Endometriosis
| Endometriosis | |
|---|---|
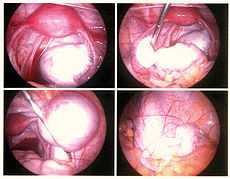 Endometriosis as seen during laparoscopic surgery | |
| Classification and external resources | |
| ICD-10 | N80 |
| ICD-9 | 617.0 |
| OMIM | 131200 |
| DiseasesDB | 4269 |
| MedlinePlus | 000915 |
| eMedicine | med/3419 ped/677 emerg/165 |
| Patient UK | Endometriosis |
| MeSH | D004715 |
Endometriosis is a disease in which tissue that normally grows inside the uterus grows outside the uterus.[1] Its main symptoms are pelvic pain and infertility. Nearly half have chronic pelvic pain while in 70% pain occurs during menstruation. Pain with sex is also common. Infertility occurs in up to half of people.[2] Endometriosis can have both social and psychological effects.[3] Less common symptoms include urinary or bowel symptoms. About 25% of women have no symptoms.[2]
The cause is not entirely clear.[2] Risk factors include having a family history of the condition. Most often the ovaries, fallopian tubes, and tissue around the uterus are affected; however, in rare cases it may also occur in other parts of the body.[4] The areas of endometriosis bleed each month which results in inflammation and scarring.[2][4] The growths due to endometriosis are not cancer. Diagnosis is usually based on symptom in combination with medical imaging. Biopsy is the most sure method of diagnosis.[4] Other causes of similar symptoms include: irritable bowel syndrome, interstitial cystitis, and fibromyalgia.[2]
Tentative evidence suggests that the use of combined oral contraceptives reduces the risk of endometriosis.[5] Exercise and avoiding large amount of alcohol may also be preventative.[4] There is no cure for endometriosis, but a number of treatments may improve symptoms.[2] This may include pain medication, hormonal treatments, or surgery. The recommended pain medication is usually an NSAID such as naproxen. Taking the active component of the birth control pill continuously or an intrauterine device with progestogen may also be useful. Gonadotropin-releasing hormone agonist may improve the ability of those who are infertile to get pregnant. Surgical removal of endometriosis may be done in those whose symptoms are not manageable with other treatment.[4]
Endometriosis is estimated to occur in roughly 6–10% of women.[2] It is most common in those in their thirties and forties.[4] It results in few deaths with this being estimated at 200 globally in 2013.[6] Endometriosis was first determined to be a separate condition in the 1920s. Before that time endometriosis and adenomyosis were considered together. It is unclear who first described the disease.[7]
Signs and symptoms

Although 20–25% of people with endometriosis have no symptoms, pain and infertility are the most common signs.[2]
Pelvic pain
A major symptom of endometriosis is recurring pelvic pain. The pain can range from mild to severe cramping or stabbing pain that occurs on both sides of the pelvis, in the lower back and rectal area, and even down the legs. The amount of pain a woman feels correlates poorly with the extent or stage (1 through 4) of endometriosis, with some women having little or no pain despite having extensive endometriosis or endometriosis with scarring, while other women may have severe pain even though they have only a few small areas of endometriosis.[8] Symptoms of endometriosis-related pain may include:[9]
- dysmenorrhea – painful, sometimes disabling cramps during the menstrual period; pain may get worse over time (progressive pain), also lower back pains linked to the pelvis
- chronic pelvic pain – typically accompanied by lower back pain or abdominal pain
- dyspareunia – painful sex
- dysuria – urinary urgency, frequency, and sometimes painful voiding
Throbbing, gnawing, and dragging pain to the legs are reported more commonly by women with endometriosis.[10] Compared with women with superficial endometriosis, those with deep disease appear to be more likely to report shooting rectal pain and a sense of their insides being pulled down.[10] Individual pain areas and pain intensity appears to be unrelated to the surgical diagnosis, and the area of pain unrelated to area of endometriosis.[10]
Endometriosis lesions react to hormonal stimulation and may "bleed" at the time of menstruation. The blood accumulates locally, causes swelling, and triggers inflammatory responses with the activation of cytokines. This process may cause pain. Pain can also occur from adhesions (internal scar tissue) binding internal organs to each other, causing organ dislocation. Fallopian tubes, ovaries, the uterus, the bowels, and the bladder can be bound together in ways that are painful on a daily basis, not just during menstrual periods.[11]
Also, endometriotic lesions can develop their own nerve supply, thereby creating a direct and two-way interaction between lesions and the central nervous system, potentially producing a variety of individual differences in pain that can, in some women, become independent of the disease itself.[8]
Infertility
Many women with infertility may have endometriosis. Among women with endometriosis, 30–50% may experience infertility.[12]
Other
Other symptoms include diarrhea or constipation,[10] chronic fatigue, nausea and vomiting, headaches, low-grade fevers, heavy and/or irregular periods, and hypoglycemia.[13]
In addition to pain during menstruation, the pain of endometriosis can occur at other times of the month. There can be pain with ovulation, pain associated with adhesions, pain caused by inflammation in the pelvic cavity, pain during bowel movements and urination, during general bodily movement like exercise, pain from standing or walking, and pain with intercourse. But the most desperate pain is usually with menstruation and many women dread having their periods. Pain can also start a week before a menstrual period, during and even a week after a menstrual period, or it can be constant. The pain can be debilitating and the emotional stress can take a toll.[14]
There is an association between endometriosis and certain types of cancers, notably some types of ovarian cancer,[15][16] non-Hodgkin's lymphoma and brain cancer.[17] Despite similarities in their name and location, endometriosis bears no relationship to endometrial cancer.[18]
Endometriosis often also coexists with leiomyoma or adenomyosis, but studies that look into similarities and differences between endometriosis and adenomyosis have conflicting results.[19]
Risk factors
Genetics
Genetic predisposition plays a role in endometriosis.[20] Daughters or sisters of women with endometriosis are at higher risk of developing endometriosis themselves; low progesterone levels may be genetic, and may contribute to a hormone imbalance.[21] There is an about six-fold increased incidence in women with an affected first-degree relative.[22]
It has been proposed that endometriosis results from a series of multiple hits within target genes, in a mechanism similar to the development of cancer.[20] In this case, the initial mutation may be either somatic or heritable.[20]
Individual genomic changes (found by genotyping including genome-wide association studies) that have been associated with endometriosis include:
- Changes on chromosome 1 near WNT4.[23]
- Changes on chromosome 2 near GREB1.[23]
- Changes on chromosome 6 near ID4.[23]
- Changes on chromosome 7 in the 7p15.2 region.[23][24]
- Changes on chromosome 9 near CDKN2BAS.[23]
- Changes on chromosome 10 at region 10q26.[25]
- Changes on chromosome 12 near VEZT.[23]
In addition, there is a weaker association with changes in the fibronectin gene as well as in the 2p14 region of chromosome 2.[23]
In addition, there are many findings of altered gene expression and epigenetics, but both of these can also be a secondary result of, for example, environmental factors and altered metabolism. Examples of altered gene expression include that of miRNAs.[20]
Environmental toxins
Several studies have investigated the potential link between exposure to dioxins and endometriosis, but the evidence is equivocal and potential mechanisms are poorly understood.[26] A 2004 review of studies of dioxin and endometriosis concluded that "the human data supporting the dioxin-endometriosis association are scanty and conflicting",[27] and a 2009 follow-up review also found that there was "insufficient evidence" in support of a link between dioxin exposure and women developing endometriosis.[28] A 2008 review concluded that more work was needed, stating that "although preliminary work suggests a potential involvement of exposure to dioxins in the pathogenesis of endometriosis, much work remains to clearly define cause and effect and to understand the potential mechanism of toxicity".[29]
Pathophysiology

While the exact cause of endometriosis remains unknown, many theories have been presented to better understand and explain its development. These concepts do not necessarily exclude each other. The pathophysiology of endometriosis is likely to be multifactorial and to involve an interplay between several factors.[20]
Broadly, the aspects of the pathophysiology can basically be classified as underlying predisposing factors, inflammation, metabolic changes, formation of ectopic endometrium, and generation of pain and other effects. It is not certain, however, to what degree predisposing factors lead to metabolic and inflammatory changes and so on, or if metabolic and inflammatory changes or formation of ectopic endometrium is the primary cause. Also, there are several theories within each category, but the uncertainty over what is a cause versus what is an effect when considered in relation to other aspects is as true for any individual entry in the pathophysiology of endometriosis.[20] Inflammation is a central part of the aetiopathology and causes pain.[30] Also, pathogenic mechanisms appear to differ in the formation of distinct types of endometriotic lesion, such as peritoneal, ovarian and rectovaginal lesions.[20]
Formation
The main theories for the formation of ectopic endometrium are retrograde menstruation, müllerianosis, coelomic metaplasia and transplantation, each further described below.
