisions, birth rate falls. Women don't want to have 12 kids of whom nine will die." David Attenborough[23]
Attempts have been made to analyse the socioeconomic conditions that affect the realisation of a woman's reproductive rights. The term reproductive justice has been used to describe these broader social and economic issues. Proponents of reproductive justice argue that while the right to legalized abortion[24] and contraception applies to everyone, these choices are only meaningful to those with resources, and that there is a growing gap between access and affordability.[25]
Men's rights
Men's reproductive rights have been claimed by various organizations, both for issues of reproductive health, and other rights related to sexual reproduction.
Three international issues in men's reproductive health are sexually transmitted diseases, cancer and exposure to toxins.[26]
Recently men's reproductive right with regards to paternity have become subject of debate in the U.S. The term "male abortion" was coined by Melanie McCulley, a South Carolina attorney, in a 1998 article. The theory begins with the premise that when a woman becomes pregnant she has the option of abortion, adoption, or parenthood; it argues, in the context of legally recognized gender equality, that in the earliest stages of pregnancy the putative (alleged) father should have the right to relinquish all future parental rights and financial responsibility, leaving the informed mother with the same three options.[27] This concept has been supported by a former president of the feminist organization National Organization for Women, attorney Karen DeCrow.[28] The feminist argument for male reproductive choice contends that the uneven ability to choose experienced by men and women in regards to parenthood is evidence of a state-enforced coercion favoring traditional sex roles.[29]
In 2006, the National Center for Men brought a case in the US, Dubay v. Wells (dubbed by some "Roe v. Wade for men"), that argued that in the event of an unplanned pregnancy, when an unmarried woman informs a man that she is pregnant by him, he should have an opportunity to give up all paternity rights and responsibilities. Supporters argue that this would allow the woman time to make an informed decision and give men the same reproductive rights as women.[30][31] In its dismissal of the case, the U.S. Court of Appeals (Sixth Circuit) stated that "the Fourteenth Amendment does not deny to [the] State the power to treat different classes of persons in different ways."[32]
Intersex and reproductive rights
Intersex, in humans and other animals, is a variation in sex characteristics including chromosomes, gonads, or genitals that do not allow an individual to be distinctly identified as male or female. Such variation may involve genital ambiguity, and combinations of chromosomal genotype and sexual phenotype other than XY-male and XX-female.[33][34] Intersex persons are subjected to involuntary "sex normalizing" surgical and hormonal treatments in infancy and childhood, often also including sterilization.[35][36][37][38][39]
UN agencies have begun to take note. On 1 February 2013, Juan E Mendés, the UN Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment, issued a statement condemning non-consensual surgical intervention on intersex people. His report stated, "Children who are born with atypical sex characteristics are often subject to irreversible sex assignment, involuntary sterilization, involuntary genital normalizing surgery, performed without their informed consent, or that of their parents, "in an attempt to fix their sex", leaving them with permanent, irreversible infertility and causing severe mental suffering".[40] In May 2014, the World Health Organization issued a joint statement on Eliminating forced, coercive and otherwise involuntary sterilization, An interagency statement with the OHCHR, UN Women, UNAIDS, UNDP, UNFPA and UNICEF. The report references the involuntary surgical "sex-normalising or other procedures" on "intersex persons". It questions the medical necessity of such treatments, patients' ability to consent, and a weak evidence base.[41] The report recommends a range of guiding principles to prevent compulsory sterilization in medical treatment, including ensuring patient autonomy in decision-making, ensuring non-discrimination, accountability and access to remedies.[42]
Youth rights and access
Youth are often denied equal access to reproductive health services because health workers view adolescent sexual activity as unacceptable,[43] or see sex education as the responsibility of parents. Providers of reproductive health have little accountability to youth clients, a primary factor in denying youth access to reproductive health care.[43]
Africa
Many unintended pregnancies stem from traditional contraceptive methods or no contraceptive measures.[44]
Youth sexual education in Uganda is relatively low. Comprehensive sex education is not generally taught in schools; even if it was, the majority of young people do not stay in school after the age of fifteen, so information would be limited regardless.[45]

Africa experiences high rates of unintended pregnancy, along with high rates of HIV/AIDS. Young women aged 15–24 are eight times more likely to have HIV/AIDS than young men. Attempted abortions and unsafe abortions are a risk for youth in Africa. On average, there are 2.4 million unsafe abortions in East Africa, 1.8 million in Western Africa, over 900,000 in Middle Africa, and over 100,000 in Southern Africa each year.[44]
In Uganda, abortion is illegal except to save the mother's life. However, 78% of teenagers report knowing someone who has had an abortion and the police do not always prosecute everyone who has an abortion. An estimated 22% of all maternal deaths in the area stem from illegal, unsafe abortions.[45]
European Union
Over 85% of European women (all ages) have used some form of birth control in their lives.[46] Europeans as an aggregate report using the pill and condoms as the most commonly used contraceptives.[46]
Family planning has become prominent throughout the region and most taboos concerning sexuality have been lifted or diminished.[47] Youth sexual and reproductive health centers have been established across most of the region.[47] In Sweden, approximately 80% of girls and 17% of boys have visited these youth centers, which provide all or nearly all services youth need at little to no charge.[47] Sweden has the highest percentage of lifetime contraceptive use, with 96% of its inhabitants claiming to have used birth control at some point in their life.[46] Sweden also has a high self-reported rate of postcoital pill use.[46] A 2007 anonymous survey of Swedish 18-year-olds showed that three out of four youth were sexually active, with 5% reporting having had an abortion and 4% reporting the contraction of an STI.[48] Similar centers exist in Estonia, Finland, and Portugal.[49]
