Endodontic therapy
Endodontic therapy or root canal therapy is a sequence of treatment for the infected pulp of a tooth which results in the elimination of infection and the protection of the decontaminated tooth from future microbial invasion.[1] Root canals and their associated pulp chamber are the physical hollows within a tooth that are naturally inhabited by nerve tissue, blood vessels and other cellular entities which together constitute the dental pulp.[2] Endodontic therapy involves the removal of these structures, the subsequent shaping, cleaning, and decontamination of the hollows with small files and irrigating solutions, and the obturation (filling) of the decontaminated canals with an inert filling such as gutta-percha and typically a eugenol-based cement.[3] Epoxy resin is employed to bind gutta-percha in some root canal procedures.[4]
Treatment procedure


.jpg)
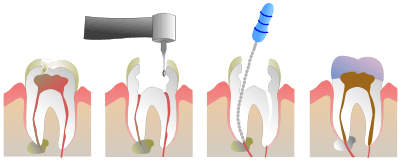
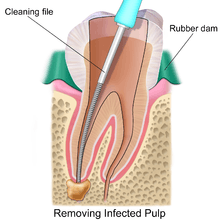
In the situation that a tooth is considered so threatened (because of decay, cracking, etc.) that future infection is considered likely or inevitable, a pulpectomy, removal of the pulp tissue, is advisable to prevent such infection. Usually, some inflammation and/or infection is already present within or below the tooth. To cure the infection and save the tooth, the dentist drills into the pulp chamber and removes the infected pulp and then drills the nerve out of the root canal(s) with long needle-shaped hand instruments known as files (H files and K files). Starting with a smaller file size (sometimes termed a 'pathfinder'), progressively larger files are used to widen the canals. This process serves to remove debris and infected tissue and facilitates greater penetration of an irrigating solution (see 'irrigants' below). After this is done, the dentist fills each of the root canals and the chamber with an inert material and seals up the opening. This procedure is known as root canal therapy. With the removal of nerves and blood supply from the tooth, it is best that the tooth be fitted with a crown.
The standard filling material is gutta-percha, a natural polymer prepared from latex from the percha (Palaquium gutta) tree. The standard endodontic technique involves inserting a gutta-percha cone (a "point") into the cleaned-out root canal along with a sealing cement.[5] Another technique uses melted or heat-softened gutta-percha which is then injected or pressed into the root canal passage(s). However, as gutta-percha shrinks as it cools, thermal techniques can be unreliable and sometimes a combination of techniques is used. Gutta-percha is radiopaque, allowing verification afterwards that the root canal passages have been completely filled, without voids.
An alternative filling material was invented in the early 1950s by Angelo Sargenti. It has undergone several formulations over the years (N2, N2 Universal, RC-2B, RC-2B White), but all contain paraformaldehyde. The paraformaldehyde, when placed into the root canal, forms formaldehyde, which penetrates and sterilizes the passage. The formaldehyde is then theoretically transformed to harmless water and carbon dioxide. The outcome is better than a root canal done with gutta-percha according to some investigations. There is however a lack of indisputable, scientifically made studies according to the Swedish Council on Health Technology Assessment.
In rare cases, the paste like any other material can be forced past the root tip into the surrounding bone. If this happens, the formaldehyde will immediately be transformed into a harmless substance. The blood normally contains 2 mg formaldehyde per liter and the body regulates this in seconds. The rest of an overfill will be gradually absorbed and the end result is normally good. In 1991 the ADA Council on Dental Therapeutics resolved that the treatment was "not recommended", and it is not taught in any American dental school. Scientific evidence in endodontic therapy was, and still is lacking.[6] The Sargenti technique has its advocates, however, who believe N2 to be less expensive and at least as safe as gutta-percha.[7]
For some patients, root canal therapy is one of the most feared dental procedures, perhaps because of a painful abscess that necessitated the root canal procedure. However, dental professionals assert that modern root canal treatment is relatively painless because the pain can be controlled with a local anesthetic during the procedure and pain control medication can be used before and/or after treatment assuming that the dentist takes the time to administer one. However, in some cases it may be very difficult to achieve pain control before performing a root canal. For example, if a patient has an abscessed tooth, with a swollen area or "fluid-filled gum blister" next to the tooth, the pus in the abscess may contain acids that inactivate any anesthetic injected around the tooth. In this case, the dentist may drain the abscess by cutting it to let the pus drain out. Releasing the pus releases pressure built up around the tooth; this pressure causes the pain. The dentist then prescribes a week of antibiotics such as penicillin, which will reduce the infection and pus, making it easier to anesthetize the tooth when the patient returns one week later. The dentist could also open up the tooth and let the pus drain through the tooth, and could leave the tooth open for a few days to help relieve pressure.