Retrograde menstruation
The theory of retrograde menstruation (also called the implantation theory or transplantation theory)[31] is the most widely accepted theory for the formation of ectopic endometrium in endometriosis.[20] It suggests that during a woman's menstrual flow, some of the endometrial debris exits the uterus through the fallopian tubes and attaches itself to the peritoneal surface (the lining of the abdominal cavity) where it can proceed to invade the tissue as endometriosis.[20]
While most women may have some retrograde menstrual flow, typically their immune system is able to clear the debris and prevent implantation and growth of cells from this occurrence. However, in some women, endometrial tissue transplanted by retrograde menstruation may be able to implant and establish itself as endometriosis. Factors that might cause the tissue to grow in some women but not in others need to be studied, and some of the possible causes below may provide some explanation, e.g., hereditary factors, toxins, or a compromised immune system. It can be argued that the uninterrupted occurrence of regular menstruation month after month for decades is a modern phenomenon, as in the past women had more frequent menstrual rest due to malnutrition, pregnancy, and lactation.
Retrograde menstruation alone is not able to explain all instances of endometriosis, and it needs additional factors such as genetic or immune differences to account for the fact that many women with retrograde menstruation do not have endometriosis. Research is focusing on the possibility that the immune system may not be able to cope with the cyclic onslaught of retrograde menstrual fluid. In this context there is interest in studying the relationship of endometriosis to autoimmune disease, allergic reactions, and the impact of toxins.[32][33] It is still unclear what, if any, causal relationship exists between toxins, autoimmune disease, and endometriosis. There are immune system changes in women with endometriosis, such as an increase macrophage-derived secretion products, but it is unknown if these are contributing to the disorder or are reactions from it.[34]
In addition, at least one study found that endometriotic lesions are biochemically very different from artificially transplanted ectopic tissue.[35] The latter finding, however, can in turn be explained by that the cells that establish endometrial lesions are not of the main cell type in ordinary endometrium, but rather of a side population cell type, as supported by exhibitition of a side population phenotype upon staining with Hoechst dye and by flow cytometry.[20] Similarly, there are changes in for example the mesothelium of the peritoneum in women with endometriosis, such as loss of tight junctions, but it is unknown if these are causes or effects of the disorder.[34]
In rare cases where imperforate hymen does not resolve itself prior to the first menstrual cycle and goes undetected, blood and endometrium are trapped within the uterus of the woman until such time as the problem is resolved by surgical incision. Many health care practitioners never encounter this defect, and due to the flu-like symptoms it is often misdiagnosed or overlooked until multiple menstrual cycles have passed. By the time a correct diagnosis has been made, endometrium and other fluids have filled the uterus and fallopian tubes with results similar to retrograde menstruation resulting in endometriosis. The initial stage of endometriosis may vary based on the time elapsed between onset and surgical procedure.
The theory of retrograde menstruation as a cause of endometriosis was first proposed by John A. Sampson.
Other theories
- Müllerianosis: A competing theory states that cells with the potential to become endometrial are laid down in tracts during embryonic development and organogenesis. These tracts follow the female reproductive (Mullerian) tract as it migrates caudally (downward) at 8–10 weeks of embryonic life. Primitive endometrial cells become dislocated from the migrating uterus and act like seeds or stem cells. This theory is supported by foetal autopsy.[36]
- Coelomic metaplasia: This theory is based on the fact that coelomic epithelium is the common ancestor of endometrial and peritoneal cells and hypothesizes that later metaplasia (transformation) from one type of cell to the other is possible, perhaps triggered by inflammation.[37]
- Vasculogenesis: Up to 37% of the microvascular endothelium of ectopic endometrial tissue originates from endothelial progenitor cells, which result in de novo formation of microvessels by the process of vasculogenesis rather than the conventional process of angiogenesis.[38]
- Neural growth: An increased expression of new nerve fibres is found in endometriosis, but does not fully explain the formation of ectopic endometrial tissue, and is not definitely correlated with the amount of perceived pain.[39]
Localization

Most endometriosis is found on these structures in the pelvic cavity: [40]
- Ovaries (the most common site)
- Fallopian tubes
- The back of the uterus and the posterior cul-de-sac
- The front of the uterus and the anterior cul-de-sac
- Uterine ligaments such as the broad or round ligament of the uterus
- Pelvic and back wall
- Intestines, most commonly the rectosigmoid
- Urinary bladder and ureters
Rectovaginal or bowel endometriosis affects approximately 5-12% of women with endometriosis, and can cause severe pain with bowel movements.[41]
Endometriosis may spread to the cervix and vagina or to sites of a surgical abdominal incision, known as "scar endometriosis."[42] Risk factors for scar endometriosis include previous abdominal surgeries, such as a hysterotomy or cesarean section, or ectopic pregnancies, salpingostomy puerperal sterilization, laparoscopy, amniocentesis, appendectomy, episiotomy, vaginal hysterectomies, and hernia repair.[43][44][45]
Endometriosis may also present with skin lesions in cutaneous endometriosis.