Views on sexual practice vary throughout the region. For example, in the United Kingdom (UK), sex among youth is generally looked down upon and seen as a problem in need of solution. In the Netherlands, sex between youth is viewed as normal and therefore not discussed in terms of solutions, but rather in terms of ensuring safe practices. That being said, the UK tends to focus on stopping sexual behavior, while the Netherlands focuses on building self-esteem and healthy relationships.[47]
Latin America
In Ecuador, education and class play a large role in the definition of which young women become pregnant and which do not - 50% of young women who are illiterate get pregnant, compared to 11% of girls with secondary education. The same is true for poorer individuals - 28% become impregnated while only 11% of young women in wealthier households do. Furthermore, access to reproductive rights, including contraceptives, are limited, due to age and the perception of female morality. Health care providers often discuss contraception theoretically, not as a device to be used on a regular basis. Decisions concerning sexual activity often involve secrecy and taboos, as well as a lack of access to accurate information. Even more telling, young women have much easier access to maternal healthcare than they do to contraceptive help, which helps explain high pregnancy rates in the region.[50]
Rates of adolescent pregnancy in Latin America number over a million each year.[50]
Jordan
In Jordan, there is essentially no sex education in the school system; even when curriculum includes information about sexual issues, teachers are apt to skim over it, for fear of upsetting parents or being uncomfortable.[45] Youth in the country desire comprehensive, correct, and precise information from healthcare providers, although they rarely report experiencing that. Many youth equate reproductive health with maternal health, not recognizing the connections to themselves before pregnancy.[51]
Accessibility and availability of clinics in Jordan vary depending on location. Some villagers have a hard time making it to clinics, due to the high cost of transportation and the distance that must be covered. Health care centers are often overcrowded and understaffed, with limited hours of operation.[45] Youth report long wait times and unhygienic conditions at clinics.[51] Personal experiences with health care workers vary, with some youth feeling as though they received disrespectful and unfair treatment.[51]
United States
Among sexually experienced teenagers, 78% of teenage females and 85% of teenage males used contraception the first time they had sex; 86% and 93% of these same females and males, respectively, reported using contraception the last time they had sex.[52] The male condom is the most commonly used method during first sex, although 54% of young women in America rely upon the pill.[52]
Young people in the United States are no more sexually active than individuals in other developed countries, but they are significantly less knowledgeable about contraception and safe sex practices.[45] As of 2006, only twenty states required sex education in schools - of these, only ten required information about contraception.[45] On the whole, less than 10% of American students receive sex education that includes topical coverage of abortion, homosexuality, relationships, pregnancy, and STI prevention.[45] Abstinence-only education was used throughout much of the United States in the 1990s and early 2000s.[45] Based upon the moral principle that sex outside of marriage is unacceptable, the programs often misled students about their rights to have sex, the consequences, and prevention of pregnancy and STIs.[45]
According to 2006 statistics, one in three people in the U.S. will contract an STI by the age of 24 and by the age of 20, forty percent of women have been pregnant.[45] According to the Center for Disease Control, young people ages 15–24 account for 50% of all new STIs, the most prevalent being HPV and chlamydia.[53] Family planning in the United States can be expensive and often not covered by insurance plans.[45] However, effective beginning September 23, 2010, following the passage of the Affordable Care Act, preventative services, including contraception, and STI screenings and counseling, are available to all insured women with no co-pay.[54]
In 24 states legislation was passed that required women who were seeking an abortion to have an ultrasound at least 24 hours before their abortion.[55] In addition to the ultrasound requirement, several states such as Texas have passed legislation requiring facilities that provide abortions to be classified as ambulatory surgery centers, despite the very low rates of abortion complications each year.[56] Many people view this type of legislation as a way to discourage women from getting abortions.[57] The U.S. Supreme Court has struck down Texas’ most recent law that would have reduced the number of facilities able to give abortions to only eight in the state.[58]
Gender equality and violence against women
Addressing issues of gender-based violence is crucial for attaining reproductive rights. The United Nations Population Fund refers to "Equality and equity for men and women, to enable individuals to make free and informed choices in all spheres of life, free from discrimination based on gender" and "Sexual and reproductive security, including freedom from sexual violence and coercion, and the right to privacy," as part of achieving reproductive rights,[59] and states that the right to liberty and security of the person which is fundamental to reproductive rights obliges states to:[60]
- Take measures to prevent, punish and eradicate all forms of gender-based violence
- Eliminate female genital mutilation/cutting
The WHO states:[61]
- "Gender and Reproductive Rights (GRR) aims to promote and protect human rights and gender equality as they relate to sexual and reproductive health by developing strategies and mechanisms for promoting gender equity and equality and human rights in the Departments global and national activities, as well as within the functioning and priority-setting of the Department itself."