A root treated tooth may be eased from the occlusion as a measure to prevent tooth fracture prior to the cementation of a crown or similar restoration. Sometimes the dentist performs preliminary treatment of the tooth by removing all of the infected pulp of the tooth and applying a dressing and temporary filling to the tooth. This is called a pulpectomy. The dentist may also remove just the coronal portion of the dental pulp, which contains 90% of the nerve tissue, and leave intact the pulp in the canals. This procedure, called a "pulpotomy", tends to essentially eliminate all the pain. A pulpotomy may be a relatively definitive treatment for infected primary teeth. The pulpectomy and pulpotomy procedures aim to eliminate pain until the follow-up visit for finishing the root canal. Further occurrences of pain could indicate the presence of continuing infection or retention of vital nerve tissue.
After removing as much of the internal pulp as possible, the root canal(s) can be temporarily filled with calcium hydroxide paste. This strong base is left in for a week or more to disinfect and reduce inflammation in surrounding tissue. The patient may still complain of pain if the dentist left pulp devitalizer over canal thus one visit increased.[8] Ibuprofen taken orally is commonly used before and/or after these procedures to reduce inflammation.
The following substances may be used as root canal irrigants during the root canal procedure:
- less than 5% sodium hypochlorite (NaOCl)
- 6% sodium hypochlorite with surface modifiers for better flow into nooks and crannies
- 2% chlorhexidine gluconate
- 0.2% chlorhexidine gluconate plus 0.2% cetrimide
- 17% ethylenediaminetetraacetic acid (EDTA)
- Framycetin sulfate
- Mixture of citric acid, doxycycline, and polysorbate 80 (detergent) (MTAD)
Molars and premolars that have had root canal therapy should be protected with a crown that covers the cusps of the tooth. This is because the access made into the root canal system removes a significant amount of tooth structure. Molars and premolars are the primary teeth used in function, and will almost certainly fracture in the future without cuspal coverage. Anterior teeth typically do not require full coverage restorations after a root canal, unless there is extensive tooth loss from decay or for esthetics or unusual occlusion. Placement of a crown or cusp-protecting cast gold covering is recommended also because these have the best ability to seal the root canaled tooth. If the tooth is not perfectly sealed, the root canal may leak, causing eventual failure of the root canal. Also, many people believe once a tooth has had a root canal treatment it cannot get decay. This is not true. A tooth with a root canal treatment still has the ability to decay, and without proper home care and an adequate fluoride source the tooth structure can become severely decayed (often without the patient's knowledge since the nerve has been removed, leaving the tooth without any pain perception). Thus, non-restorable carious destruction is the main reason for extraction of teeth after root canal therapy, with up to two-thirds of these extractions.[9] Therefore it is very important to have regular X-rays taken of the root canal to ensure that the tooth is not having any problems that the patient would not be aware of.

The procedure is often complicated, depending on circumstances, and may involve multiple visits over a period of weeks. The cost is typically high.
History
Nunn et al.[10] trace the history back to 1756, at which date Philip Pfaff[11] published his work on gold as a filler material.
Alternatives
The alternatives to root canal therapy include no treatment, tooth extraction, or 3Mix-MP procedure. Following tooth extraction, options for prostethic replacement may include a dental implant(s), a fixed partial denture (commonly referred to as a 'bridge'), or by a removable denture.[12] There are risks to conducting no treatment such as pain, infection and the possibility of worsening dental infection such that the tooth will be no longer restorable (root canal treatment will not be successful, often due to excessive loss of tooth structure). If extensive loss of tooth structure occurs, extraction may be the only treatment option.
In December 2010, a study was published demonstrating a new alternative to root canal therapy in treating infected tooth pulps, 3Mix-MP procedure, through the local application of an antibacterial drug mixture.[13] While previous studies had failed in similar experiments, this study succeeded by utilizing a unique vehicle for the antibiotics, propylene glycol, which has been shown to successfully penetrate and spread through dentinal tubules.[14] This is an important finding which seems to offer an alternative to root canal therapy other than tooth extraction.
