Genu valgum
| Genu valgum | |
|---|---|
 | |
| Classification and external resources | |
| ICD-10 | Q74.1 |
| ICD-9 | 736.41, 755.64 |
| DiseasesDB | 29408 |
| MedlinePlus | 001263 |
| eMedicine | orthoped/495 |
Genu valgum, commonly called "knock-knee", is a condition in which the knees angle in and touch one another when the legs are straightened. Individuals with severe valgus deformities are typically unable to touch their feet together while simultaneously straightening the legs. The term originates from the Latin genu, "knee", and valgus which actually means bent outwards, but in this case, it is used to describe the distal portion of the knee joint which bends outwards and thus the proximal portion seems to be bent inwards. For citation and more information on uses of the words Valgus and Varus, please visit the internal link to -varus.
Mild genu valgum is diagnosed when a person standing upright with the feet touching also shows the knees touching. It can be seen in children from ages 2 to 5, and is often corrected naturally as children grow. However, the condition may continue or worsen with age, particularly when it is the result of a disease, such as rickets or obesity. Idiopathic genu valgum is a form that is either congenital or has no known cause.
Other systemic conditions may be associated, such as Schnyder crystalline corneal dystrophy, an autosomal dominant condition frequently reported with hyperlipidemia.
Treatment
Persons with knock knees often have collapsed inner arches of their feet, and their inner ankle bones are generally lower than their outer ankle bones. Adults with uncorrected genu valgum are typically prone to injury and chronic knee problems such as chondromalacia and osteoarthritis. These in turn can cause severe pain and problems in walking.
It is normal for children to have knock knees between the ages of two and five years of age, and almost all of them resolve as the child grows older. If symptoms are prolonged and pronounced or hereditary, doctors often use orthotic shoes or leg braces at night to gently move a child's leg back into position. If the conditions persists and worsens later in life, surgery may be required to relieve pain and complications resulting from severe or hereditary genu valgum. Available surgical procedures include adjustments to the lower femur and total knee replacement (TKR).
Weight loss and substitution of low-impact for high-impact exercise can help slow progression of the condition. With every step, the patient's weight places a distortion on the knee toward a knocked knee position, and the effect is increased with increased angle or increased weight. Even in the normal knee position, the femurs function at an angle because they connect to the hip girdle at points much further apart than they connect at the knees.
Physical therapy is generally of benefit to people with knock knees. To correct knock knees, the entire leg must be treated, especially:
- Activating and developing the arches of the feet,
- Waking up the inner leg muscles (adductors), and
- Learning how to move the inner ankle bone inwards towards the outer ankle bone, and upwards towards the knee.
Working with a physical medicine specialist such as a physiatrist, or a physiotherapist, a chiropractor or an osteopath may assist a patient learning how to improve outcomes and use the leg muscles properly to support the bone structures. Alternative or complementary treatments may include certain procedures from Iyengar Yoga or the Feldenkrais Method.
Rarely, the bone malformation underlying knock knees can be traced to a lack of nutrition necessary for bone growth, which can cause conditions such as rickets (lack of bone nutrients, especially dietary vitamin D and calcium), or scurvy (lack of vitamin C). The correction of the underlying vitamin deficiency may restore a more normal progression of bone growth.
Diagnostic test
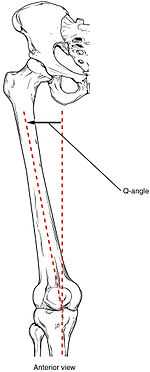
The degree of genu valgum can be estimated by the Q angle, which is the angle formed by a line drawn from the anterior superior iliac spine through the center of the patella and a line drawn from the center of the patella to the center of the tibial tubercle. In women, the Q angle should be less than 22 degrees with the knee in extension and less than 9 degrees with the knee in 90 degrees of flexion. In men, the Q angle should be less than 18 degrees with the knee in extension and less than 8 degrees with the knee in 90 degrees of flexion. A typical Q angle is 12 degrees for men and 17 degrees for women.[1]
See also
- Genu varum (bow-legs)
- Genu recurvatum (back knee)
- Knee pain
- Knee osteoarthritis
References
External links
- 1697644537 at GPnotebook
- Spencer, Samantha. "Knock knees". Boston Children's Hospital.
- Genu valgum, from Duke University's Wheeless' Textbook of Orthopaedics
- Treating knock knee - UK NHS
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||