Norrie disease
| Norrie disease | |
|---|---|
| Classification and external resources | |
| ICD-10 | Q15.8 |
| ICD-9 | 743.8 |
| OMIM | 310600 |
| DiseasesDB | 31165 |
Norrie disease is a genetic disorder that primarily affects the eye and almost always leads to blindness. In addition to the congenital ocular symptoms, some patients suffer from a progressive hearing loss starting mostly in their 2nd decade of life, while another portion may be mentally challenged.
Patients with Norrie disease may develop cataracts, leukocoria (a condition where the pupils appear white when light is shone on them), along with other developmental issues in the eye, such as shrinking of the globe and the wasting away of the iris.[1] Around 30 to 50% of them will also have developmental delay/mental retardation, psychotic-like features, incoordination of movements or behavioral abnormalities.[1] Most patients are born with normal hearing; however, the onset of hearing loss is very common in early adolescence.[2] About 15% of patients are estimated to develop all the features of the disease.[3]
The disease affects almost only male infants at or soon after birth, because the disease is inherited X-linked recessive. Only in very rare cases, females have been diagnosed with Norrie disease as well. The exact incidence number is unknown; only a few hundred cases have been reported. It is a very rare disorder that is not associated with any specific ethnic or racial groups.[4]
Characteristics
The most prominent symptoms of Norrie disease are ocular. The first visible finding is Leukocoria, a grayish-yellow pupillary reflex that originates from a mass of unorganized tissue behind the lens. This material, which possibly includes an already detached retina, may be confused with a tumor and thus is termed pseudoglioma.[1][4] However, an affected baby may have a normally sized eye globe and inconspicuous iris, anterior chamber, cornea and intraocular pressure.
Over the first few months of life, complete or partial retinal detachment evolves. From infancy through childhood, the patient may undergo progressive changes in the disease.[1] These progressions include the formation of cataracts, deterioration of the iris with adhesions forming between the iris and the lens or the cornea, and shallowing of the anterior chamber which may increase intraocular pressure, causing eye pain.[1] As the situation worsens, there is corneal opacification, where the cornea becomes opaque, and band keratopathy. Intraocular pressure is lost and the globe shrinks. In the last stage of Norrie disease, the globes appear small and sunken in (phthisis bulbi) and the cornea appears to be milky .[1]
Norrie disease can also have cognitive and behavioral symptoms. Developmental delay and mental retardation are present in about 30 to 50% of males who have Norrie disease.[1] Psychotic-like features and poorly characterized behavior abnormalities may also be present. Auditory symptoms are common with Norrie disease. Progressive hearing loss starts in early childhood for a majority of males with the condition. Early hearing loss is sensorineural, mild and asymmetric.[1] By adolescence, high-frequency hearing loss begins to appear. Hearing loss is severe, symmetric, and broad-spectrum by the age of 35. However, studies show that while the hearing loss is deteriorating, the ability to speak well is highly preserved.[2] The slowly progressing hearing loss is more problematic to adjust to than the congenital blindness for most people with Norrie disease.[1]
Genetics
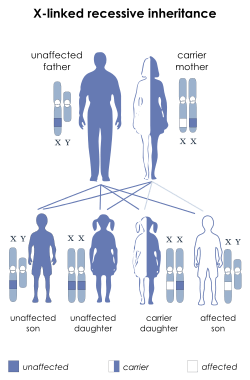
Norrie disease is a genetic disorder caused by mutations in the NDP gene, located on Xp11.4 (GeneID: 4693).[5] It is inherited in an X-linked recessive manner. This means that almost only males are affected. Sons of affected men will not have the mutation, while all of their daughters will be genetic carriers of the mutation. They also usually show no clinical symptoms, but will inherit the mutation to 50% of their offspring. Daughters receiving the mutated gene will also be, like their mother, asymptomatic carriers, but 50% of their sons will express clinical symptoms.
Females are very unlikely to express clinical signs. One possible scenario leading to this (unlikely) case would be if both of their copies of the NDP gene bear mutations, which could be the case in consanguineous families or due to a spontaneous somatic mutation. Another explanation for affected females could be skewed X-Chromosome inactivation.
However, there have been a few rare cases where females have shown symptoms associated with Norrie disease such as retinal abnormalities and mild hearing loss.[4]
The NDP Gene
A mutation in the NDP gene causes Norrie disease. The official name of the gene is "Norrie disease (pseudoglioma)", and its official symbol is NDP. The normal function of the NDP gene is to produce the instructions for creating a protein called norrin. For the normal development of the eye and other body systems, norrin is believed to be crucial.[6] Norrin also appears to be crucial in the specialization of the cells of the retina and the establishment of a blood supply to the inner ear and the tissues of the retina. The role of norrin in the specialization of retinal cells for their unique sensory is interfered by the mutation of NDP.[6] This results in an accumulation of immature retinal cells in the back of the eye. When norrin's role in the establishment of blood vessels supplying the eye is disrupted, eventually the tissues will break down.[6]
Norrin is not only important in the development of the eye. The mutation of the NDP gene can affect other systems of the body as well. The most severe problems are caused by chromosomal deletions in the region of the NDP gene, causing the prevention of the gene product, or even that of the neighboring MAO genes. When the mutations simply change a single amino acid in norrin, the effects are less widespread and severe. However, the location and type of the NDP mutation does not necessarily determine the degree of severity of the disease, since highly varying clinical signs have been diagnosed in patients carrying the exact same mutation. Therefore, the involvement of other modifying genes is very likely. On the other hand, if certain structurally important amino acids are changed (e.g. the cysteines forming the putative cystine knot), the clinical outcome has been shown to be more serious.[7]
Diagnosis
Norrie disease and other NDP related diseases are diagnosed with the combination of clinical findings and molecular genetic testing. Molecular genetic testing identifies the mutations that cause the disease in about 85% of affected males.[1] Clinical diagnoses rely on ocular findings. Norrie disease is diagnosed when grayish-yellow fibrovascular masses are found behind the eye from birth through three months. Doctors also look for progression of the disease from three months through 8–10 years of age. Some of these progressions include cataracts, iris atrophy, shallowing of anterior chamber, and shrinking of the globe.[1] By this point, people with the condition either have only light perception or no vision at all.