Amnesty International writes that:[62]
- Violence against women violates women's rights to life, physical and mental integrity, to the highest attainable standard of health, to freedom from torture and it violates their sexual and reproductive rights."
One key issue for achieving reproductive rights is criminalization of sexual violence. If a woman is not protected from forced sexual intercourse, she is not protected from forced pregnancy, namely pregnancy from rape. In order for a woman to be able to have reproductive rights, she must have the right to choose with whom and when to reproduce; and first of all, decide whether, when, and under what circumstances to be sexually active.[63] In many countries, these rights of women are not respected, because women do not have a choice in regard to their partner, with forced marriage and child marriage being common in parts of the world; and neither do they have any rights in regard to sexual activity, as many countries do not allow women to refuse to engage in sexual intercourse when they do not want to (because marital rape is not criminalized in those countries) or to engage in consensual sexual intercourse if they want to (because sex outside marriage is illegal in those countries). In addition to legal barriers, there are also social barriers, because in many countries a complete sexual subordination of a woman to her husband is expected (for instance, in one survey 74% of women in Mali said that a husband is justified to beat his wife if she refuses to have sex with him[64]), while sexual/romantic relations disapproved by family members, or generally sex outside marriage, can result in serious violence, such as honor killings.[65]
HIV/AIDS
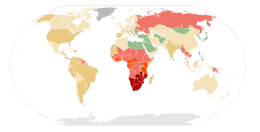
No data
<0.10
0.10–0.5
0.5–1
|
1–5
5–15
15–50
|
The WHO states that: "All women, including those with HIV, have the right “to decide freely and responsibly on the number and spacing of their children and to have access to the information, education and means to enable them to exercise these rights”".[67] The reproductive rights of people living with HIV, and their health, are very important. The link between HIV and reproductive rights exists in regard to four main issues:[67]
- prevention of unwanted pregnancy
- help to plan wanted pregnancy
- healthcare during and after pregnancy
- access to abortion services if the woman asks to
Issues
Cairo Programme of Action implementation
Implementation of the Cairo Programme of Action varies considerably from country to country. In many countries, post-ICPD tensions emerged as the human rights-based approach was implemented. Since the ICPD, many countries have broadened their reproductive health programs and attempted to integrate maternal and child health services with family planning. More attention is paid to adolescent health and the consequences of unsafe abortion. Lara Knudsen observes that the ICPD succeeded in getting feminist language into governments' and population agencies' literature, but in many countries the underlying concepts are not widely put into practice.[12] In two preparatory meetings for the ICPD+10 in Asia and Latin America, the United States, under the George W. Bush Administration, was the only nation opposing the ICPD's Programme of Action.[68]
Abortion
Lara Knudsen, a pro-choice activist, has suggested that "twenty percent of all pregnancies worldwide end in abortion, and nearly half of those abortions are unsafe and often illegal."[69] According to the WHO, more than 45 million (legal and illegal) abortions take place annually. At the same time, approximately 66,500 women die from the complications of unsafe abortion every year.[70]
An article from the World Health Organization calls safe, legal abortion a "fundamental right of women, irrespective of where they live" and unsafe abortion a "silent pandemic".[71] The article states "ending the silent pandemic of unsafe abortion is an urgent public-health and human-rights imperative." It also states "access to safe abortion improves women’s health, and vice versa, as documented in Romania during the regime of President Nicolae Ceaușescu" and "legalisation of abortion on request is a necessary but insufficient step toward improving women’s health" citing that in some countries, such as India where abortion has been legal for decades, access to competent care remains restricted because of other barriers. WHO’s Global Strategy on Reproductive Health, adopted by the World Health Assembly in May 2004, noted: “As a preventable cause of maternal mortality and morbidity, unsafe abortion must be dealt with as part of the MDG on improving maternal health and other international development goals and targets." [72] The WHO's Development and Research Training in Human Reproduction (HRP), whose research concerns people's sexual and reproductive health and lives,[73] has an overall strategy to combat unsafe abortion that comprises four inter-related activities:[72]
- to collate, synthesize and generate scientifically sound evidence on unsafe abortion prevalence and practices;
- to develop improved technologies and implement interventions to make abortion safer;
- to translate evidence into norms, tools and guidelines;
- and to assist in the development of programmes and policies that reduce unsafe abortion and improve access to safe abortion and highquality postabortion care
When negotiating the Cairo Programme of Action at the 1994 International Conference on Population and Development (ICPD), the issue was so contentious that delegates eventually decided to omit any recommendation to legalize abortion, instead advising governments to provide proper post-abortion care and to invest in programs that will decrease the number of unwanted pregnancies.[74]
On April 18, 2008 the Parliamentary Assembly of the Council of Europe, a group comprising members from 47 European countries, adopted a resolution calling for the decriminalization of abortion within reasonable gestational limits and guaranteed access to safe abortion procedures. The nonbinding resolution was passed on April 16 by a vote of 102 to 69.[75]
During and after the ICPD, some interested parties attempted to interpret the term ‘reproductive health’ in the sense that it implies abortion as a means of family planning or, indeed, a right to abortion. These interpretations, however, do not reflect the consensus reached at the Conference. For the European Union, where legislation on abortion is certainly less restrictive than elsewhere, the Council Presidency has clearly stated that the Council’s commitment to promote ‘reproductive health’ did not include the promotion of abortion.[76] Likewise, the European Commission, in response to a question from a Member of the European Parliament, clarified:
“The term ‘reproductive health’ was defined by the United Nations (UN) in 1994 at the Cairo International Conference on Population and Development. All Member States of the Union endorsed the Programme of Action adopted at Cairo. The Union has never adopted an alternative definition of ‘reproductive health’ to that given in the Programme of Action, which makes no reference to abortion.”[77]
With regard to the US, it should be noted that, only a few days prior to the Cairo Conference, the head of the US delegation, Vice President Al Gore, had stated for the record:
