Limb lengthening methods
Limb lengthening methods extend the length of bones (height) in disproportionately short limbs, either by the administration of growth stimulators or surgery (distraction osteogenesis). Active natural growth in humans ends in the majority of cases before 20 years of age and can, in some cases, leave disproportionately short limbs. Significant results are possible only by artificially lengthening lower extremity bone length with various construction devices .
Surgical methods may be grouped into three main categories:
- external methods;
- internal (intraosseal) methods; and
- combined (mixed) methods.
All methods generally feature:
- Bone dissection (artificial fracture). This is the location where additional length can be added.
- Artificial regeneration process, prolonged by distraction (gradual bone part separation at an average speed of 1 mm a day). The 'young' bone is stretched to a planned length, and is totally formed (ossified) only after distraction is terminated.
- muscle and tendon stretching (various methods change the stretching conditions).
General requirements for all methods:
- Stiff, solid bone fragment fixation until the moment of complete bone co-ossification («device-bone» complex).
- Gradual distraction (lengthening). In other words, creating favorable conditions for 'young bone' regeneration that takes place between stretching bone fragments.
- Sparing environment for muscles and joints during stretching and regeneration.
External methods
Characteristic features of external methods are:
- external constructions (outside the body)
- power clusters (for distraction activation) situated on the external construction
- bone fixation (creation of a common «device-bone complex») with spokes (rods) that run through the leg segment. The spoke (rod) ends are fixed in the external device
- distraction due to the separation of external device elements (increases the distance between spokes, which fixates various bone zones)
Starting in the 1960s, external compression-distraction devices gained popularity to achieve transosseous compression-distraction osteosynthesis in shin and hip lengthening. This approach was the result of device construction changes and more progressive surgical intervention methods.
Three were three common methods, involving the use of Volkov-Oganesyan [1][2] (Fig. 1.1), Gudushauri[3] (Fig. 1.2), and Ilizarov (Fig. 1.3) devices.
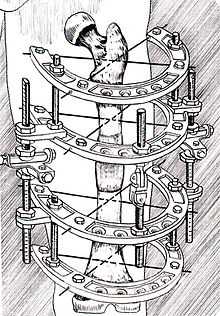 Fig. 1.1 External device by Volkov-Oganesyan |  Fig. 1.2 Variants of external devices by Gudushauri | 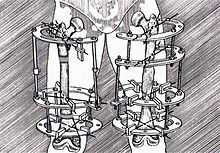 Fig. 1.3 Ilizarov compression-distraction devices |
The Ilizarov method developed by G.A. Ilizarov became widespread in many countries.[4][5][6] The Ilizarov device (see Fig. 1.3) involves an external ring clamp consisting of split rings with the fixation possibility of bars, spikes or rods. The composition of the device may vary (Fig. 1.4, Fig. 1.5) depending on the particular clinical task.[7][8]
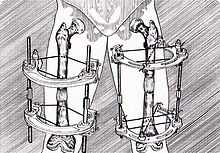 Fig. 1.4 Variants of Sivash compression-distraction devices |  Fig. 1.5 Wagner rod device: left – distraction hip osteosynthesis by Wagner; right – Wagner device is extracted, fixation by plate and screws |
Internal methods (devices)
Internal method characteristics:
- intraosseous device completes distraction and fixation functions without external constructions
- soft tissues (skin, muscles, fascia) remain intact (have no contact with the devices).
