Late termination of pregnancy
Late termination of pregnancy (TOP)[1] or late-term abortions are abortions which are performed during a later stage of pregnancy. Late-term abortions are more controversial than abortion in general because the fetus is more developed and sometimes viable.
Definition
A late-term abortion often refers to an induced abortion procedure that occurs after the 20th week of gestation. The exact point when a pregnancy becomes late-term, however, is not clearly defined. Some sources define an abortion after 16 weeks as "late".[2][3] Three articles published in 1998 in the same issue of the Journal of the American Medical Association could not agree on the definition. Two of the JAMA articles chose the 20th week of gestation to be the point where an abortion procedure would be considered late-term.[4] The third JAMA article chose the third trimester, or 27th week of gestation.[5]
The point at which an abortion becomes late-term is often related to the "viability" (ability to survive outside the uterus) of the fetus. Sometimes late-term abortions are referred to as post-viability abortions. However, viability varies greatly among pregnancies. Nearly all pregnancies are viable after the 27th week, and no pregnancies are viable before the 21st week. Everything in between is a "grey area".[5]
Incidence
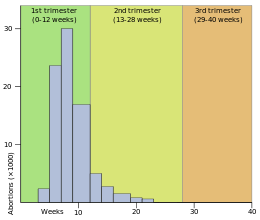
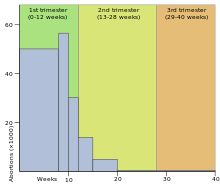
- Canada: During the year 2009, 29% of induced abortions were performed before 8 weeks, 41% at 9 to 12 weeks, 7% at 13 to 16 weeks and 2% over 21 weeks.[6]
- England and Wales: In 2005, 9% of abortions occurred between 13 and 19 weeks, while 1% occurred at or over 20 weeks.[7]
- New Zealand: In 2003, 2.03% of induced abortions were done between weeks 16 and 19, and 0.56% were done over 20 weeks.[8]
- Norway: In 2005, 2.28% of induced abortions were performed between 13 and 16 weeks, 1.24% of abortions between 17 and 20 weeks, and 0.20% over 21 weeks.[9] Between February 15, 2010 and December 1, 2011, a total number of ten abortions were performed between 22 to 24 weeks. These have been declared illegal by The Norwegian Directorate of Health.[10]
- Scotland: In 2005, 6.1% of abortions were done between 14 and 17 weeks, while 1.6% were performed over 18 weeks.[11]
- Sweden: In 2005, 5.6% of abortions were carried out between 12 and 17 weeks, and 0.8% at or greater than 18 weeks.[12]
- United States: In 2003, from data collected in those areas that sufficiently reported gestational age, it was found that 6.2% of abortions were conducted between 13 and 15 weeks, 4.2% between 16 and 20 weeks, and 1.4% at or after 21 weeks.[13] Because the Centers for Disease Control and Prevention's annual study on abortion statistics does not calculate the exact gestational age for abortions performed past the 20th week, there are no precise data for the number of abortions performed after viability.[13] In 1997, the Guttmacher Institute estimated the number of abortions in the U.S. past 24 weeks to be 0.08%, or approximately 1,032 per year.[14]
Reasons
United States
In 1987, the Alan Guttmacher Institute collected questionnaires from 1,900 women in the United States who came to clinics to have abortions. Of the 1,900 questioned, 420 had been pregnant for 16 or more weeks. These 420 women were asked to choose among a list of reasons they had not obtained the abortions earlier in their pregnancies. The results were as follows:[2]
- 71% Woman didn't recognize she was pregnant or misjudged gestation
- 48% Woman found it hard to make arrangements for abortion
- 33% Woman were afraid to tell her partner or parents
- 24% Woman took time to decide to have an abortion
- 8% Woman waited for her relationship to change
- 8% Someone pressured woman not to have abortion
- 6% Something changed after woman became pregnant
- 6% Woman didn't know timing is important
- 5% Woman didn't know she could get an abortion
- 2% A fetal problem was diagnosed late in pregnancy
- 11% Other
A new study in 2013 shows that most women seeking late term abortion "fit at least one of five profiles: They were raising children alone, were depressed or using illicit substances, were in conflict with a male partner or experiencing domestic violence, had trouble deciding and then had access problems, or were young and nulliparous."[15]
Legal restrictions
As of 1998, among the 152 most populous countries, 54 either banned abortion entirely or permitted it only to save the life of the pregnant woman.[16]