“Let us get a false issue off the table: the US does not seek to establish a new international right to abortion, and we do not believe that abortion should be encouraged as a method of family planning.”[78]
Some years later, the position of the US Administration in this debate was reconfirmed by US Ambassador to the UN, Ellen Sauerbrey, when she stated at a meeting of the UN Commission on the Status of Women that: “nongovernmental organizations are attempting to assert that Beijing in some way creates or contributes to the creation of an internationally recognized fundamental right to abortion”.[79] She added: “There is no fundamental right to abortion. And yet it keeps coming up largely driven by NGOs trying to hijack the term and trying to make it into a definition”.[80]
Collaborative research from the Institute of Development Studies states that "access to safe abortion is a matter of human rights, democracy and public health, and the denial of such access is a major cause of death and impairment, with significant costs to [international] development".[81] The research highlights the inequities of access to safe abortion both globally and nationally and emphasises the importance of global and national movements for reform to address this. The shift by campaigners of reproductive rights from an issue-based agenda (the right to abortion), to safe, legal abortion not only as a human right, but bound up with democratic and citizenship rights, has been an important way of reframing the abortion debate and reproductive justice agenda.[81]
Meanwhile, however the European Court of Human Rights settled the question through a landmark judgment (case of A. B. and C. v. Ireland), in which it is stated that the European Convention on Human Rights does not contain a right to abortion.
Population control
Compulsory or forced sterilizations and abortions may also occur in the context of population control policies. From the 1970s to 1980s, tension grew between women's health activists who advance women's reproductive rights as part of a human rights-based approach on the one hand, and population control advocates on the other.[82] At the 1984 UN World Population Conference in Mexico City population control policies came under attack from women's health advocates who argued that the policies' narrow focus led to coercion and decreased quality of care, and that these policies ignored the varied social and cultural contexts in which family planning was provided in developing countries. In the 1980s the HIV/AIDS epidemic forced a broader discussion of sex into the public discourse in many countries, leading to more emphasis on reproductive health issues beyond reducing fertility. The growing opposition to the narrow population control focus led to a significant departure in the early 1990s from past population control policies.[83] In the United States, abortion opponents have begun to foment conspiracy theories about reproductive rights advocates, accusing them of advancing a racist agenda of eugenics, and of trying to reduce the African American birth rate in the U.S.[84]
Sperm donation
Laws in many countries and states require sperm donors to be either anonymous or known to the recipient, or the laws restrict the number of children each donor may father. Although many donors choose to remain anonymous, new technologies such as the Internet and DNA technology have opened up new avenues for those wishing to know more about the biological father, siblings and half-siblings.
Compulsory sterilization
Roma women
During the 20th century, forced sterilization of Roma women in European countries, especially in former Communist countries, was practiced,[85][86] and there are allegations that these practices continue unofficially in some countries, such as Czech Republic, Bulgaria, Hungary and Romania.[87][88] In V. C. vs. Slovakia, the European Court for Human Rights ruled in favor of a Roma woman who was the victim of forced sterilization in a state hospital in Slovakia in 2000.[89]
United States
An individual’s sterilization is one of the main issues behind the reproductive rights that are being ignored by those who believe that they have a right to decide whether certain people are "fit" to have children. The mental stability of an individual and the physical defects that an individual might have played an important role in the beginnings of forced sterilization. Individuals were afraid that these defects were hereditary and wanted to put a stop to it before society became incompetent. Although there are numerous operations which may render one sterile, vasectomy in the male and salpingectomy in the female are considered the least radical. Neither operation is considered dangerous.[90] The laws of the states in which sterilization is practiced vary. Numerous provisions have been made both by the United States and by individual states for limiting the number of degenerates in this country. The creation of voluntary programs such as Planned Parenthood (presented the use of abstinence and contraceptives as forms of controlling the population growth) were introduced to help families control their birth rate.[91]
Sterilization has long been a controversial topic in the United States. Up through the 1970s, states could choose which women were allowed the procedure and which women were not eligible. This strategy proved repressive, both for women who wished to become sterilized and were not granted the right, as well as for women who had no choice but to become sterilized. Then, as today, sterilization was a form of birth control highly sought after by some women. However, until the 1960s, it was illegal for women to become sterilized for reasons other than eugenics, which meant sterilization as birth control was illegal. This left many women with highly legitimate reasons for sterilization unable to receive the procedure. It also meant most women who were undergoing the procedure were getting it for non-birth control reasons and not by choice.[92]
Additionally, both compulsory and coercive sterilization have become constitutional issues because some argue that it violates an individual’s ‘right to procreate’. In 1972, Eisenstadt v. Baird set the precedent: “the right of the individual, married or single, to be free from unwarranted government intrusion into matters so fundamentally affecting a person as the decision to bear or beget a child”. Yet, sterilization is still being used in court sentencing for both men and women in cases involving child abuse and/or neglect, drug abuse, and other criminal activity. The relationship between reproductive rights and sterilization is also visible in hospital settings where doctors have been documented as ordering women, namely low-income women of color, to consent to sterilization or have their birthing services withheld.[93][94][95]
Criticisms
Some opponents of legalized abortion view the term "reproductive rights" as a euphemism to sway emotions in favor of abortion. National Right to Life has referred to "reproductive rights" as a "fudge term" and "the code word for abortion rights."[96]
See also
|
References
- ↑ 1.0 1.1 1.2 1.3 Cook, Rebecca J.; Mahmoud F. Fathalla (September 1996). "Advancing Reproductive Rights Beyond Cairo and Beijing". International Family Planning Perspectives (International Family Planning Perspectives, Vol. 22, No. 3) 22 (3): 115–121. doi:10.2307/2950752. JSTOR 2950752.