Less commonly lesions can be found on the diaphragm. Diaphragmatic endometriosis is rare, almost always on the right hemidiaphragm, and may inflict cyclic pain of the right shoulder just before and during a menstrual period. Rarely, endometriosis can be extraperitoneal and is found in the lungs and CNS.[46]
Diagnosis

A health history and a physical examination can lead the health care practitioner to suspect endometriosis. Although doctors can often feel the endometrial growths during a pelvic exam, and these symptoms may be signs of endometriosis, diagnosis cannot be confirmed by exam only. Use of pelvic ultrasound may identify large endometriotic cysts (called endometriomas). However, smaller endometriosis implants cannot be visualized with ultrasound technique.
Laparoscopy

Laparoscopy, a surgical procedure where a camera is used to look inside the abdominal cavity, is the only way to officially diagnose endometriosis as it permits lesion visualization, unless the lesion is visible externally, e.g. an endometriotic nodule in the vagina. If the growths are not visible, a biopsy may be taken to determine the diagnosis.[47] Surgery for diagnoses also allows for surgical treatment of endometriosis at the same time.
To the eye, lesions can appear dark blue, powder-burn black, red, white, yellow, brown or non-pigmented. Lesions vary in size. Some within the pelvis walls may not be visible, as normal-appearing peritoneum of infertile women reveals endometriosis on biopsy in 6–13% of cases.[48] Early endometriosis typically occurs on the surfaces of organs in the pelvic and intra-abdominal areas. Health care providers may call areas of endometriosis by different names, such as implants, lesions, or nodules. Larger lesions may be seen within the ovaries as endometriomas or "chocolate cysts", "chocolate" because they contain a thick brownish fluid, mostly old blood.
Frequently during diagnostic laparoscopy, no lesions are found in women with chronic pelvic pain, a symptom common to other disorders including adenomyosis, pelvic adhesions, pelvic inflammatory disease, congenital anomalies of the reproductive tract, and ovarian or tubal masses.[49]
Staging
Surgically, endometriosis can be staged I–IV (Revised Classification of the American Society of Reproductive Medicine).[50] The process is a complex point system that assesses lesions and adhesions in the pelvic organs, but it is important to note staging assesses physical disease only, not the level of pain or infertility. A person with Stage I endometriosis may have little disease and severe pain, while a person with Stage IV endometriosis may have severe disease and no pain or vice versa. In principle the various stages show these findings:
- Stage I (Minimal)
- Findings restricted to only superficial lesions and possibly a few filmy adhesions
- Stage II (Mild)
- In addition, some deep lesions are present in the cul-de-sac
- Stage III (Moderate)
- As above, plus presence of endometriomas on the ovary and more adhesions.
- Stage IV (Severe)
- As above, plus large endometriomas, extensive adhesions.
Endometrioma on the ovary of any significant size (Approx. 2 cm +) must be removed surgically because hormonal treatment alone will not remove the full endometrioma cyst, which can progress to acute pain from the rupturing of the cyst and internal bleeding. Endometrioma is sometimes misdiagnosed as ovarian cysts.
Markers
An area of research is the search for endometriosis markers.[51]
A systematic review in 2010 of essentially all proposed biomarkers for endometriosis in serum, plasma and urine came to the conclusion that none of them have been clearly shown to be of clinical use, although some appear to be promising.[51] Another review in 2011 identified several putative biomarkers upon biopsy, including findings of small sensory nerve fibers or defectively expressed β3 integrin subunit.[52]
The one biomarker that has been used in clinical practice over the last 20 years is CA-125.[51] However, its performance in diagnosing endometriosis is low, even though it shows some promise in detecting more severe disease.[51] CA-125 levels appear to fall during endometriosis treatment, but has not shown a correlation with disease response.[51]
It has been postulated a future diagnostic tool for endometriosis will consist of a panel of several specific and sensitive biomarkers, including both substance concentrations and genetic predisposition.[51]
Histopathology



Typical endometriotic lesions show histopathologic features similar to endometrium, namely endometrial stroma, endometrial epithelium, and glands that respond to hormonal stimuli. Older lesions may display no glands but hemosiderindeposits (see photomicrograph on right) as residual.
Immunohistochemistry has been found to be useful in diagnosing endometriosis as stromal cells have a peculiar surface antigen, CD10, thus allowing the pathologist go straight to a staining area and hence confirm the presence of stromal cells and sometimes glandular tissue is thus identified that was missed on routine H&E staining.[53]
Pain quantification
The most common pain scale for quantification of endometriosis-related pain is the visual analogue scale (VAS); VAS and numerical rating scale (NRS) were the best adapted pain scales for pain measurement in endometriosis. For research purposes, and for more detailed pain measurement in clinical practice, VAS or NRS for each type of typical pain related to endometriosis (dysmenorrhea, deep dyspareunia and non-menstrual chronic pelvic pain), combined with the clinical global impression (CGI) and a quality of life scale, are used.[54]
Methods of limited use
In order to avoid invasive diagnosis and potentially life-threatening complications of laparoscopy, the response to hormonal agonists such as Lupron has been advocated as a possible method for diagnosing endometriosis, under the premise that if the chronic pelvic pain was reduced or relieved with Lupron, the diagnosis would be established.[49] However, a randomized controlled trial investigating pain relief in response to Lupron administration found that pain relief was not significantly different in women who did or did not have endometriosis as detected by laparoscopy.[55] Thus, response to Lupron is currently not an accurate diagnostic method for detecting endometriosis, and the only definitive measure for diagnosis is laparoscopy.
Prevention
Limited evidence indicates that the use of combined oral contraceptives is associated with a reduced risk of endometriosis.[5]
Management
While there is no cure for endometriosis, there are two types of interventions; treatment of pain and treatment of endometriosis-associated infertility.[56] In many women menopause (natural or surgical) will abate the process.[57] In women in the reproductive years, endometriosis is merely managed: the goal is to provide pain relief, to restrict progression of the process, and to restore or preserve fertility where needed. In younger women with unfulfilled reproductive potential, surgical treatment attempts to remove endometrial tissue and preserve the ovaries without damaging normal tissue.[58]
In general, the diagnosis of endometriosis is confirmed during surgery, at which time ablative steps can be taken. Further steps depend on circumstances: a woman without infertility can be managed with hormonal medication that suppress the natural cycle and pain medication, while an infertile woman may be treated expectantly after surgery, with fertility medication, or with IVF. As to the surgical procedure, ablation (or fulguration) of endometriosis (burning and vaporizing the lesions with an electric device) has shown high rate of short-term recurrence after the procedure. The best surgical procedure with much less rate of short-term recurrence is to excise (cut and remove) the lesions completely.