In addition, another 44 of the 152 most populous countries restricted abortions after a particular gestational age: 12 weeks (Albania, Armenia, Azerbaijan, Belarus, Bosnia-Herzegovina, Bulgaria, Croatia, Cuba, Czech Republic, Denmark, Estonia, France, Georgia, Greece, Kazakhstan, Kyrgyz Rep., Latvia, Lithuania, Macedonia, Moldova, Mongolia, Norway (additional restrictions after 18 weeks), Russian Federation, Slovakia, Slovenia, South Africa, Ukraine, Tajikistan, Tunisia, Turkey, Turkmenistan, Uzbekistan, and Yugoslavia), 13 weeks (Italy), 14 weeks (Austria, Belgium, Cambodia, Germany, Hungary, and Romania), 18 weeks (Sweden), viability (Netherlands and to some extent the United States), and 24 weeks (Singapore and Britain).[16] In these countries, abortions after the general gestational age limit are allowed only under restricted circumstances, which include, depending on country, risk to the woman's life, physical or mental health, fetal malformation, cases where the pregnancy was the result of rape, or poor socio-economic conditions. For instance, in Italy, abortion is allowed on request up until 90 days, after which it is allowed only if the pregnancy or childbirth pose a threat to the woman’s life, a risk to physical health of the woman, a risk to mental health of the woman; if there is a risk of fetal malformation; or if the pregnancy is the result of rape or other sexual crime.[17] Denmark provides a wider range of reasons, including social and economic ones, which can be invoked by a woman who seeks an abortion after 12 weeks.[18] Abortions at such stages must in general be approved by a doctor or a special committee, unlike early abortions which are performed on demand. The ease with which the doctor or the committee allows a late term abortion varies significantly by country, and is often influenced by the social and religious views prevalent in that region.
Some countries, like Canada, China (Mainland only) and Vietnam have no legal limit on when an abortion can be performed.[16]
United States
The United States Supreme Court decisions on abortion, including Roe v. Wade, allow states to impose more restrictions on post-viability abortions than during the earlier stages of pregnancy.
As of December 2014, forty-two states had bans on late-term abortions that were not facially unconstitutional under Roe v. Wade (i.e. banning all abortions) or enjoined by court order.[19] In addition, the Supreme Court in the case of Gonzales v. Carhart ruled that Congress may ban certain late-term abortion techniques, "both previability and postviability".
The Supreme Court has held that bans must include exceptions for threats to the woman's life, physical health, and mental health, but four states allow late-term abortions only when the woman's life is at risk; four allow them when the woman's life or physical health is at risk, but use a definition of health that pro-choice organizations believe is impermissibly narrow.[19] Assuming that one of these state bans is constitutionally flawed, then that does not necessarily mean that the entire ban would be struck down: "invalidating the statute entirely is not always necessary or justified, for lower courts may be able to render narrower declaratory and injunctive relief."[20]
Eighteen states prohibit abortion after a certain number of weeks' gestation (usually 22 weeks from the last menstrual period).[19] The U.S. Supreme Court held in Webster v. Reproductive Health Services that a statute may create "a presumption of viability" after a certain number of weeks, in which case the physician must be given an opportunity to rebut the presumption by performing tests.[21] Because this provision is not explicitly written into these state laws, as it was in the Missouri law examined in Webster, pro-choice organizations believe that such a state law is unconstitutional, but only "to the extent that it prohibits pre-viability abortions".[22]
Ten states (although Florida's enforcement of such laws are under permanent injunction) require a second physician to approve.[19] The U.S. Supreme Court struck down a requirement of "confirmation by two other physicians" (rather than one other physician) because "acquiescence by co-practitioners has no rational connection with a patient's needs and unduly infringes on the physician's right to practice".[23] Pro-choice organizations such as the Guttmacher Institute therefore interpret some of these state laws to be unconstitutional, based on these and other Supreme Court rulings, at least to the extent that these state laws require approval of a second or third physician.[19]
Thirteen states have laws that require a second physician to be present during late-term abortion procedures in order to treat a fetus if born alive.[19] The Court has held that a doctor's right to practice is not infringed by requiring a second physician to be present at abortions performed after viability in order to assist in the case of a living fetus.[24]
Methods
There are at least three medical procedures associated with late-term abortions:
- Dilation and evacuation (D&E)
- Early labour induction
- Intact dilation and extraction (IDX or D&X), sometimes referred to as "partial-birth abortion"
Abortions done for fetal abnormality are usually performed with induction of labor or with IDX; elective late-term abortions are usually performed with D&E. In the USA, fetal demise is usually induced by ultrasound-guided intracardiac injection of hypertonic saline, digoxin, or some other heart-stopping agent before the beginning of any late-term abortion procedure.[25] The possibility of unsuccessful feticide—resulting in birth of a live infant—is a malpractice concern.[26][27]
References
- ↑ Graham, RH; Robson, SC; Rankin, JM (January 2008). "Understanding feticide: an analytic review.". Social science & medicine (1982) 66 (2): 289–300. doi:10.1016/j.socscimed.2007.08.014. PMID 17920742.