- ↑ Gender and reproductive rights home page
- ↑ 3.0 3.1 3.2 Amnesty International USA (2007). "Stop Violence Against Women: Reproductive rights". SVAW. Amnesty International USA. Retrieved 2007-12-08.
- ↑ 4.0 4.1 4.2 4.3 4.4 Freedman, Lynn P.; Stephen L. Isaacs (Jan–Feb 1993). "Human Rights and Reproductive Choice". Studies in Family Planning (Studies in Family Planning, Vol. 24, No. 1) 24 (1): 18–30. doi:10.2307/2939211. JSTOR 2939211. PMID 8475521.
- ↑ Template
- ↑ 6.0 6.1 "Proclamation of Teheran". International Conference on Human Rights. 1968. Archived from the original on 2007-10-17. Retrieved 2007-11-08.
- ↑ Center for Reproductive Rights, International Legal Program, Establishing International Reproductive Rights Norms: Theory for Change, US CONG. REC. 108th CONG. 1 Sess. E2534 E2547 (Rep. Smith) (Dec. 8, 2003):
We have been leaders in bringing arguments for a woman's right to choose abortion within the rubric of international human rights. However, there is no binding hard norm that recognizes women's right to terminate a pregnancy. (...) While there are hard norms prohibiting sex discrimination that apply to girl adolescents, these are problematic since they must be applied to a substantive right (i.e., the right to health) and the substantive reproductive rights of adolescents are not `hard' (yet!). There are no hard norms on age discrimination that would protect adolescents' ability to exercise their rights to reproductive health, sexual education, or reproductive decisionmaking. In addition, there are no hard norms prohibiting discrimination based on marital status, which is often an issue with respect to unmarried adolescents' access to reproductive health services and information. The soft norms support the idea that the hard norms apply to adolescents under 18. They also fill in the substantive gaps in the hard norms with respect to reproductive health services and information as well as adolescents' reproductive autonomy. (...) There are no hard norms in international human rights law that directly address HIV/AIDS directly. At the same time, a number of human rights bodies have developed soft norms to secure rights that are rendered vulnerable by the HIV/AIDS epidemic. (...) Practices with implications for women's reproductive rights in relation to HIV/AIDS are still not fully covered under existing international law, although soft norms have addressed them to some extent. (...) There is a lack of explicit prohibition of mandatory testing of HIV-positive pregnant women under international law. (...) None of the global human rights treaties explicitly prohibit child marriage and no treaty prescribes an appropriate minimum age for marriage. The onus of specifying a minimum age at marriage rests with the states' parties to these treaties. (...) We have to rely extensively on soft norms that have evolved from the TMBs and that are contained in conference documents to assert that child marriage is a violation of fundamental human rights.
- ↑ Knudsen, Lara (2006). Reproductive Rights in a Global Context. Vanderbilt University Press. p. 1. ISBN 0-8265-1528-2.
- ↑ 9.0 9.1 "Population Matters search on "reproductive rights"". http://populationmatters.org/''. Population Matters.
- ↑ Declaration on Social Progress and Development
- ↑ 11.0 11.1 11.2 Knudsen, Lara (2006). Reproductive Rights in a Global Context. Vanderbilt University Press. pp. 5–6. ISBN 0-8265-1528-2.
- ↑ 12.0 12.1 Knudsen, Lara (2006). Reproductive Rights in a Global Context. Vanderbilt University Press. p. 7. ISBN 0-8265-1528-2.
- ↑ 13.0 13.1 United Nations, Report of the Fourth International Conference on Population and Development, Cario, 5 - 13 September 1994
- ↑ Bunch, Charlotte; Susana Fried (Autumn 1996). "Beijing '95: Moving Women's Human Rights from Margin to Center". Signs 22 (1): 200–204. doi:10.1086/495143. JSTOR 3175048.