Surgery
Conservative treatment consists of the excision of the endometrium, adhesions, resection of endometriomas, and restoration of normal pelvic anatomy as much as is possible.[59] Laparoscopy, besides being used for diagnosis, can also be used to perform surgery. It's considered a "minimally invasive" surgery because the surgeon makes very small openings (incisions) at (or around) the belly button and lower portion of the belly. A thin telescope-like instrument (the laparoscope) is placed into one incision, which allows the doctor to look for endometriosis using a small camera attached to the laparoscope. Small instruments are inserted through the incisions to remove the endometriosis tissue and adhesions. Because the incisions are very small, there will only be small scars on the skin after the procedure, and all endometriosis can be removed, and women recover from surgery quicker and have a lower risk of adhesions.[60] 55% to 100% of women develop adhesions following pelvic surgery,[61] which can result in infertility, chronic abdominal and pelvic pain, and difficult reoperative surgery. Trehan's temporary ovarian suspension, a technique in which the ovaries are suspended for a week after surgery may be used to reduce the incidence of adhesions after endometriosis surgery.[62][63]
Conservative treatment involves excision of endometriosis while preserving the ovaries and uterus, very important for women wishing to conceive, but may increase the risk of recurrence.[64]
Endometriosis recurrence following conservative surgery is estimated as 21.5% at 2 years and 40-50% at 5 years.[65]
A hysterectomy (removal of the uterus) can be used to treat endometriosis in women who do not wish to conceive. However, this should only be done when combined with removal of the endometriosis by excision, as if endometriosis is not also removed at the time of hysterectomy, pain may persist.[66]
For women with extreme pain, a presacral neurectomy may be very rarely performed where the nerves to the uterus are cut. However, this technique is almost never used due to the high incidence of associated complications including presacral haematoma and irreversible problems with urination and constipation.[66]
Hormones
- Progesterone or Progestins: Progesterone counteracts estrogen and inhibits the growth of the endometrium.[67] Such therapy can reduce or eliminate menstruation in a controlled and reversible fashion. Progestins are chemical variants of natural progesterone. An example of a Progestin is Dienogest (Visanne).
- Avoiding products with xenoestrogens, which have a similar effect to naturally produced estrogen and can increase growth of the endometrium.
- Hormone contraception therapy: Oral contraceptives reduce the menstrual pain associated with endometriosis.[68] They may function by reducing or eliminating menstrual flow and providing estrogen support. Typically, it is a long-term approach.
- Danazol (Danocrine) and gestrinone are suppressive steroids with some androgenic activity.[58] Both agents inhibit the growth of endometriosis but their use remains limited as they may cause hirsutism and voice changes.
- Gonadotropin Releasing Hormone (GnRH) agonist:[58] These agents work by increasing the levels of GnRH. Consistent stimulation of the GnRH receptors results in downregulation, inducing a profound hypoestrogenism by decreasing FSH and LH levels. While effective in some people, they induce unpleasant menopausal symptoms, and over time may lead to osteoporosis. To counteract such side effects some estrogen may have to be given back (add-back therapy). These drugs can only be used for six months at a time.
- Lupron depo shot is a GnRH agonist and is used to lower the hormone levels in the woman's body to prevent or reduce growth of endometriosis. Symptoms will mostly come back after completing the Lupron courses. Long-term use of Lupron (over five to six months) is associated with severe side effects, and should not be offered to the women. Thus, Lupron is not considered a treatment option for endometriosis. Instead, it is widely used in the United States as the non-invasive method for the diagnosis of endometriosis.
- Aromatase inhibitors are medications that block the formation of estrogen and have become of interest for researchers who are treating endometriosis.[69]
Other medication
- NSAIDs: Anti-inflammatory. They are commonly used in conjunction with other therapy. For more severe cases narcotic prescription drugs may be used. NSAID injections can be helpful for severe pain or if stomach pain prevents oral NSAID use.
- Opioids: Morphine sulphate tablets and other opioid painkillers work by mimicking the action of naturally occurring pain-reducing chemicals called "endorphins". There are different long acting and short acting medications that can be used alone or in combination to provide appropriate pain control.
- Following laparoscopic surgery women who were given Chinese herbs were reported to have comparable benefits to women with conventional drug treatments, though the journal article that reviewed this study also noted that "the two trials included in this review are of poor methodological quality so these findings must be interpreted cautiously. Better quality randomised controlled trials are needed to investigate a possible role for CHM [Chinese Herbal Medicine] in the treatment of endometriosis.",[70]
- Pentoxifylline, an immunomodulating agent, has been theorized to improve pain as well as improve pregnancy rates in women with endometriosis. A 2012 Cochrane review; however, enough evidence to support either of these uses.[71] Current American Congress of Obstetricians and Gynecologists (ACOG) guidelines do not include immune-modulators, such as pentoxifylline, in standard treatment protocols.[72]
- Angiogenesis inhibitors lack clinical evidence of efficacy in endometriosis therapy.[73] Under experimental in vitro and in vivo conditions, compounds that have been shown to exert inhibitory effects on endometriotic lesions include growth factor inhibitors, endogenous angiogenesis inhibitors, fumagillin analogues, statins, cyclo-oxygenase-2 inhibitors, phytochemical compounds, immunomodulators, dopamine agonists, peroxisome proliferator-activated receptor agonists, progestins, danazol and gonadotropin-releasing hormone agonists.[73] However, many of these agents are associated with undesirable side effects and more research is necessary. An ideal therapy would diminish inflammation and underlying symptoms without being contraceptive.[74][75]
The overall effectiveness of manual physical therapy to treat endometriosis has not yet been identified.[76] There is no evidence to support nutritional therapy as effective.
Comparison of interventions
Medicinal and surgical interventions produce roughly equivalent pain-relief benefits. Recurrence of pain was found to be 44 and 53 percent with medicinal and surgical interventions, respectively.[21] Each approach has advantages and disadvantages.[37] Manual therapy showed a decrease in pain for 84 percent of study participants, and a 93 percent improvement in sexual function.[77]
Evidence on how effective medication is for relieving pain associated with endometriosis is limited.[56]
The advantages of surgery are demonstrated efficacy for pain control,[78] it is more effective for infertility than medicinal intervention,[58] it provides a definitive diagnosis,[58] and surgery can often be performed as a minimally invasive (laparoscopic) procedure to reduce morbidity and minimize the risk of post-operative adhesions.[79] Efforts to develop effective strategies to reduce or prevent adhesions have been undertaken, but their formation remain a frequent side effect of abdominal surgery.[61]
The advantages of physical therapy techniques are decreased cost, absence of major side-effects, it does not interfere with fertility, and near-universal increase of sexual function.[77] Disadvantages are that there are no large or long-term studies of its use for treating pain or infertility related to endometriosis.[77]
Treatment of infertility
Surgery is more effective than medicinal intervention for addressing infertility associated with endometriosis.[58] Surgery attempts to remove endometrial tissue and preserve the ovaries without damaging normal tissue.[58] In-vitro fertilization (IVF) procedures are effective in improving fertility in many women with endometriosis.
