Effective dose (radiation)
The radiation dose quantity effective dose is the tissue-weighted sum of the equivalent doses in all specified tissues and organs of the body and represents the stochastic health risk, which the probability of cancer induction and genetic effects of ionizing radiation delivered to those body parts.[1][2] It takes into account the type of radiation and the nature of each organ or tissue being irradiated.
It is the central quantity for dose limitation in radiological protection in the international system of radiological protection devised by the International Commission on Radiological Protection (ICRP).[3] The effective dose is not intended as a measure of deterministic health effect, which is the severity of acute tissue damage that is certain to happen.[4]
The SI unit for effective dose is the sievert (Sv) which is one joule/kilogram (J/kg). The effective dose replaced the former "effective dose equivalent" in 1991 in the ICRP system of dose quantities.[5]
Use
According to the ICRP, the main uses of effective dose are the prospective dose assessment for planning and optimisation in radiological protection, and demonstration of compliance with dose limits for regulatory purposes. The effective dose is thus a central dose quantity for regulatory purposes. [6]
The UK Ionising Radiations Regulations 1999 state; "Any reference to an effective dose means the sum of the effective dose to the whole body from external radiation and the committed effective dose from internal radiation." [7]
The ICRP also states that effective dose has made a significant contribution to radiological protection as it has enabled doses to be summed from whole and partial body exposure from external radiation of various types and from intakes of radionuclides.[8]
Use for external dose
The calculation of effective dose is required for partial or non-uniform irradiation of the human body because equivalent dose does not consider the tissue irradiated, but only the radiation type. Various body tissues react to ionizing radiation in different ways, so the ICRP has assigned sensitivity factors to specified tissues and organs so that the effect of partial irradiation can be calculated if the irradiated regions are known.[9] A radiation field irradiating only a portion of the body will carry lower risk than if the same field irradiated the whole body. To take this into account, the effective doses to the component parts of the body which have been irradiated are calculated and summed. This becomes the effective dose for the whole body, dose quantity E. It is a "protection" dose quantity which can be calculated, but cannot be measured in practice.
An effective dose will carry the same effective risk to the whole body regardless of where it was applied, and it will carry the same effective risk as the same amount of equivalent dose applied uniformly to the whole body.
Use for internal dose
Effective dose can be calculated for committed dose which is the internal dose resulting from inhaling, ingesting, or injecting radioactive materials.
The dose quantity used is:
Committed effective dose, E(t) is the sum of the products of the committed organ or tissue equivalent doses and the appropriate tissue weighting factors WT, where t is the integration time in years following the intake. The commitment period is taken to be 50 years for adults, and to age 70 years for children.[10]
Calculation of effective dose
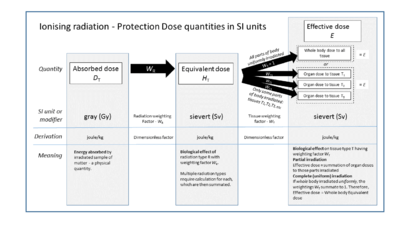
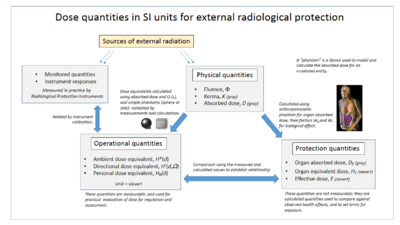
Ionising radiation deposits energy in the matter being irradiated. The quantity used to express this is the absorbed dose, a physical dose quantity that is independent of radiation type and tissue type. To allow consideration of the stochastic radiological risk, the dose quantities equivalent dose and effective dose have been devised by the International Commission on Radiation Units and Measurements (ICRU) and the ICRP to calculate the biological effect of an absorbed dose.
To obtain an effective dose, the absorbed organ dose DT is first corrected for the radiation type using factor WR to give a weighted average of the equivalent dose quantity HT received in irradiated body tissues, and the result is further corrected for the tissues or organs being irradiated using factor WT, to produce the effective dose quantity E.