- ↑ About the Yogyakarta Principles
- ↑ International Service for Human Rights, Majority of GA Third Committee unable to accept report on the human right to sexual education
- ↑ "The Yogyakarta Principles" Preamble and Principle 9. The Rights to Treatment with Humanity While in Detention
- ↑ United Nations General Assembly, Official Records, Third Committee, Summary record of the 29th meeting held in New York, on Monday, 25 October 2010, at 3 p.m. For instance, Malawi, speaking on behalf of all African States, argued that the Yogyakarta Principles were "controversial and unrecognized," while the representative of the Russian Federation said that they "had not been agreed to at the intergovernmental level, and which therefore could not be considered as authoritative expressions of the opinion of the international community" (para. 9, 23).
- ↑ Wilson, Teddy (2015-02-06). "A New Textbook Could Revolutionize the Way Law Students Learn About Reproductive Rights". Rhrealitycheck.org. Retrieved 2015-02-17.
- ↑ Amnesty International, Defenders of Sexual and Reproductive Rights; International Women’s Health Coalition and the United Nations, Campaign for an Inter-American Convention on Sexual and Reproductive Rights , Women's Health Collection, Abortion as a human right: possible strategies in unexplored territory. (Sexual Rights and Reproductive Rights), (2003); and Shanthi Dairiam, Applying the CEDAW Convention for the recognition of women's health rights, Arrows For Change, (2002). In this regard, the Center for Reproductive Rights has noted that:
Our goal is to ensure that governments worldwide guarantee women's reproductive rights out of an understanding that they are bound to do so. The two principal prerequisites for achieving this goal are: (1) the strengthening of international legal norms protecting reproductive rights; and (2) consistent and effective action on the part of civil society and the international community to enforce these norms. Each of these conditions, in turn, depends upon profound social change at the local, national and international (including regional) levels. (...) Ultimately, we must persuade governments to accept reproductive rights as binding norms. Again, our approach can move forward on several fronts, with interventions both at the national and international levels. Governments' recognition of reproductive rights norms may be indicated by their support for progressive language in international conference documents or by their adoption and implementation of appropriate national-level legislative and policy instruments. In order to counter opposition to an expansion of recognized reproductive rights norms, we have questioned the credibility of such reactionary yet influential international actors as the United States and the Holy See. Our activities to garner support for international protections of reproductive rights include: Lobbying government delegations at UN conferences and producing supporting analyses/materials; fostering alliances with members of civil society who may become influential on their national delegations to the UN; and preparing briefing papers and factsheets exposing the broad anti-woman agenda of our opposition.
Center for Reproductive Rights, International Legal Program, Establishing International Reproductive Rights Norms: Theory for Change, US CONG. REC. 108th CONG. 1 Sess. E2534 E2547 (Rep. Smith) (Dec. 8, 2003) - ↑ "[programme] Basis for action". Iisd.ca. Retrieved 2015-02-17.
- ↑ United Nations, Report of the Fourth International Conference on Population and Development, Cario, 5 - 13 September 1994. Guatemala entered the following reservation:
Chapter VII: we enter a reservation on the whole chapter, for the General Assembly's mandate to the Conference does not extend to the creation or formulation of rights; this reservation therefore applies to all references in the document to "reproductive rights", "sexual rights", "reproductive health", "fertility regulation", "sexual health", "individuals", "sexual education and services for minors", "abortion in all its forms", "distribution of contraceptives" and "safe motherhood"
- ↑ "Sir David Attenborough on the roots of Climatic problems". www.independent.co.uk (The Independent, UK broadsheet newspaper).
- ↑ "RoeVSWade"
- ↑ Kirk, Okazawa-Rey 2004
- ↑ Best, Kim (2006). "Men's Reproductive Health Risks: Threats to men's fertility and reproductive health include disease, cancer and exposure to toxins.". Network:Spring 1998, Vol. 18, No. 3. Family Health International. Retrieved 2008-01-02.
- ↑ McCulley Melanie G (1998). "The male abortion: the putative father's right to terminate his interests in and obligations to the unborn child". The Journal of Law and Policy VII (1): 1–55. PMID 12666677.
- ↑ Young, Kathy (Oct 19, 2000). "A man's right to choose". Salon.com. Retrieved May 10, 2011.
- ↑ Owens, Lisa Lucile, Coerced Parenthood as Family Policy: Feminism, the Moral Agency of Women, and Men's 'Right to Choose' (May 20, 2014). Alabama Civil Rights & Civil Liberties Law Review, Vol. 5, p. 1, 2013. Available at SSRN: http://ssrn.com/abstract=2439294
- ↑ Traister, Rebecca. (March 13, 2006). "Roe for men?." Salon.com. Retrieved December 17, 2007.
- ↑ The National Center For Men
- ↑ "U.S. Court of Appeals for the Sixth Circuit, case No. 06-11016" (PDF).
- ↑ Money, John; Ehrhardt, Anke A. (1972). Man & Woman Boy & Girl. Differentiation and dimorphism of gender identity from conception to maturity. USA: The Johns Hopkins University Press. ISBN 0-8018-1405-7.
- ↑ Domurat Dreger, Alice (2001). Hermaphrodites and the Medical Invention of Sex. USA: Harvard University Press. ISBN 0-674-00189-3.
- ↑ Resolution 1952/2013, Provision version, Children’s right to physical integrity, Council of Europe, 1 October 2013
- ↑ Involuntary or coerced sterilisation of intersex people in Australia, Australian Senate Community Affairs Committee, October 2013.