Prognosis
Proper counseling of women with endometriosis requires attention to several aspects of the disorder. Of primary importance is the initial operative staging of the disease to obtain adequate information on which to base future decisions about therapy. The woman's symptoms and desire for childbearing dictate appropriate therapy. Not all therapy works for all women. Some women have recurrences after surgery or pseudo-menopause. In most cases, treatment will give women significant relief from pelvic pain and assist them in achieving pregnancy.[80]
The underlying process that causes endometriosis may not cease after surgical or medical intervention. Studies have shown that endometriosis recurs at a rate of 20 to 40 percent within five years following conservative surgery,[81] unless hysterectomy is performed or menopause reached. Monitoring of women consists of periodic clinical examinations and sonography.
Vaginal childbirth decreases recurrence of endometriosis. In contrast, endometriosis recurrence rates have been shown to be higher in women who have not given birth vaginally, such as in cesarean section.[82]
Complications
Complications of endometriosis include internal scarring, adhesions, pelvic cysts, chocolate cyst of ovaries, ruptured cysts, and bowel and ureteral obstruction resulting from pelvic adhesions.[83] Endometriosis-associated infertility can be related to scar formation and anatomical distortions due to the endometriosis.
Ovarian endometriosis may complicate pregnancy by decidualization, abscess and/or rupture.[84]
Pleural implantations are associated with recurrent right pneumothoraces at times of a menstrual period, termed catamenial pneumothorax.[85]
Epidemiology
Endometriosis can affect any female, from premenarche to postmenopause, regardless of race or ethnicity or whether or not they have had children. It is primarily a disease of the reproductive years.[86] The number of women affected is between 6–10%.[2] It is more common in women with infertility and chronic pelvic pain (35–50%).[2]
Incidences of endometriosis have occurred in postmenopausal women,[87] and in less common cases, girls may have endometriosis symptoms before they even reach menarche.[88][89]
History
Endometriosis was first discovered microscopically by Karl von Rokitansky in 1860,[90] although it was documented in medical texts more than 4,000 years ago.[91] The Hippocratic Corpus outlines symptoms similar to endometriosis, including uterine ulcers, adhesions, and infertility.[91] Historically, women with these symptoms were treated with leeches, straight-jackets, bloodletting, chemical douches, genital mutilation, pregnancy (as a form of treatment), hanging upside down, surgical intervention, and even killing due to suspicion of demonic possession.[91] Hippocratic doctors recognized and treated chronic pelvic pain as a true organic disorder 2,500 years ago, but during the Middle Ages, there was a shift into believing that women with pelvic pain were mad, immoral, imagining the pain, or simply misbehaving.[91] The symptoms of inexplicable chronic pelvic pain were often attributed to imagined madness, female weakness, promiscuity, or hysteria.[91] The historical diagnosis of hysteria, which was thought to be a psychological disease, may have indeed been endometriosis.[91] The idea that chronic pelvic pain was related to mental illness influenced modern attitudes regarding women with endometriosis, leading to delays in correct diagnosis and indifference to the patients' true pain during the 20th century.[91]
Hippocratic doctors believed that delaying childbearing could trigger diseases of the uterus, which caused endometriosis-like symptoms. Women with dysmenorrhea were encouraged to marry and have children at a young age.[91] The fact that Hippocratics were recommending changes in marriage practices due to an endometriosis-like illness implies that this disease was likely common, with rates higher than the 5-15% prevalence that is often cited today.[91] If indeed this disorder was so common historically, this may point away from modern theories that suggest links between endometriosis and dioxins, PCBs, and chemicals.[91]
Society and culture
As recently as 1995, reports found that over 50% of women with chronic pelvic pain had no organic cause, with women still often being considered mentally unstable.[92] Due to centuries-old attitudes linking mental illness to pelvic pain, there is often a delay in the correct diagnosis - on average, it takes six to seven years for a woman to receive the diagnosis of endometriosis.[93]
In terms of societal effects, the economic effects associated with endometriosis are substantial and are similar to that of other chronic diseases such as Crohn’s disease, diabetes, or rheumatoid arthritis.[94] This economic burden is attributed mostly to the inability to consistently work and predicted by decreased quality of life.[94]
References
- ↑ "Endometriosis: Overview". http://www.nichd.nih.gov''. 2013-06-24. Retrieved 4 March 2015.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 2.7 2.8 2.9 Bulletti C, Coccia ME, Battistoni S, Borini A (August 2010). "Endometriosis and infertility". J. Assist. Reprod. Genet. 27 (8): 441–7. doi:10.1007/s10815-010-9436-1. PMC 2941592. PMID 20574791.
- ↑ Culley L, Law C, Hudson N, Denny E, Mitchell H, Baumgarten M, Raine-Fenning N (2013). "The social and psychological impact of endometriosis on women's lives: A critical narrative review". Human Reproduction Update 19 (6): 625–639. doi:10.1093/humupd/dmt027. PMID 23884896.
- ↑ 4.0 4.1 4.2 4.3 4.4 4.5 "Endometriosis". http://www.womenshealth.gov/''. December 5, 2014. Retrieved 4 March 2015.
- ↑ 5.0 5.1 Vercellini P, Eskenazi B, Consonni D, Somigliana E, Parazzini F, Abbiati A, Fedele L (2011). "Oral contraceptives and risk of endometriosis: a systematic review and meta-analysis". Hum. Reprod. Update 17 (2): 159–70. doi:10.1093/humupd/dmq042. PMID 20833638.
- ↑ GBD 2013 Mortality and Causes of Death Collaborators (17 December 2014). "Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013.". Lancet 385: 117–71. doi:10.1016/S0140-6736(14)61682-2. PMID 25530442.
- ↑ Brosens I (2012). Endometriosis: Science and Practice. John Wiley & Sons. p. 3. ISBN 9781444398496.
- ↑ 8.0 8.1 Stratton P, Berkley KJ (2011). "Chronic pelvic pain and endometriosis: translational evidence of the relationship and implications". Hum. Reprod. Update 17 (3): 327–46. doi:10.1093/humupd/dmq050. PMC 3072022. PMID 21106492.
- ↑ Endometriosis;NIH Pub. No. 02-2413; September 2002
- ↑ 10.0 10.1 10.2 10.3 Ballard K, Lane H, Hudelist G, Banerjee S, Wright J (June 2010). "Can specific pain symptoms help in the diagnosis of endometriosis? A cohort study of women with chronic pelvic pain". Fertil. Steril. 94 (1): 20–7. doi:10.1016/j.fertnstert.2009.01.164. PMID 19342028.
- ↑ Murray MT, Pizzorno J (2012). The Encyclopedia of Natural Medicine (3rd ed.). New York, NY: Simon and Schuster.
- ↑ Endometriosis: Does It Cause Infertility?, from American Society for Reproductive Medicine. Revised 2012
- ↑ Arbique D, Carter S, van Sell S. (2008). Endometriosis can evade diagnosis: being alert to signs of endometriosis can arrest the disease before it takes over a patient's life. Rn, 71(9), 28-32. PMID 18833741
- ↑ Colette S, Donnez J (July 2011). "Are aromatase inhibitors effective in endometriosis treatment?". Expert Opin Investig Drugs 20 (7): 917–31. doi:10.1517/13543784.2011.581226. PMID 21529311.