In distraction osteosynthesis using external devices the spikes overcome cut soft tissue resistance (skin, fascia, muscles) during lengthening. There is contact-conflict between multidirectional forces along the whole immersion depth of spike (spikes) into the body, causing a distraction force against the resistance force.[9] Therefore, methods without external constructions arose.[10]
Internal method with drive device
(Bliskunov, Dragan)[11][12] approach: in the early 1980s Professor Bliskunov created the method of completely closed distraction osteosynthesis; he proposed intraosseous devices for the hip. Afterwards, V. Dragan MD, DMSc invented an intraosseous device for shin (tibia) lengthening (Fig. 1.8). The particular feature of the device is the mechanical drive that activates it: 18 mechanism clicks – 1 mm (hip), 56 clicks – 1 mm for shin. (Fig. 1.7)
 Fig. 1.7 Internal drive device of Bliskunov for hip (femur) lengthening |
 Fig. 1.8 Internal drive device of Bliskunov-Dragan for shin (tibia) lengthening
(4 – fixating screws; 5 – tibia, 6 - intraosseous device; 7 – drive; 8 – growth-regeneration zone) |
The devices are made of titanium alloy and are fixated to the lengthening bones. The nail lengthens on a ratcheting principle. The device works like a lever and considerably facilitates the process of lengthening. There are two designs for the clicker. One is for the tibia (shin) and the other is for the femur (hip).
With the Bliskinov nail the patient has an opportunity to independently lengthen by him/herself. In order to lengthen the hip a patient makes a side-movement with the leg (diversion) until the mechanism is activated ("click" sound). To lengthen the shin a patient alternately presses on drive wings (the drive is situated under soft tissues and works as a pendulum). Device activation is painless. The devices provide a smooth lengthening process without harsh jerks and deleterious twisting along the bone. This approach is useful for the gradual adaptation of muscles, nerves and tendons to the newly lengthened limb.
Albizzia Method
The Albizzia method of J.-M.Guichet[13][14] was developed in 1986 and patented in 1988. The Albizzia telescopic tube device (Fig. 1.9, 1.10) consists of two tubes – one external (1) and one internal (2), connected by a ratchet mechanism that allows lengthening through rotation in one direction. Due to the ratchet mechanism, reverse rotation brings the system back into a neutral position without a loss of lengthening. The rotation angle of the inner rod is 20°; 15 back-and-forth rotations correspond to 1 mm of lengthening. The nail is made of highly resistant stainless steel allowing full weight bearing and a fast return to sport activities. A 10 cm maximal gain is possible.
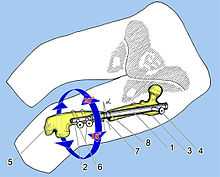 Fig. 1.9 Internal device Albizzia (1,2) for hip (femur) lengthening. Femur bone (3, 5) is fixed by screws (4, 6) |
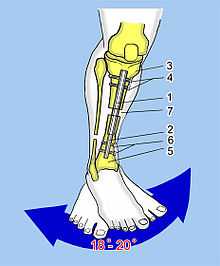 Fig. 1.10 Internal device Albizzia (1,2) for shin (tibia) lengthening. The same principle. Tibia bone (3, 5) is fixed by screws (4, 6) |
Guichet Method
The Guichet nail system is the latest evolution of the Albizzia nail. The Albizzia rotatory ratchet concept, validated on thousands of patients, has been maintained, but the system strength (nail and screws) has been greatly increased, with some parts made of chrome-cobalt. Small nails (down to a 12 cm length) allow lengthening with this device in cases of dwarfism or congenital short bones (PFFD, etc.). Specific devices exist for the femur, tibia and humerus.
The method itself is fully modified with complete control by the patient initiated in the preoperative phase (evaluation of bone and muscle quality, specific muscle and stretching training). The control of the surgery itself with minimal blood loss allows patients to resume biking on the first day after surgery, and even in some cases from 30 to 60 minutes after discharge from the operating room. The pre- and post-operative care with intensive training allows a higher speed of gain (43 mm in one month) while maintaining a full range of motion, and a higher speed of healing (healing index down to 15–20 days per cm of gain, to obtain bone fusion). Patients use standard crutches for walking, and perform gentle sports during lengthening, then weight training after bone fusion (e.g., a minimum of four months for 7 cm of gain). Gain can be stopped at any time.
