Fencing response
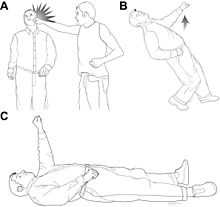
The fencing response is a peculiar position of the arms following a concussion. Immediately after moderate forces have been applied to the brainstem, the forearms are held flexed or extended (typically into the air) for a period lasting up to several seconds after the impact. The fencing response is often observed during athletic competition involving contact, such as American football, hockey, rugby and martial arts. It is used as an overt indicator of injury force magnitude and midbrain localization to aid in injury identification and classification for events including, but not limited to, on-field and/or bystander observations of sports-related head injuries.[1]
Relationship to fencing reflex and posturing
The fencing response designation arises from the similarity to the asymmetrical tonic neck reflex in infants. Like the reflex, a positive fencing response resembles the “en garde” position that initiates a fencing bout, with the extension of one arm and the flexion of the other.
Tonic posturing (see abnormal posturing) preceding convulsion has been observed in sports injuries at the moment of impact[2][3] where extension and flexion of opposite arms occur despite body position or gravity. The fencing response emerges from the separation of tonic posturing from convulsion and refines the tonic posturing phase as an immediate forearm motor response to indicate injury force magnitude and location.
Pathophysiology
The neuromotor manifestation of the fencing response resembles reflexes initiated by vestibular stimuli. Vestibular stimuli activate primitive reflexes in human infants, such as the asymmetric tonic neck reflex, Moro reflex, and parachute reflexes, which are likely mediated by vestibular nuclei in the brainstem. The lateral vestibular nucleus (LVN; Deiter’s nucleus) has descending efferent fibers in the vestibulocochlear nerve distributed to the motor nuclei of the anterior column and exerts an excitatory influence on ipsilateral limb extensor motoneurons while suppressing flexor motoneurons. The anatomical location of the LVN, adjacent to the cerebellar peduncles (see cerebellum), suggests that mechanical forces to the head may stretch the cerebellar peduncles and activate the LVN. LVN activity would manifest as limb extensor activation and flexor inhibition, defined as a fencing response, while flexion of the contralateral limb is likely mediated by crossed inhibition necessary for pattern generation.
Injury severity and sports applications
In a survey of documented head injuries followed by unconsciousness, most of which involved sporting activities, two thirds of head impacts demonstrated a fencing response,[4] indicating a high incidence of fencing in head injuries leading to unconsciousness, and those pertaining to athletic behavior. Likewise, animal models of diffuse brain injury have illustrated a fencing response upon injury at moderate but not mild levels of severity as well as a correlation between fencing, blood brain barrier disruption, and nuclear shrinkage within the LVN,[4] all of which indicates diagnostic utility of the response. The most challenging aspect to managing sport-related concussion (mild traumatic brain injury, TBI) is recognizing the injury.[5] Consensus conferences have worked toward objective criteria to identify mild TBI in the context of severe TBI.[5][6][7][8][9] However, few tools are available for distinguishing mild TBI from moderate TBI. As a result, greater emphasis has regularly been placed on the management of concussions in athletes than on the immediate identification and treatment of such an injury.[5][6] On-field predictors of injury severity can define return-to-play guidelines and urgency of care, but past criteria have either lacked sufficient incidence for effective utility,[10][11] did not directly address the severity of the injury,[12] or have become cumbersome and fraught with interrater reliability issues.[13] By providing a clear, discernible physiological event immediately upon injury, the fencing response can discern moderate brain injury forces from milder forces, providing an additional criterion by which the identification and classification of concussions can be improved, with immediate application to sport-related on-field diagnoses and decisions affecting return-to-play status for athletes, thereby facilitating the transition from diagnosis to the treatment of any post-concussion symptoms (PCS).
Further application
The fencing response may also have the potential to indicate traumatic brain injury for soldiers in military settings, specifically with regard to blast injury and subsequent shell shock. There are currently no studies or data to determine the utility of the fencing response in such an arena.
Notable fencing displays
Increased awareness of clinical significance on behalf of the bystander is critical to the utility of the fencing response designation.[14] Therefore, notable fencing displays are listed below in order to aid the bystander in identifying the various physical manifestations of the fencing response as well as demonstrating the prevalence of such a response in popular sporting and social events.
- Jahvid Best, NCAA college football running back for the California Golden Bears: Oregon State vs. California, November 7, 2009[15][16]
- Austin Collie, professional American football wide receiver for the Indianapolis Colts: Indianapolis vs. Philadelphia, November 8, 2010[17][18]
- Denarius Moore, NCAA college football wide receiver for the Tennessee Volunteers: Tennessee vs. Alabama, October 23, 2010[19][20]
- James Rodgers, NCAA college football wide receiver for the Oregon State Beavers: Oregon State vs. Boise State, September 25, 2010[21]
- Kenny Shaw, NCAA college football wide receiver for Florida State: Oklahoma vs. Florida State, September 17, 2011 [22]
- Justin McBride, professional bull rider: 2007 Glendale PBR[23]
- Ulf Samuelsson, professional hockey player: following a punch to the head by Tie Domi[24]
- Nathan Horton, professional hockey player: following a hit from Aaron Rome[25]
- James May, a television presenter: after being thrown to the ground by a taut line[26]
- Klaas-Jan Huntelaar, a professional footballer: after a collision with the English defender Chris Smalling in the friendly England–Netherlands match on February 29, 2012. He scored a goal at the same time. [27]
- Jakub Voráček, professional NHL ice hockey player for the Philadelphia Flyers: after a collision with Nicklas Kronwall of the Detroit Red Wings on March 6, 2012[28]
- Gerard Piqué, professional footballer: after a collision with FC Barcelona goalkeeper Víctor Valdés in the second leg of Champions League semifinals against Chelsea F.C. on April 24, 2012[29]
- Oscar, professional footballer: after a collision with Arsenal F.C. goalkeeper David Ospina in a Premier League fixture on April 26, 2015[30]
References
- ↑ Newton, Phil (August 28, 2009). "Youtube helps identify a new tool in the evaluation of brain injury". Psychology Today. Retrieved April 4, 2015.