Innovation
In the last ten to twenty years, there have been great innovations in the art and science of root canal therapy. Dentists now must be educated on the current concepts in order to optimally perform a root canal. Root canal therapy has become more automated and can be performed faster thanks, in part, to machine driven rotary technology and more advanced root canal filling methods. Many root canal procedures are done in one dental visit which may last for around 1–2 hours. Newer technologies are available (e.g. cone-beam CT scanning) that allow more efficient, scientific measurements to be taken of the dimensions of the root canal. Many dentists use dental loupes to perform root canal therapy, and the consensus is that root canals performed using loupes, or other forms of magnification (e.g. a surgical microscope), are more likely to succeed than those performed without them. Although general dentists are becoming versed in these advanced technologies, they are still more likely to be used by specialist root canal doctors (known as endodontists).
Laser root canal procedures are a controversial innovation. Lasers may be fast but have not been shown to thoroughly disinfect the whole tooth,[15] and may cause damage.[16]
Types of canal instrumentation
Dr. Gargs' Textbook of Endodontics, II ed., describes several procedures and techniques of canal shaping.
Procedures for shaping
The oldest cited is the standardized one, introduced by Ingle. It has disadvantages like chances of loss of working length and easily making ledging, zipping or perforations.
The step back technique, also known as telescopic or serial root canal preparation, was first described by Mullaney and is divided in two phases: during the first one the working length is established and then the apical part of the canal is delicately shaped since «a size 25 K-file reaches the working length; during the second one the remaining canal part is prepared with manual or rotating instrumentation.
This procedure, however, has some disadvantages, like iatrogenic errors like apical transportation, i.e. too short or long instrumentation, that are worked out by the modified step back, or piling obstructing debris up, that are worked out by the passive step back developed by Torabinejad.
All these procedures and the following ones provide frequent irrigation and recapitulation with master apical file, i.e. the small file (usually a 10 or 15) that reaches the apical foramen.
The crown down is a procedure in which the dentist prepares the canal beginning from the coronal part after exploring the patency of the whole canal with the master apical file.
There is also a "hybrid" procedure combining "step back" and "crown down": after the canal's patency check, the coronal third is prepared with hand or Gates Glidden drills, then the working length is determined and finally the apical portion is shaped «using step back techniques.
The double flare is a procedure introduced by Fava where the canal is explored using a small file. Then canal is prepared in crown down manner using K-files then follows a "step back" preparation with 1 mm increments with increasing file sizes.
Another book, Endodontics by prof. Castellucci from Florence, describes the Early coronal enlargement, ideated by prof. Clifford J. Ruddle from Santa Barbara; this technique is the same as that by dr. Francesco Riitano from Catanzaro previously described as "three times technique". However, according to this complex procedure, apical canals are in the first place prepared initially after a working length check with an apex locator; then progressively enlarged with Gates Glidden drills (only coronal and middle third); in a third time the dentist "arrives at the apex" and, if necessary, prepares the apical foramen with a size 25 K-file; the last phase is divided in two refining passages: the first one with 1-mm-staggered instrument, the second one with 0.5 staggering.
From the early nineties engine-driven instrumentation were gradually introduced; these are: the ProFile system, the Greater Taper files (or "GT files"), the ProTaper files (highly praised by Castellucci), and other systems like Light Speed, Quantec, K-3 rotary, Real World Endo, and Hero 642.
Ultrasound preparations are also described by Gargs, but the writer has no direct or indirect experience of that, so he will not outline this topic.
Operative techniques for instruments
Gargs and Castellucci also display various hand technique about how to maneuver endodontic instruments;
There are two slightly different anti-curvature technique: one according the Textbook of Endodontics and one according the Endodontics. The first one was developed by Lin, the other by Abou-Rass, Franck and Glick.
In the balanced forces technique, developed in 1985 by Roane and Sabala, the dentist inserts his file into the canal and rotates clockwise a quarter of a turn, engaging dentin, then rotates counter-clockwise half/three quarter of a revolution, applying pressure in apical direction, shearing off tissue previously meshed.
From the "balanced forces" stem two other techniques: the reverse balanced force (where GT instruments are rotated first anti-clockwise and then clockwise) and the gentler "feed it in and pull" where the instrument is rotated only a quarter of a revolution and moved coronally after engagement, but not drawn out.