- ↑ Pearce CL, Templeman C, Rossing MA et al. (2012). "Association between endometriosis and risk of histological subtypes of ovarian cancer: a pooled analysis of case-control studies". Lancet Oncol. 13 (4): 385–94. doi:10.1016/S1470-2045(11)70404-1. PMC 3664011. PMID 22361336.
- ↑ Nezhat F. Article by Prof. Farr Nezhat, MD, FACOG, FACS, University of Columbia, May 1, 2012
- ↑ Audebert A (April 2005). "La femme endométriosique est-elle différente ?" [Women with endometriosis: are they different from others?]. Gynécologie, Obstétrique & Fertilité (in French) 33 (4): 239–46. doi:10.1016/j.gyobfe.2005.03.010. PMID 15894210.
- ↑ Rowlands IJ, Nagle CM, Spurdle AB, Webb PM; Australian National Endometrial Cancer Study Group and Australian Ovarian Cancer Study Group (Dec 2011). "Gynecological conditions and the risk of endometrial cancer". Gynecol Oncol 3: 537–41.
- ↑ Benagiano G, Brosens I, Habiba M (2014). "Structural and molecular features of the endomyometrium in endometriosis and adenomyosis". Hum. Reprod. Update 20 (3): 386–402. doi:10.1093/humupd/dmt052. PMID 24140719.
- ↑ 20.0 20.1 20.2 20.3 20.4 20.5 20.6 20.7 20.8 20.9 Fauser BC, Diedrich K, Bouchard P, Domínguez F, Matzuk M, Franks S, Hamamah S, Simón C, Devroey P, Ezcurra D, Howles CM (2011). "Contemporary genetic technologies and female reproduction". Hum. Reprod. Update 17 (6): 829–47. doi:10.1093/humupd/dmr033. PMC 3191938. PMID 21896560.
- ↑ 21.0 21.1 Kapoor D, Davila W (2005). Endometriosis, eMedicine.
- ↑ Giudice LC, Kao LC (2004). "Endometriosis". Lancet 364 (9447): 1789–99. doi:10.1016/S0140-6736(04)17403-5. PMID 15541453.
- ↑ 23.0 23.1 23.2 23.3 23.4 23.5 23.6 Rahmioglu N, Nyholt DR, Morris AP et al. (2014). "Genetic variants underlying risk of endometriosis: insights from meta-analysis of eight genome-wide association and replication datasets". Human Reproduction Update 20 (5): 702–716. doi:10.1093/humupd/dmu015. ISSN 1355-4786.
- ↑ Painter JN, Anderson CA, Nyholt DR et al. (January 2011). "Genome-wide association study identifies a locus at 7p15.2 associated with endometriosis". Nature Genetics 43 (1): 51–4. doi:10.1038/ng.731. PMC 3019124. PMID 21151130.
- ↑ Treloar SA, Wicks J, Nyholt DR et al. (September 2005). "Genomewide linkage study in 1,176 affected sister pair families identifies a significant susceptibility locus for endometriosis on chromosome 10q26". American Journal of Human Genetics 77 (3): 365–76. doi:10.1086/432960. PMC 1226203. PMID 16080113.
- ↑ Anger DL, Foster WG (2008). "The link between environmental toxicant exposure and endometriosis". Frontiers in Bioscience 13: 1578–93. doi:10.2741/2782. PMID 17981650.
- ↑ Guo SW (2004). "The link between exposure to dioxin and endometriosis: a critical reappraisal of primate data". Gynecologic and Obstetric Investigation 57 (3): 157–73. doi:10.1159/000076374. PMID 14739528.
- ↑ Guo SW, Simsa P, Kyama CM et al. (October 2009). "Reassessing the evidence for the link between dioxin and endometriosis: from molecular biology to clinical epidemiology". Molecular Human Reproduction 15 (10): 609–24. doi:10.1093/molehr/gap075. PMID 19744969.
- ↑ Rier S, Foster WG (December 2002). "Environmental dioxins and endometriosis". Toxicological Sciences 70 (2): 161–70. doi:10.1093/toxsci/70.2.161. PMID 12441361.
- ↑ Burney RO, Giudice LC (September 2012). "Pathogenesis and pathophysiology of endometriosis". Fertil. Steril. 98 (3): 511–9. doi:10.1016/j.fertnstert.2012.06.029. PMC 3836682. PMID 22819144.
- ↑ van der Linden PJ (1996). "Theories on the pathogenesis of endometriosis". Human reproduction (Oxford, England). 11 Suppl 3: 53–65. doi:10.1093/humrep/11.suppl_3.53. PMID 9147102.
- ↑ Gleicher N, el-Roeiy A, Confino E, Friberg J (July 1987). "Is endometriosis an autoimmune disease?". Obstet Gynecol 70 (1): 115–22. PMID 3110710.
- ↑ Capellino S, Montagna P, Villaggio B, Sulli A, Soldano S et al. (June 2006). "Role of estrogens in inflammatory response: expression of estrogen receptors in peritoneal fluid macrophages from endometriosis". Annals of the New York Academy of Sciences 1069: 263–7. doi:10.1196/annals.1351.024. PMID 16855153.
- ↑ 34.0 34.1 Young VJ, Brown JK, Saunders PT, Horne AW (2013). "The role of the peritoneum in the pathogenesis of endometriosis". Human Reproduction Update 19 (5): 558–569. doi:10.1093/humupd/dmt024. PMID 23720497.
- ↑ Redwine DB (October 2002). "Was Sampson wrong?". Fertility and Sterility 78 (4): 686–93. doi:10.1016/S0015-0282(02)03329-0. PMID 12372441.
- ↑ Signorile PG, Baldi F, Bussani R, D'Armiento M, De Falco M, Baldi A (April 2009). "Ectopic endometrium in human foetuses is a common event and sustains the theory of müllerianosis in the pathogenesis of endometriosis, a disease that predisposes to cancer". Journal of Experimental & Clinical Cancer Research 28: 49. doi:10.1186/1756-9966-28-49. PMC 2671494. PMID 19358700.
- ↑ 37.0 37.1 "Diagnosis and Treatment of Endometriosis". American Academy of Family Physicians. 1999-10-15. Retrieved 2011-07-26.
- ↑ Laschke MW, Giebels C, Menger MD (2011). "Vasculogenesis: a new piece of the endometriosis puzzle". Hum. Reprod. Update 17 (5): 628–36. doi:10.1093/humupd/dmr023. PMID 21586449.
- ↑ Morotti M, Vincent K, Brawn J, Zondervan KT, Becker CM (2014). "Peripheral changes in endometriosis-associated pain". Human Reproduction Update 20 (5): 717–736. doi:10.1093/humupd/dmu021. ISSN 1355-4786.
- ↑ Jenkins S, Olive DL, Haney AF (March 1986). "Endometriosis: pathogenetic implications of the anatomic distribution". Obstetrics and gynecology 67 (3): 335–8. PMID 3945444.