- ↑ It's time to defend intersex rights, Morgan Carpenter at Australian Broadcasting Corporation, 15 November 2013.
- ↑ Australian Parliament committee releases intersex rights report, Gay Star News, 28 October 2013.
- ↑ On the management of differences of sex development, Ethical issues relating to "intersexuality", Opinion No. 20/2012, Swiss National Advisory Commission on Biomedical Ethics, November 2012.
- ↑ Report of the UN Special Rapporteur on Torture, Office of the UN High Commissioner for Human Rights, February 2013.
- ↑ WHO/UN interagency statement on involuntary or coerced sterilisation, Organisation Intersex International Australia, 30 May 2014.
- ↑ Eliminating forced, coercive and otherwise involuntary sterilization, An interagency statement, World Health Organization, May 2014.
- ↑ 43.0 43.1 Mugisha, Frederick (2009). "Chapter 42: HIV and AIDS, STIs and sexual health among young people". In Furlong, Andy. Handbook of Youth and Young Adulthood. Routledge. pp. 344–352. ISBN 978-0-415-44541-2.
- ↑ 44.0 44.1 Lukale, Nelly (2012). "Sexual Reproductive Health and Rights for Young People in Africa". ARROWs for Change 18 (2): 7–8.
- ↑ 45.0 45.1 45.2 45.3 45.4 45.5 45.6 45.7 45.8 45.9 45.10 Knudson, Lara (2006). Reproductive Rights in a Global Context: South Africa, Uganda, Peru, Denmark, United States, Vietnam, Jordan. Nashville, TN: Vanderbilt University Press.
- ↑ 46.0 46.1 46.2 46.3 Irala, Jokin; Alfonso Osoria, Silvia Carlos, Cristina Lopez-del Burgo (2010). "Choice of Birth Control Methods Among European Women and the Role of Partners and Providers". Article in Press: 1–7.
- ↑ 47.0 47.1 47.2 47.3 Ketting, Evert; Esin Aysegul (2010). "Integrating Sexual and Reproductive Primary Health in Europe: Position Paper of the European Forum for Primary Care". Quality in Primary Care 18 (4): 269–282.
- ↑ Larsson, M; T. Tyden; U. Hansen; E. Haggstrom-Nordin (2007). "Contraceptive Use and Associated Factors Among Swedish High School Students". The European Journal of Contraceptive and Reproductive Health Care 12 (2): 119–124. doi:10.1080/13625180701217026.
- ↑ Ketting, Evert and Esin, Aysegul. 2010. “Integrating Sexual and Reproductive Health in Primary Health Care in Europe: Position Paper of the European Forum for Primary Care.” Quality in Primary Health 18(4): 269-282.
- ↑ 50.0 50.1 Goicolea, Isabel (2010). "Adolescent Pregnancies in the Amazon Basin of Ecuador: A Rights and Gender Approach to Adolescents' Sexual and Reproductive Health". Global Health Action 3: 1–11. doi:10.3402/gha.v3i0.5280.
- ↑ 51.0 51.1 51.2 Khalaf, Inaam; Fathieh Abu Moghli; Erika Sivarajan Froelicher (2010). "Youth Friendly Reproductive Services in Jordan from the Perspective of the Youth: A Descriptive Qualitative Study". Scandinavian Journal of Caring Sciences 24 (2): 321–331. doi:10.1111/j.1471-6712.2009.00723.x.
- ↑ 52.0 52.1 "Fact Sheet: Contraceptive Use in the United States". Guttmacher Institute. Retrieved 24 April 2013.
- ↑ "CDC Fact Sheet: Incidence, Prevalence, and Cost of Sexually Transmitted Infections in the United States" (PDF). Retrieved 24 April 2013.
- ↑ "Preventative Services Covered Under the Affordable Care Act". HealthCare.gov. Retrieved 24 April 2013.
- ↑ Angela Smith, "What Factors Lead to Abortion Restrictions?", "Washington Research Library Consortium", May 2013
- ↑
- ↑
- ↑
- ↑ "United Nations Population Fund | Supporting the Constellation of Reproductive Rights". UNFPA. Retrieved 2015-02-17.
- ↑ "United Nations Population Fund | State of World Population 2005". UNFPA. Retrieved 2015-02-17.
- ↑ "WHO | Gender and Reproductive Rights". Who.int. Retrieved 2015-02-17.
- ↑ "Sexual and reproductive rights | Amnesty International". Amnesty.org. 2007-11-06. Retrieved 2015-02-17.
- ↑ "WHO | Gender and human rights". Who.int. 2002-01-31. Retrieved 2015-02-17.
- ↑ "Bioline International Official Site (site up-dated regularly)". Bioline.org.br. 2015-02-09. Retrieved 2015-02-17.
- ↑ "Ethics: Honour Crimes". BBC. 1970-01-01. Retrieved 2015-02-17.
- ↑ "AIDSinfo". UNAIDS. Retrieved 4 March 2013.
- ↑ 67.0 67.1 "WHO | Reproductive choices for women with HIV". Who.int. Retrieved 2015-02-17.
- ↑ Knudsen, Lara (2006). Reproductive Rights in a Global Context. Vanderbilt University Press. p. 9. ISBN 0-8265-1528-2.