- ↑ 2.0 2.1 Torres, Aida and Forrest, Jacqueline Darroch. (1988). Why Do Women Have Abortions. Family Planning Perspectives, 20 (4), 169-176. Retrieved April 19, 2007.
- ↑ Weihe, Pál, Steuerwald, Ulrike, Taheri, Sepideh, Færø, Odmar, Veyhe, Anna Sofía, & Nicolajsen, Did. (2003). The Human Health Programme in the Faroe Islands 1985-2001. In AMAP Greenland and the Faroe Islands 1997-2001. Danish Ministry of Environment. Retrieved April 19, 2007.
- ↑ Sprang, M.L, and Neerhof, M.G. (1998). Rationale for banning abortions late in pregnancy. Journal of the American Medical Association, 280 (8), 744-747.
Grimes, D.A. (1998). The continuing need for late abortions. Journal of the American Medical Association, 280 (8), 747-750. - ↑ 5.0 5.1 Gans Epner, J.E., Jonas, H.S., Seckinger, D.L. (1998). Late-term abortion. Journal of the American Medical Association, 280 (8), 724-729.
- ↑ Globe & Mail. (2012). Percentage distribution of induced abortions by gestation period. Retrieved December 7th, 2012.
- ↑ Government Statistical Service for the Department of Health. (July 4, 2006). Abortion statistics, England and Wales: 2005. Retrieved May 10, 2007.
- ↑ Statistics New Zealand. (January 31, 2005). Demographic Trends 2004. Retrieved April 19, 2007.
- ↑ Statistics Norway. (April 26, 2006). Induced abortions, by period of gestation and the womans age. 2005. Retrieved January 17, 2006.
- ↑ The Norwegian Directorate of Health. (May 7, 2012). Senaborter etter 22. uke Retrieved May 11, 2012.
- ↑ ISD Scotland. (May 24, 2006). Percentage of abortions performed in Scotland by estimated gestation. Retrieved May 10, 2007.
- ↑ Nilsson, E., Ollars, B., & Bennis, M.. The National Board of Health and Welfare. (May 2006). Aborter 2005. Retrieved May 10, 2007.
- ↑ 13.0 13.1 Strauss, L.T., Gamble, S.B., Parker, W.Y, Cook, D.A., Zane, S.B., & Hamdan, S. (November 24, 2006). Abortion Surveillance - United States, 2003. Morbidity and Mortality Weekly Report, 55 (11), 1-32. Retrieved May 10, 2007.
- ↑ Guttmacher Institute. (January 1997). The Limitations of U.S. Statistics on Abortion. Retrieved April 19, 2007.
- ↑ Foster, Diana (December 2013). "Who Seeks Abortions at or After 20 Weeks?". Perspectives on Sexual and Reproductive Health 45 (4): 210–218. doi:10.1363/4521013. Retrieved 9 September 2014.
- ↑ 16.0 16.1 16.2 Anika Rahman, Laura Katzive and Stanley K. Henshaw. A Global Review of Laws on Induced Abortion, 1985-1997, International Family Planning Perspectives (Volume 24, Number 2, June 1998).
- ↑ http://www.ippfen.org/NR/rdonlyres/2EB28750-BA71-43F8-AE2A-8B55A275F86C/0/Abortion_legislation_Europe_Jan2007.pdf
- ↑ http://cyber.law.harvard.edu/population/abortion/Denmark.abo.htm
- ↑ 19.0 19.1 19.2 19.3 19.4 19.5 Guttmacher Institute. (April 1, 2007). State Policies on Later-Term Abortions. State Policies in Brief. Retrieved April 19, 2007.
- ↑ Ayotte v. Planned Parenthood, 546 U.S. 320 (2006).
- ↑ Webster v. Reproductive Health Services, 492 U.S. 490 (1989).
- ↑ NARAL Pro-Choice America. (2007). "Delaware." Who Decides? The Status of Women's Reproductive Rights in the United States. Retrieved April 19, 2007.
- ↑ Doe v. Bolton, 410 U.S. 179 (1973).
- ↑ Planned Parenthood Ass'n v. Ashcroft, 462 U.S. 476, 486-90 (1983).
- ↑ http://www.societyfp.org/_documents/resources/InductionofFetalDemise.pdf
- ↑ Jansen RP (1990). "Unfinished feticide". J Med Ethics 16 (2): 61–5. doi:10.1136/jme.16.2.61. PMC 1375929. PMID 2195170.
- ↑ "Mother delivers healthy baby and lawsuit after unsuccessful abortion", Phil Trexler, Akron Beacon Journal, 2013-05-14, retrieved 2014-10-05.
External links
- Gina Gonzales as told to Barry Yeoman, "I Had An Abortion When I Was Six Months Pregnant", Glamour