Procedural accidents
Instruments may separate (break) during root canal treatment, meaning a portion of the metal file used during the procedure remains inside the tooth. The file segment may be left behind if an acceptable level of cleaning and shaping has already been completed and attempting to remove the segment would risk damage to the tooth. While potentially disconcerting to the patient, having metal inside of a tooth is relatively common, such as with metal posts, amalgam fillings, gold crowns, and porcelain fused to metal crowns. The occurrence of file separation is proportional to the narrowness, curvature, length, calcification and number of roots on the tooth being treated. Complications resulting from incompletely cleaned canals, due to blockage from the separated file, can be addressed with surgical root canal treatment. The occurrence of instrument separation is well documented.[17]
A sodium hypochlorite incident is an immediate reaction of severe pain, followed by edema, haematoma and ecchymosis as a consequence of the solution escaping the confines of the tooth and entering the periapical space.[18] This may be caused iatrogenically by binding or excessive pressure on the irrigant syringe or it may occur if the tooth has an unusually large apical foramen.[19] It is usually self resolving and may take 2 to 5 weeks to fully resolve.[19]
Success and prognosis
Root canal treated teeth may fail to heal, for example if the dentist does not find, clean and fill all of the root canals within a tooth. On a maxillary molar, there is a more than 50% chance that the tooth has four canals instead of just three. But the fourth canal, often called a "mesio-buccal 2", tends to be very difficult to see and often requires special instruments and magnification in order to see it (most commonly found in first maxillary molars; studies have shown an average of 76% up to 96% of such teeth with the presence of an MB2 canal). This infected canal may cause a continued infection or "flare up" of the tooth. Any tooth may have more canals than expected, and these canals may be missed when the root canal is performed. Sometimes canals may be unusually shaped, making them impossible to clean and fill completely; some infected material may remain in the canal. Sometimes the canal filling does not fully extend to the apex of the tooth, or it does not fill the canal as densely as it should. Sometimes a tooth root may be perforated while the root canal is being treated, making it difficult to fill the tooth. The perforation may be filled with a root repair material, such as one derived from natural cement called mineral trioxide aggregate (MTA). A specialist can often re-treat failing root canals, and these teeth will then heal, often years after the initial root canal procedure.
However, the survival or functionality of the endodontically-treated tooth is often the most important aspect of endodontic treatment outcomes, rather than apical healing alone.[20] Recent studies indicate that substances commonly used to clean the root canal space incompletely sterilize the canal.[21] A properly restored tooth following root canal therapy yields long-term success rates near 97%. In a large scale Delta Dental Study of over 1.6 million patients who had root canal therapy, 97% had retained their teeth 8 years following the procedure, with most untoward events, such as re-treatment, apical surgery or extraction, occurring during the first 3 years after the initial endodontic treatment.[22] Endodontically treated teeth are prone to extraction mainly due to non-restorable carious destruction and to a lesser extent to endodontic-related reasons such as endodontic failure, vertical root fracture, or perforation (procedural error).[9]
Systemic issues
An infected tooth may endanger other parts of the body. People with special vulnerabilities, such as prosthetic joint replacement or mitral valve prolapse, may need to take antibiotics to protect from infection spreading during dental procedures. Both endodontic therapy and tooth extraction can lead to subsequent jaw bone infection. The American Dental Association (ADA) asserts that any risks can be adequately controlled.
In the early 1900s, several researchers theorized that bacteria from teeth which had necrotic pulps or which had received endodontic treatment could cause chronic or local infection in areas distant from the tooth through the transfer of bacteria through the bloodstream. This was called the "focal infection theory", and it led some dentists to advocate dental extraction. In the 1930s, this theory was discredited, but the theory was recently revived by a book entitled Root Canal Cover-Up Exposed which used the early discredited research, and further complicated by epidemiological studies which found correlations between periodontal disease and heart disease, strokes, and preterm births. Bacteremia (bacteria in the bloodstream) can be caused by many everyday activities, e.g. brushing teeth, but may also be caused after any dental procedure which involves bleeding. It is particularly likely after dental extractions due to the movement of the tooth and force needed to dislodge it, but endodontically treated teeth alone do not cause bacteremia or systemic disease.[23]
See also
- Endodontic retreatment
- Dental implant
- Dental pulp
- Dentistry
- Gum inflammation
- Oral and maxillofacial surgery
- Periodontitis
- Regenerative endodontics
- Toothache
- Tooth extraction
- American Association of Endodontists
- Smear layer
References
- ↑ Cohen, Stephen (2006). Pathways of the Pulp. Mosby. ISBN 032303067X.
- ↑ Nanci, Antonio (2012). Ten Cate's Oral Histology: Development, Structure, and Function. Mosby. ISBN 032307846X.
- ↑ Patel, Shanon (2013). The Principles of Endodontics. OUP Oxford. ISBN 0199657513.