ISKD device
The ISKD device (skeletal kinetic distractor)[15][16] was proposed by the Orthofix company. Its working principle resembles that of the Albizzia device. This is an intramedullary rod with mechanical distraction, created for hips (Fig. 1.11) and shins (Fig. 1.12). Its proximal and distal parts are connected inside by a thread and two one-sided clamps. In rotation from 3 to 9° these clamps are activated; 1 mm of distraction is achieved after 160 extremity rotation movements. Actual distraction length is controlled by an external manual monitor that assesses magnetic orientation in the distal part of the internal threaded rod. Patients change the distraction minimum five times a day. If the distraction length is not significant, the lower extremity is rotated under monitor control until the desired length is achieved.
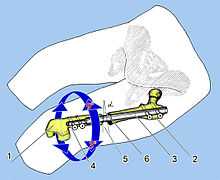 Fig. 1.11 Internal device ISKD (3, 4) for hip (femur – 1, 2) lengthening |
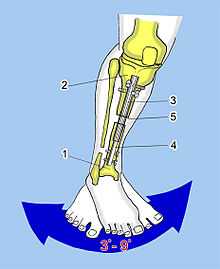 Fig. 1.12 Internal device ISKD (3, 4) for shin (tibia - 1, 2) lengthening |
Fitbon system
The Fitbon system was developed by German constructors[17][18][19] for hip (Fig. 1.13) and shin lengthening (Fig. 1.14). The peculiar feature of this method is device activation by electromagnetic impulses.
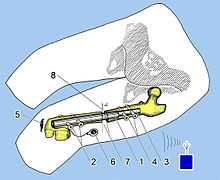 Fig. 1.13 Internal device Fitbone for hip (femur) lengthening |  Fig. 1.14 Internal device Fitbone for shin (tibia) lengthening. The same principle |
The rod consists of two parts: an external corpus (1), where a special mechanism is situated, a highly sensitive epicyclic drive (produced by Wittenstein Intens Company, which specializes in high accuracy drives), two holes for fixating screws (2), and a telescopic rod (3) with two holes for screws (4). A special electric aggregate (5 on Fig. 1.14) sends electric impulses to an antenna (receiver) (6) under the patient's skin, connected to epicyclic drive, which in turn moves a telescopic rod (3) with impulsive force up to 200 kg (600 microimpulses). According to R. Baumgart and A. Betz [23] this is enough to counteract muscle resistance during distraction.
Combined methods
Combined method characteristics:
- during the protraction period an external device is used (fixation and distraction functions);
- after lengthening, the external device is removed and a rod is implanted into the bone (providing for more stable fixation comparing to the external device).
An external device bone complex uses spikes (rods) to counteract a closed regeneration process; the «perimeter» is not closed in the spike penetration zones. External construction device cause discomfort for the patient, negative conditions for muscles and joints, and the risk of infectious complications.[20][21] Therefore, combined methods were developed which shortened the external (open) fixation time. The lengthening is provided by an external device, which is removed immediately (rods are taken off) after distraction is completed. Fixation after external device removal is provided by an intraosseous rod (osteosynthesis).
The Wasserschtein method[22][23] involved intraperiosteal osteotomy of a shin-bone in the medium one-third and of a fibula in the lower one-third; the fragments were fixated inside the bone with a flat metal rod. A Gudushauri or Ilizarov device was used as a distraction device. After lengthening was completed with a distraction speed of 2 mm per day, diastasis between bone fragments was substituted by a homocylindrical transplant with a longitudinal notch (Fig. 1.6 left).
Sanchis Olmos[24] (see Fig. 1.6 right) proposed to insert an inset separator from the patient's shin bone between bone fragments using the same lengthening method. J. Kepf[25] proposed after lengthening completion in the transosseous way to block the rod in order to exclude the rotational shifting of fragments. D. Paley[26] used simultaneously an external device (Ilizarov device, one-sided "Orthofix" device), and an intramedullary rod for hip lengthening. Authors J. E. Herzenberg and D. Paley,[27] carried out shin lengthening using the same approach (LON).