Molecular genetic testing is used for more than an initial diagnosis. It is used to confirm diagnostic testing, for carrier testing females, prenatal diagnosis, and preimplantation genetic diagnosis. There are three types of clinical molecular genetic testing. In approximately 85% of males, mis-sense and splice mutations of the NDP gene and partial or whole gene deletions are detected using sequence analysis.[1] Deletion/duplication analysis can be used to detect the 15% of mutations that are submicroscopic deletions. This is also used when testing for carrier females. The last testing used is linkage analysis, which is used when the first two are unavailable. Linkage analysis is also recommended for those families who have more than one member affected by the disease.[1]
History
In 1961, a Danish ophthalmologist named Mette Warburg reported about a Danish family that showed seven cases of a hereditary degenerative disease throughout seven generations. The first member of the family to be thoroughly studied was a 12-month-old boy. At the child's examination at three months, it was noticed that he was normal except that his lens appeared to be opaque and his irises were deteriorating.[8] The area behind his lens was filled with a growing yellowish mass. Five months later, his left eye was removed due to suspicion of retinoblastoma, a cancerous tumor on the retina. A histologic examination showed a hemorrhagic necrotic mass in the posterior chamber, surrounded by undifferentiated (immature, undeveloped) glial tissue. The diagnosis included a pseudotumor of the retina, hyperplasia of retinal, ciliary, and iris pigment epithelium, hypoplasia and necrosis of the inner layer of the retina, cataract, and Phthisis bulbi. This means his eye was removed because the physician suspected a tumor, although it emerged that it was a developmental defect that led to the malformation of inner parts of the eye. Because the eye was not functional, cells already began to die (necrosis) and the eye globe began to shrink due to its dysfunction (phthisi bulbi). In this Danish family, five of the seven people in these cases developed deafness later in life. Also, in four of the seven, mental capacity was determined to be low. After Warburg researched literature under various medical categories, she discovered 48 similar cases which she believed were cause by this disease as well.[8] She then suggested this disease be named after another famous Danish ophthalmologist, Gordon Norrie (1855–1941). Norrie was greatly recognized for his work with the blind and for being a surgeon at the Danish Institute for the Blind for 35 years.[9]
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 1.9 1.10 1.11 1.12 Sims, Katherine. "NDP-Related Retinopathies". GeneReviews. Retrieved 28 January 2007.
- ↑ 2.0 2.1 Halpin C, Owen G, Gutiérrez-Espeleta G, Sims K, Rehm H (2005). "Audiologic features of Norrie disease". Ann Otol Rhinol Laryngol 114 (7): 533–8. PMID 16134349.
- ↑ Dickinson JL, Sale MM, Passmore A, FitzGerald LM, Wheatley CM, Burdon KP, Craig JE, Tengtrisorn S, Carden SM, Maclean H, Mackey DA (2006). "Mutations in the NDP gene: contribution to Norrie disease, familial exudative vitreoretinopathy and retinopathy of prematurity". Clin Experiment Ophthalmol. 34 (7): 682–8. doi:10.1111/j.1442-9071.2006.01314.x. PMID 16970763.
- ↑ 4.0 4.1 4.2 "Norrie Disease". Genetics Home Reference. Retrieved 28 January 2007.
- ↑ "NDP Norrie disease (pseudoglioma) [ Homo sapiens (human) ]". Gene (National Center for Biotechnology Information). Retrieved 26 October 2013.
- ↑ 6.0 6.1 6.2 "Norrie disease (pseudoglioma)". Genetics Home Reference. U.S. National Library of Medicine. March 2008. Retrieved 18 March 2008.
- ↑ Meitinger T, Meindl A, Bork P, Rost B, Sander C, Haasemann M, Murken J (1993). "Molecular modelling of the Norrie disease protein predicts a cystine knot growth factor tertiary structure". Nature Genetics 5 (4): 376–380. doi:10.1038/ng1293-376. PMID 8298646.
- ↑ 8.0 8.1 Warburg M (1961). "Norrie's disease: a new hereditary bilateral pseudotumour of the retina". Acta Ophthal. (Copenh) 39: 757–772.
- ↑ Gordon Norrie at Who Named It?. Retrieved 13 February 2007.
External links
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||