- ↑ M. A. Marciano, R. Ordinola-Zapata, T. V. R. N. Cunha, M. A. H. Duarte, B. C. Cavenago, R. B. Garcia, C. M. Bramante, N. Bernardineli, I. G. Moraes (April 2011). "Analysis of four gutta-percha techniques used to fill mesial root canals of mandibular molars". International Endodontic Journal 44: 321–329. doi:10.1111/j.1365-2591.2010.01832.x. PMID 21219361.
- ↑ Tronstad, Leif (2008). Clinical Endodontics: A Textbook. Thieme. ISBN 978-3-13-768103-8.
- ↑ Barrett, M.D., Stephen (Jan 9, 2011), Be Wary of Sargenti Root Canal Treatment
- ↑ The Truth about Sargenti N2 Steup, 2001 [201] Treatment outcome. N2. The collected data indicates that the N2DONTIC Method according to Sargenti is classified as successful method for the evaluated practice.
- ↑ Hargreaves, Ken M (2006), "Single-visit more effective than multiple-visit root canal treatment?", Evidence-Based Dentistry 7 (1): 13–14, doi:10.1038/sj.ebd.6400372, PMID 16557250
- ↑ 9.0 9.1 Zadik Y, Sandler V, Bechor R, Salehrabi R (August 2008), "Analysis of factors related to extraction of endodontically treated teeth", Oral Surg Oral Med Oral Pathol Oral Radiol Endod 106 (5): e31, doi:10.1016/j.tripleo.2008.06.017, PMID 18718782.
- ↑ Nunn JH, Smeaton I, Gilroy J. (1996). "The development of formocresol as a medicament for primary molar pulpotomy procedures.". ASDC J Dent Child. 63 (1): 51–53. PMID 8655751.
- ↑ German wiki of Philip Pfaff
- ↑ Shillingberg, Herbert (1997). Fundamentals of Fixed Prosthodontics. Quintessence Publishing Co Inc. ISBN 086715201X.
- ↑ "Survival of Root Canal Pulp Tissue after Pulpitis".
- ↑ Cruz, E. V.; Kota, K.; Huque, J.; Iwaku, M.; Hoshino, E. "Penetration of propylene glycol into dentine". Journal of Endodontics Research.
- ↑ D. Jha, DDS, A. Guerrero, DDS, T. Ngo, DDS, A. Helfer, DDS, MSD and G. Hasselgren, DDS, PhD (January 1, 2006), "Inability of laser and rotary instrumentation to eliminate root canal infection", Journal of American Dental Association 137 (1): 67–70, doi:10.14219/jada.archive.2006.0023, PMID 16457001
- ↑ Laser Root Canal Treatment. What is it and is it good?
- ↑ Johnson, William B. (May 24, 1988), United States Patent 4,746,292: Tool and method for removing a parted endodontic file
- ↑ Torabinejad, Mahmoud, Richard Walton. Endodontics, 4th Edition.Page 265. W.B. Saunders Company, 2008. VitalBook file
- ↑ 19.0 19.1 Hülsmann M, Hahn W (2000). "Complications during root canal irrigation--literature review and case reports". Int Endod J (Review) 33 (3): 186–93. doi:10.1046/j.1365-2591.2000.00303.x. PMID 11307434. Vancouver style error (help)
- ↑ Friedman S, Mor C (2004), "The success of endodontic therapy: healing and functionality", J Calif Dent Assoc 32 (6): 493–503, PMID 15344440.
- ↑ G Tang, LP Samaranayake, H-K Yip (2004), "Molecular evaluation of residual endodontic microorganisms after instrumentation, irrigation and medication with either calcium hydroxide or Septomixine", Oral Diseases 6 (10): 389–397, doi:10.1111/j.1601-0825.2004.01015.x, PMID 15533217
- ↑ Rotstein I., Salehrabi R. (December 2004), "Endodontic treatment outcomes in a large patient population in the USA: an epidemiological study", Journal of Endodontics 12 (30): 846–50
- ↑ Baumgartner JC, Bakland LK, Sugita EI (2002), Endodontics, Chapter 3: Microbiology of endodontics and asepsis in endodontic practice (PDF), Hamilton, Ontario: BC Becker, pp. 63–94, retrieved 2009-11-27
External links
| Wikiversity has learning materials about Endodontics |
- An animated review of root canal treatment.
- Comparison of antibacterial and toxic effects of various root canal irrigants.
- Endodontic treatment of teeth associated with a large periapical lesion.
- What does root canal treatment feel like from a patient's perspective?
- Concept of predictable disinfection in endodontics
| Wikimedia Commons has media related to Root canal. |
| ||||||||||||||||||||||||||||||||