References
- ↑ Volkov M. V. Treatment of joints and bones damages by author devices/ М. V. Volkov, О. V. Oganesyan. – Tashkent : Medicine, (1978), P. 203
- ↑ Ryabzev S. L. Lower extremities lengthening in adults with simultaneous restoration of adjacent joints function by Volkov-Oganesyan devices / S. L. Ryabzev // Form and function restoration in damaged joints by Volkov-Oganesyan devices: CYTO Works Collection. – М. : CYTO Publishing House, (1982), P. 100–102
- ↑ Gudushauri О. N. Device for reposition and fixation of long tubular bones in fractures and bones lengthening/ О. N. Gudushauri // Orthopedics, traumatology and prosthetics– (1958). – # 3, P. 53–56
- ↑ Popova L. А. G/A/Ilizarov method evolution in traumatology and orthopaedics / L. А. Popova // Orthoped genius – (2006). # 4, P. 10–19
- ↑ Ilizarov G. А. Clinical possibilities of transosteous osteosynthesis method (basic practical directions)/ Ilizarov G. А., Popova L. А., Shevzov V. I. // Russian Federation Health Care. – (1986) # 9, P. 5–10
- ↑ Ilizarov G. А. Clinical and theoretical aspects of compression and distraction osteosynthesis/ G. А. Ilizarov // In the book: Theoretical and practical aspects of transosteous compression and distraction osteosynthesis. – Kurgan: Kurgan Publishers. NIIEKoT, (1976), P. 14–25
- ↑ Blachier D. Allongements progressifs du temur selon la technique de Wagner. A propos de 48 cas / D. Blachier, L. Trevonx // Rev. Chir. Orthop. – (1986),Vol. 72., P. 495–499
- ↑ Wagner H. Surgical lengthening or shortening of femur and tibia / H. Wagner // Progress in Orthopaedic Surg. (1977), Vol. 1., P. 71
- ↑ V. Klimovitskiy, V. Dragan, L.Goncharova, А. Danylyk, Abu Nemer Jamal A. M., S. Lysunov, A. Kuznetsov DISTRACTIOUS OSTEOSYNTHESIS EXTERNAL VS INTERNAL, Bulletin of Orthopaedics, Traumatology and Prosthetics, (2010), No. 3; P.59-61 ON-LINE ACCESS
- ↑ V. V. Dragan, COMPARATIVE ANALYSIS OF MODERN METHODS OF LONG BONES LENGTHENING BY INTRAMEDULLARY DEVICES. PRIORITIES OF DISTRACTION ORTHOPAEDICS. Bulletin of Orthopaedics, Traumatology and Prosthetics, (2008), No. 3; P.81-87 ON-LINE ACCESS
- ↑ V. Klimovitskiy, V. Dragan, L. Goncharova, Abu Nemer Jamal A.M., S. Lysunov, A. Kuznetsov MULTI-PAIR ELONGATION OF THE LOWER EXTREMITIES WITH THE INTRAOSTEAL DRIVE DEVICES Bulletin of Orthopaedics, Traumatology and Prosthetics, (2009), No. 3; P.44-47 ON-LINE ACCESS
- ↑ Vladimir Dragan M.D. A Short Height is as Social-Conditioned Indication for Orthopedic Correction of the Length of Lower Limbs // Таврический медико-биологический вестник.- В кн.: Труды Крымского государственного медицинского университета им. С.И.Георгиевского, - Симферополь. - (2006).- т.9.- № 1., С. 34-37. (2002) ON-LINE ACCESS
- ↑ D.A.Popkov, J.-M.Guichet, Elongation of the femur using the Albizzia intramedullary rod P.Lascombes, Genij Ortopedii 1, (2001) ON-LINE ACCESS
- ↑ Guichet J.-M., Deromendis B., Donnan L. T. Gradual femoral lengthening with the Albizzia intramedullary nail / [et al.] // J. Bone Jt Surg. – (2003) Vol. 85-A, № 5. P. 838–848