- ↑ Knudsen, Lara (2006). Reproductive Rights in a Global Context. Vanderbilt University Press. pp. 1–2. ISBN 0-8265-1528-2.
- ↑ According to data repeatedly published by Ipas.
- ↑ "WHO: Unsafe Abortion - The Preventable Pandemic". Retrieved 2010-01-16.
- ↑ 72.0 72.1 "WHO | Preventing unsafe abortion". Who.int. Retrieved 2015-02-17.
- ↑ "HRP | World Health Organization". Who.int. Retrieved 2015-02-17.
- ↑ Knudsen, Lara (2006). Reproductive Rights in a Global Context. Vanderbilt University Press. p. 6. ISBN 0-8265-1528-2.
- ↑ "Council of Europe Urges Member States to Decriminalize Abortion". Guttmacher.org. 2008-04-18. Retrieved 2015-02-17.
- ↑ European Parliament, 4 December 2003: Oral Question (H-0794/03) for Question Time at the part-session in December 2003 pursuant to Rule 43 of the Rules of Procedure by Dana Scallon to the Council. In the written record of that session, one reads: Posselt (PPE-DE): “Does the term ‘reproductive health’ include the promotion of abortion, yes or no?” - Antonione, Council: “No.”
- ↑ European Parliament, 24 October 2002: Question no 86 by Dana Scallon (H-0670/02)
- ↑ Jyoti Shankar Singh, Creating a New Consensus on Population (London: Earthscan, 1998), 60
- ↑ Lederer, AP/San Francisco Chronicle, 1 March 2005
- ↑ Leopold, Reuters, 28 February 2005
- ↑ 81.0 81.1 "Unsafe Abortion: A Development Issue". Institute of Development Studies (IDS) Bulletin 39 (3). July 2009.
- ↑ Knudsen, Lara (2006). Reproductive Rights in a Global Context. Vanderbilt University Press. p. 2. ISBN 0-8265-1528-2.
- ↑ Knudsen, Lara (2006). Reproductive Rights in a Global Context. Vanderbilt University Press. pp. 4–5. ISBN 0-8265-1528-2.
- ↑ Dewan, Shaila (February 26, 2010). "To Court Blacks, Foes of Abortion Make Racial Case". New York Times. Retrieved 7 June 2010.
- ↑ "Czech regret over sterilisation". BBC News. 2009-11-24. Retrieved 2015-02-17.
- ↑ http://popdev.hampshire.edu/sites/default/files/uploads/u4763/DT%2071%20Albert.pdf
- ↑ Denysenko, Marina (2007-03-12). "Europe | Sterilised Roma accuse Czechs". BBC News. Retrieved 2015-02-17.
- ↑ "Kocáb draws attention to the forced sterilization of Romani women; most recent incident allegedly took place in 2007". Romea.cz. 2009-07-21. Retrieved 2015-02-17.
- ↑ http://hudoc.echr.coe.int/sites/eng/pages/search.aspx?i=001-107364#{%22itemid%22:[%22001-107364%22]}
- ↑ Oswald, Frances (July 1930). "Eugenical Sterilization in the United States". American Journal of Sociology 36 (1): 65–73. doi:10.1086/215285.
- ↑ Dombroff, Robert M.; Harris T. Lifshitz (1972). "Overpopulation: No Strength in Numbers". Family Law Quarterly 6 (2): 93–144.
- ↑ Schoen, Johanna (2001). "Between Choice and Coercion: Women and the Politics of Sterilization in North Carolina, 1929-1975". Journal of Women's History 13 (1): 132–156. doi:10.1353/jowh.2001.0034.
- ↑ Carey, Allison C. (1998). "Gender and compulsory sterilization programs in America: 1907-1950". Journal of Historical Sociology 11 (1): 74–105. doi:10.1111/1467-6443.00054.
- ↑ Roth, Rachel (2004). "No New Babies-Gender Inequality and Reproductive Control in the Criminal Justice and Prison Systems". Am. UJ Gender Soc. Pol'y & L 12: 391.
- ↑ Blum, Erika T. (1993). "When Termination Parental Rights is Not Enough: A New Look at Compulsory Sterilization". Georgia Law Reviews 28: 977–986.
- ↑ "THE CHOICE "THAT DARE NOT SPEAK ITS NAME"". 2003.
External links
- Organizations
- The League of Women Voters on Reproductive Choice
- UNFPA Population Issues: Reproductive Rights
- American Civil Liberties Union
- Women's Global Network for Reproductive Rights Network that links grassroots organizations that are active within this topic
- Further readings
- Gebhard, Julia, Trimiño, Diana. Reproductive Rights, International Regulation, Max Planck Encyclopedia of Public International Law
- Reproductive rights cases before the European Court of Human Rights
- The Environmental Politics of Population and Overpopulation A University of California, Berkeley summary about the role of reproductive rights in the current political and ecological context
- Introductory note by Djamchid Momtaz, procedural history note and audiovisual material on the Proclamation of Teheran in the Historic Archives of the United Nations Audiovisual Library of International Law
- Murray, Melissa and Kristin Luker. Cases on Reproductive Rights and Justice. United States: Foundation Press, 2015. ISBN 978-1609304348.
| ||||||||||||||
| ||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||