- ↑ McCrory PR, Berkovic SF. Video analysis of acute motor and convulsive manifestations in sport-related concussion. Neurology. 2000;54(7):1488-91.
- ↑ McCrory PR, Bladin PF, Berkovic SF. Retrospective study of concussive convulsions in elite Australian rules and rugby league footballers; phenomenology, aetiology, and outcome. BMJ. 1997;314(7075):171-4.
- ↑ 4.0 4.1 Hosseini AH, Lifshitz J. Brain Injury Forces of Moderate Magnitude Elicit the Fencing Response. Med. Sci. Sports Exerc., 2009;41(9):1687–97.
- ↑ 5.0 5.1 5.2 Guskiewicz KM, Bruce SL, Cantu RC, et al. National Athletic Trainers’ Association position statement: management of sportrelated concussion. J Athl Train. 2004;39(3):280–97.
- ↑ 6.0 6.1 American College of Sports Medicine. Concussion (mild traumatic brain injury) and the team physician: a consensus statement. Med Sci Sports Exerc. 2006;38(2):395–9.
- ↑ Aubry M, Cantu R, Dvorak J, et al. Summary and agreement statement of the 1st International Symposium on Concussion in Sport, Vienna 2001. Clin J Sport Med. 2002;12(1):6–11.
- ↑ Cantu RC, Aubry M, Dvorak J, et al. Overview of concussion consensus statements since 2000. Neurosurg Focus. 2006;21(4):E3.
- ↑ McCrory P, Johnston K, Meeuwisse W, et al. Summary and agreement statement of the 2nd International Conference on Concussion in Sport, Prague 2004. Br J Sports Med. 2005;39(4): 196–204..
- ↑ De K Jr, Leffers P, Menheere PP, Meerhoff S, Rutten J, Twijnstra A. Prediction of post-traumatic complaints after mild traumatic brain injury: early symptoms and biochemical markers. J Neurol Neurosurg Psychiatry. 2002;73(6):727–32.,
- ↑ McCrory PR, Berkovic SF. Concussive convulsions. Incidence in sport and treatment recommendations. Sports Med. 1998;25(2): 131–6.
- ↑ Collins MW, Iverson GL, Lovell MR, McKeag DB, Norwig J, Maroon J. On-field predictors of neuropsychological and symptom deficit following sports-related concussion. Clin J Sport Med. 2003;13(4):222–9.
- ↑ Gill M, Windemuth R, Steele R, Green SM. A comparison of the Glasgow Coma Scale score to simplified alternative scores for the prediction of traumatic brain injury outcomes. Ann Emerg Med. 2005;45(1):37–42.
- ↑ "Fencing Response Awareness". Theconcussionblog.com. 2011-09-21. Retrieved 2015-04-04.
- ↑ "California RB Jahvid Best leaves game after scary fall". Sports.espn.go.com. 2009-11-08. Retrieved 2015-04-04.
- ↑ "Jahvid Best Epic Concussion (Multiple Angles)". YouTube.com. 2009-11-07. Retrieved 2015-04-04.
- ↑ "Colts’ Collie taken off field on stretcher - NFL.com". Blogs.nfl.com. 2010-11-07. Retrieved 2015-04-04.
- ↑ "Austin Collie Big Hit". YouTube.com. 2010-11-07. Retrieved 2015-04-04.
- ↑
- ↑ "Denarius Moore leveled by DeMarcus Milliner". YouTube.com. 2010-10-23. Retrieved 2015-04-04.
- ↑ "Boise State Vs. Oregon State: James Rodgers Blindsided, Hits Ground And Stays Down". SBNation.com. 2010-09-25. Retrieved 2015-04-04.
- ↑ "FSU's Kenny Shaw OK after being knocked unconscious". Orlandosentinel.com. Retrieved 2015-04-04.
- ↑ "Justin McBride Concussion". YouTube.com. 2007-07-14. Retrieved 2015-04-04.
- ↑ "Domi KO's Ulf 95-96". YouTube.com. 2009-02-20. Retrieved 2015-04-04.
- ↑ "YouTube". YouTube.com. Retrieved 2015-04-04.
- ↑ "James May hurt during Top Gear stunt". Telegraph.co.uk. 2010-12-23. Retrieved 2015-04-04.
- ↑ Metcalfe, Nick (2012-03-01). "Chris Smalling injury: In hospital after clashing heads with Klaas-Jan Huntelaar at Wembley | Daily Mail Online". Dailymail.co.uk. Retrieved 2015-04-04.
- ↑ Wyshynski, Greg (2012-03-06). "Witness Niklas Kronwall’s devastating hit on Jakub Voracek in Red Wings vs. Flyers (VIDEO) | Puck Daddy - Yahoo Sports". Sports.yahoo.com. Retrieved 2015-04-04.
- ↑ "Piqué given all-clear after clash with Valdes". BuenosAiresHerald.com. 2012-04-24. Retrieved 2015-04-04.
- ↑ "Oscar headed to hospital after thunderous clash with Ospina". BuenosAiresHerald.com. 2015-04-26. Retrieved 2015-04-26.