- ↑ Weed JC, Ray JE (May 1987). "Endometriosis of the bowel". Obstetrics and gynecology 69 (5): 727–30. PMID 3574800.
- ↑ Uzunçakmak C, Güldaş A, Ozçam H, Dinç K (2013). "Scar endometriosis: a case report of this uncommon entity and review of the literature". Case reports in obstetrics and gynecology 2013: 386783. doi:10.1155/2013/386783. PMID 23762683.
- ↑ Dwivedi AJ, Agrawal SN, Silva YJ (February 2002). "Abdominal wall endometriomas". Digestive diseases and sciences 47 (2): 456–61. PMID 11855568.
- ↑ Kaunitz A, Di Sant'Agnese PA (December 1979). "Needle tract endometriosis: an unusual complication of amniocentesis". Obstetrics and gynecology 54 (6): 753–5. PMID 160025.
- ↑ Koger KE, Shatney CH, Hodge K, McClenathan JH (September 1993). "Surgical scar endometrioma.". Surgery, gynecology & obstetrics 177 (3): 243–6. PMID 8356497.
- ↑ Daly S (October 18, 2004). "Endometrioma/Endometriosis". WebMD. Retrieved 2006-12-19.
- ↑ Office on Women’s Health, U.S. Department of Health and Human Services. (16 July 2012). Endometriosis Fact Sheet. Retrieved from Womenshealth.gov http://www.womenshealth.gov/publications/our-publications/fact-sheet/endometriosis.html
- ↑ Nisolle M, Paindaveine B, Bourdon A, Berlière M, Casanas-Roux F, Donnez J (June 1990). "Histologic study of peritoneal endometriosis in infertile women". Fertility and Sterility 53 (6): 984–8. PMID 2351237.
- ↑ 49.0 49.1 Practice Committee of the American Society for Reproductive, Medicine (April 2014). "Treatment of pelvic pain associated with endometriosis: a committee opinion.". Fertility and Sterility 101 (4): 927–35. doi:10.1016/j.fertnstert.2014.02.012. PMID 24630080.
- ↑ American Society For Reproductive M, (May 1997). "Revised American Society for Reproductive Medicine classification of endometriosis: 1996". Fertility and Sterility 67 (5): 817–21. doi:10.1016/S0015-0282(97)81391-X. PMID 9130884.
- ↑ 51.0 51.1 51.2 51.3 51.4 51.5 May KE, Conduit-Hulbert SA, Villar J, Kirtley S, Kennedy SH, Becker CM (2010). "Peripheral biomarkers of endometriosis: a systematic review". Hum. Reprod. Update 16 (6): 651–74. doi:10.1093/humupd/dmq009. PMC 2953938. PMID 20462942.
- ↑ May KE, Villar J, Kirtley S, Kennedy SH, Becker CM (2011). "Endometrial alterations in endometriosis: a systematic review of putative biomarkers". Hum. Reprod. Update 17 (5): 637–53. doi:10.1093/humupd/dmr013. PMID 21672902.
- ↑ http://www.rfay.com.au/docs/cd10poster.pdf
- ↑ Bourdel N, Alves J, Pickering G et al. (2014). "Systematic review of endometriosis pain assessment: how to choose a scale?". Human Reproduction Update 21 (1): 136–152. doi:10.1093/humupd/dmu046. ISSN 1355-4786.
- ↑ Ling FW (January 1999). "Randomized controlled trial of depot leuprolide in patients with chronic pelvic pain and clinically suspected endometriosis. Pelvic Pain Study Group.". Obstetrics and gynecology 93 (1): 51–8. doi:10.1016/s0029-7844(98)00341-x. PMID 9916956.
- ↑ 56.0 56.1 "What are the treatments for endometriosis". Eunice Kennedy Shriver National Institute of Child Health and Human Development. Retrieved 20 August 2013.
- ↑ Moen MH, Rees M, Brincat M et al. (2010). "EMAS position statement: Managing the menopause in women with a past history of endometriosis". Maturitas 67 (1): 94–7. doi:10.1016/j.maturitas.2010.04.018. PMID 20627430.
- ↑ 58.0 58.1 58.2 58.3 58.4 58.5 58.6 Wellbery C (1999). "Diagnosis and treatment of endometriosis". Am Fam Physician 60 (6): 1753–62, 1767–8. PMID 10537390.
- ↑ Speroff L, Glass RH, Kase NG (1999). Clinical Gynecologic Endocrinology and Infertility (6th ed.). Lippincott Willimas Wilkins. p. 1057. ISBN 0-683-30379-1.
- ↑ "Endometriosis and Infertility: Can Surgery Help?" (PDF). American Society for Reproductive Medicine. 2008. Retrieved 31 Oct 2010.
- ↑ 61.0 61.1 Liakakos T, Thomakos N, Fine PM, Dervenis C, Young RL (2001). "Peritoneal Adhesions: Etiology, Pathophysiology, and Clinical Significance". Dig Surgery 18 (4): 260–273. doi:10.1159/000050149. PMID 11528133.
- ↑ Trehan AK (2002). "Temporary ovarian suspension". Gynaecological Endoscopy 11 (1): 309–314. doi:10.1046/j.1365-2508.2002.00520.x. PMID 11821616.
- ↑ name="pmid11821616">Abuzeid MI, Ashraf M, Shamma FN (2002). "Temporary ovarian suspension at laparoscopy for prevention of adhesions". J Am Assoc Gynecol Laparosc 9 (1): 98–102. doi:10.1046/j.1365-2508.2002.00520.x. PMID 11821616.
- ↑ Namnoum AB, Hickman TN, Goodman SB, Gehlbach DL, Rock JA (November 1995). "Incidence of symptom recurrence after hysterectomy for endometriosis". Fertility and Sterility 64 (5): 898–902. PMID 7589631.
- ↑ Guo SW (2009). "Recurrence of endometriosis and its control". Hum. Reprod. Update 15 (4): 441–61. doi:10.1093/humupd/dmp007. PMID 19279046.
- ↑ 66.0 66.1 Johnson NP, Hummelshoj L (June 2013). "Consensus on current management of endometriosis.". Human Reproduction 28 (6): 1552–68. doi:10.1093/humrep/det050. PMID 23528916.
- ↑ Patel B, Elguero S, Thakore S et al. (2014). "Role of nuclear progesterone receptor isoforms in uterine pathophysiology". Human Reproduction Update 21 (2): 155–173. doi:10.1093/humupd/dmu056. ISSN 1355-4786.
- ↑ Harada T, Momoeda M, Taketani Y, Hoshiai H, Terakawa N (November 2008). "Low-dose oral contraceptive pill for dysmenorrhea associated with endometriosis: a placebo-controlled, double-blind, randomized trial". Fertility and Sterility 90 (5): 1583–8. doi:10.1016/j.fertnstert.2007.08.051. PMID 18164001.
- ↑ Attar E, Bulun SE (May 2006). "Aromatase inhibitors: the next generation of therapeutics for endometriosis?". Fertility and Sterility 85 (5): 1307–18. doi:10.1016/j.fertnstert.2005.09.064. PMID 16647373.