- ↑ Stefan Hankemeier, Hans-Christoph Pape, Thomas Gosling, Tobias Hufner, Martinus Richter, Christian Krettek Improved comfort in lower limb lengthening with the intramedullary skeletal kinetic distractor. Principles and preliminary clinical experiences, Arch Orthop Trauma Surg (2004) 124 : P.129–133 ON-LINE ACCESS
- ↑ Cole J. Dean The intramedullary skeletal kinetic distraction (ISKD): first clinical results of a new intramedullary nail for lengthening of the femur and tibia / Cole Dean J., Justin Daniel, Tagus Hasparis // Injury. – (2001), Vol. 32 (Suppl. 4)., P. 129–139
- ↑ Andreas H. Krieg, MD, Bernhard M. Speth, MD, and Bruce K. Foster, MBBS, MD Leg Lengthening With a Motorized Nail in Adolescents. An Alternative to External Fixators?, Clin Orthop Relat Res. (2008), January; 466(1), P. 189–197. ON-LINE ACCESS
- ↑ Baumgart R. A fully implantable motorized intramedullary nail for limb lengthening and bone transport / Baumgart R., Betz A., Schweinberer L. // Clin. Orthop. – (1997), Vol. 343., P. 135–143
- ↑ Betz A. A fully implantable intramedullary system for callus distraction – intramedullary nail with programmable drive for leg lengthening and segment displacement. Principles and initial clinical results / Betz A., Baumgart R., Schweiberer L. // Chirurgie. – (1990), Vol. 61., P. 605–609
- ↑ B. Vargas Barreto, J. Caton, Z. Merabet, J. C. Panisset and J. P. Pracros. Complications of Ilizarov leg lengthening: a comparative study between patients with leg length discrepancy and short stature, Int. Orthop. (2007) October; 31(5), P. 587–591 ON-LINE ACCESS
- ↑ B de Billy; J. Langlais; J.C. Pouliquen; J.M. Guichet and J.P. Damsin. COMPLICATIONS IN LENGTHENING OF THE FEMUR USING DIFFERENT METHODS, Journal of Bone and Joint Surgery - British Volume, Vol 87-B, Issue SUPP_I, 70., (2004) June ON-LINE ACCESS
- ↑ Wasserstein I. The Closed Distraction Epiphysiolysis. Methods and Recommendations / I. Wasserstein, T. Hawiko. – Riga, (1975), P. 1–24
- ↑ Wasserstein I. Twenty-five years experience with lengthening of shortened lower extremities using cylindrical allografs / I. Wasserstein // Clinic. Orhtoped. – (1990), Vol. 250, P. 150–154
- ↑ Sanchis Olmos Verlangerungosteotomien des Oberschenkelkels / Sanchis Olmos // Z. Orthop. – (1963) Bd. 97, № 3., P 289–296
- ↑ Kepf J. Locked intramedullary nailing. Its application to femoral and tibial axial, rotational, lengthening, and shortening osteotomic / Kepf J., Corosse A., Abalo C. // Clin. Orthop. – (1986), Vol. 212, P. 165–173
- ↑ Paley D. Femoral lengthening by simultaneous external fixation and intramedullary rodding / Paley D., Maar D., Tetsworth K. // Montaggi speciali in traumatologia e ortopedia. – Genova : (1993), P. 91–92
- ↑ Herzenberg J. E. Tibial lengthening over nails (LON) / J. E. Herzenberg, D. Paley // Tech. Orthop. – (1997), Vol. 12., P. 250–259
External links
- Guichet procedure
- Information on Bliskunov procedure
- Betz Institute
- Introduction to Distraction Osteogenesis by Dr. Martin Chin, D.D.S.
- Cosmetic Leg Lengthening
- Cosmetic and Congenital Short Stature Lengthening
- Limb Lengthening - ISKD Documents by Dr. Cole
- Vardaan Hospital describes the Ilizarov's technique