- ↑ Flower A, Liu JP, Chen S, Lewith G, Little P (2009). Flower, Andrew, ed. "Chinese herbal medicine for endometriosis". Cochrane Database Syst Rev (3): CD006568. doi:10.1002/14651858.CD006568.pub2. PMID 19588398.
- ↑ Lu D, Song H, Li Y, Clarke J, Shi G (Jan 18, 2012). "Pentoxifylline for endometriosis.". Cochrane database of systematic reviews (Online) 1: CD007677. doi:10.1002/14651858.CD007677.pub3. PMID 22258970.
- ↑ "Practice bulletin no. 114 management of endometriosis". Obstet Gynecol 116 (1): 223–36. July 2010. doi:10.1097/AOG.0b013e3181e8b073. PMID 20567196.
- ↑ 73.0 73.1 Laschke MW, Menger MD (2012). "Anti-angiogenic treatment strategies for the therapy of endometriosis". Human Reproduction Update 18 (6): 682–702. doi:10.1093/humupd/dms026. PMID 22718320.
- ↑ Canny GO, Lessey BA (2013). "The role of lipoxin A4 in endometrial biology and endometriosis". Mucosal Immunol 6 (3): 439–50. doi:10.1038/mi.2013.9. PMC 4062302. PMID 23485944.
- ↑ Streuli I, de Ziegler D, Santulli P et al. (2013). "An update on the pharmacological management of endometriosis". Expert Opin Pharmacother 14 (3): 291–305. doi:10.1517/14656566.2013.767334. PMID 23356536.
- ↑ Valiani M, Ghasemi N, Bahadoran P, Heshmat R (2010). "The effects of massage therapy on dysmenorrhea caused by endometriosis". Iran J Nurs Midwifery Res 15 (4): 167–71. PMC 3093183. PMID 21589790.
- ↑ 77.0 77.1 77.2 Wurn BF, Wurn LJ, Patterson K, King CR, Scharf ES (2011). "Decreasing dyspareunia and dysmenorrhea in women with endometriosis via a manual physical therapy: Results from two independent studies". Journal of Endometriosis and Pelvic Pain Disorders 3: 188–196. doi:10.5301/JE.2012.9088.
- ↑ Kaiser A, Kopf A, Gericke C, Bartley J, Mechsner S (16 January 2009). "The influence of peritoneal endometriotic lesions on the generation of endometriosis-related pain and pain reduction after surgical excision". Arch Gynecol Obstet. 280 (3): 369–73. doi:10.1007/s00404-008-0921-z. PMID 19148660.
- ↑ Radosa MP, Bernardi TS, Georgiev I, Diebolder H, Camara O, Runnebaum IB (June 2010). "Coagulation versus excision of primary superficial endometriosis: a 2-year follow-up". Eur. J. Obstet. Gynecol. Reprod. Biol. 150 (2): 195–8. doi:10.1016/j.ejogrb.2010.02.022. PMID 20303642.
- ↑ Memarzadeh S, Muse KN, Fox, MD (September 21, 2006). "Endometriosis". Differential Diagnosis and Treatment of endometriosis. Armenian Health Network, Health.am. Retrieved 2006-12-19.
- ↑ "Recurrent Endometriosis: Surgical Management". Endometriosis. The Cleveland Clinic. 7 Jan 2010. Retrieved 31 Oct 2010.
- ↑ Bulletti C, Montini A, Setti PL et al. (June 2009). "Vaginal parturition decreases recurrence of endometriosis". Fertil. Steril. 94 (3): 850–5. doi:10.1016/j.fertnstert.2009.04.012. PMID 19524893.
- ↑ Acosta S, Leandersson U, Svensson SE, Johnsen J (May 2001). "Fallbeskrivning. Endometrios orsakade kolonileus, uretärobstruktion och hypertoni" [A case report. Endometriosis caused colonic ileus, ureteral obstruction and hypertension]. Läkartidningen (in Swedish) 98 (18): 2208–12. PMID 11402601.
- ↑ Ueda Y, Enomoto T, Miyatake T et al. (June 2010). "A retrospective analysis of ovarian endometriosis during pregnancy". Fertility and Sterility 94 (1): 78–84. doi:10.1016/j.fertnstert.2009.02.092. PMID 19356751.
- ↑ Visouli AN, Zarogoulidis K, Kougioumtzi I et al. (October 2014). "Catamenial pneumothorax.". Journal of thoracic disease 6 (Suppl 4): S448–60. doi:10.3978/j.issn.2072-1439.2014.08.49. PMID 25337402.
- ↑ Nothnick WB (2011). "The emerging use of aromatase inhibitors for endometriosis treatment". Reprod. Biol. Endocrinol. 9: 87. doi:10.1186/1477-7827-9-87. PMC 3135533. PMID 21693036.
- ↑ Bulun SE, Zeitoun K, Sasano H, Simpson ER (1999). "Aromatase in aging women". Seminars in Reproductive Endocrinology 17 (4): 349–58. doi:10.1055/s-2007-1016244. PMID 10851574.
- ↑ Batt RE, Mitwally MF (December 2003). "Endometriosis from thelarche to midteens: pathogenesis and prognosis, prevention and pedagogy". Journal of Pediatric and Adolescent Gynecology 16 (6): 337–47. doi:10.1016/j.jpag.2003.09.008. PMID 14642954.
- ↑ Marsh EE, Laufer MR (March 2005). "Endometriosis in premenarcheal girls who do not have an associated obstructive anomaly". Fertility and Sterility 83 (3): 758–60. doi:10.1016/j.fertnstert.2004.08.025. PMID 15749511.
- ↑ Batt, Ronald E. (2011). A history of endometriosis. London: Springer. pp. 13–38. ISBN 978-0-85729-585-9.
- ↑ 91.0 91.1 91.2 91.3 91.4 91.5 91.6 91.7 91.8 91.9 Nezhat C, Nezhat F, Nezhat C (December 2012). "Endometriosis: ancient disease, ancient treatments.". Fertility and Sterility 98 (6 Suppl): S1–62. doi:10.1016/j.fertnstert.2012.08.001. PMID 23084567.
- ↑ Gomel V, Taylor PJ (1995). Diagnostic and operative gynecologic laparoscopy. St. Louis, MO: Mosby.
- ↑ Overton C, Davis C, McMillan L, Shaw RW (2007). An atlas of endometriosis (3rd ed.). London: Informa Healthcare.
- ↑ 94.0 94.1 Simoens S, Dunselman G, Dirksen C et al. (14 March 2012). "The burden of endometriosis: costs and quality of life of women with endometriosis and treated in referral centres". Human Reproduction 27 (5): 1292–1299. doi:10.1093/humrep/des073.
External links
| Wikimedia Commons has media related to Endometriosis. |
- Endometriosis at DMOZ
- Endometriosis fact sheet from womenshealth.gov
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||