The sum of effective doses to all organs and tissues of the body represents the effective dose for the whole body. If only part of the body is irradiated, then only those regions are used to calculate the effective dose. The tissue weighting factors summate to 1.0, so that if an entire body is radiated with uniformly penetrating external radiation, the effective dose for the entire body is equal to the equivalent dose for the entire body.
Use of tissue weighting factor WT
The ICRP tissue weighting factors are given in the accompanying table, and the equations used to calculate from either absorbed dose or equivalent dose are also given.
Some tissues like bone marrow are particularly sensitive to radiation, so they are given a weighting factor that is disproportionally large relative to the fraction of body mass they represent. Other tissues like the hard bone surface are particularly insensitive to radiation and are assigned a disproportionally low weighting factor.
| Organs | Tissue weighting factors | ||
|---|---|---|---|
| ICRP26 1977 | ICRP60 1990[12] | ICRP103 2007[13] | |
| Gonads | 0.25 | 0.20 | 0.08 |
| Red Bone Marrow | 0.12 | 0.12 | 0.12 |
| Colon | - | 0.12 | 0.12 |
| Lung | 0.12 | 0.12 | 0.12 |
| Stomach | - | 0.12 | 0.12 |
| Breasts | 0.15 | 0.05 | 0.12 |
| Bladder | - | 0.05 | 0.04 |
| Liver | - | 0.05 | 0.04 |
| Oesophagus | - | 0.05 | 0.04 |
| Thyroid | 0.03 | 0.05 | 0.04 |
| Skin | - | 0.01 | 0.01 |
| Bone surface | 0.03 | 0.01 | 0.01 |
| Salivary glands | - | - | 0.01 |
| Brain | - | - | 0.01 |
| Remainder of body | 0.30 | 0.05 | 0.12 |
| Total | 1.00 | 1.00 | 1.00 |
Calculating from the equivalent dose:
 .
.
Calculating from the absorbed dose:

Where
 is the effective dose to the entire organism
is the effective dose to the entire organism is the equivalent dose absorbed by tissue T
is the equivalent dose absorbed by tissue T is the tissue weighting factor defined by regulation
is the tissue weighting factor defined by regulation is the radiation weighting factor defined by regulation
is the radiation weighting factor defined by regulation is the mass-averaged absorbed dose in tissue T by radiation type R
is the mass-averaged absorbed dose in tissue T by radiation type R is the absorbed dose from radiation type R as a function of location
is the absorbed dose from radiation type R as a function of location is the density as a function of location
is the density as a function of location is volume
is volume is the tissue or organ of interest
is the tissue or organ of interest
The ICRP tissue weighting factors are chosen to represent the fraction of health risk, or biological effect, which is attributable to the specific tissue named. These weighting factors have been revised twice, as shown in the chart above.
The US Nuclear Regulatory Commission still endorses the ICRP's 1977 tissue weighting factors in their regulations, in spite of the ICRP's later revised recommendations.[14]
Related Quantities
US Effective Dose Equivalent
The US Nuclear Regulatory Commission has retained in the US regulation system the older term effective dose equivalent to refer to a similar quantity to the ICRP effective dose. The NRC's total effective dose equivalent (TEDE) is the sum of external effective dose with internal committed dose; in other words all sources of dose.
Cumulative equivalent
Cumulative equivalent dose due to external whole-body exposure is normally reported to nuclear energy workers in regular dosimetry reports. In the US, three different effective doses are typically reported:
- deep-dose equivalent, (DDE) which is properly a whole-body equivalent dose
- shallow dose equivalent, (SDE) which is actually the effective dose to the skin
- eye dose equivalent (not defined in the NRC glossary)
Increased Cancer Risk
One sievert (100 rem) of effective dose carries with it a 4% chance of developing a fatal cancer in an average adult, and a 0.8% chance of hereditary defect in future offspring. This average is used in radiation protection although the risk to a given exposed individual depends on many factors, particularly age as cancers may develop years or decades after exposure. There is also an increased risk of survivable cancers, including some that will never be diagnosed.
The Biologic Effects of Ionizing Radiation (BEIR) reports contain the relationship between dose and cancer calculated largely from dose reconstructions for A-bomb survivors.[15][16]
History
The concept of effective dose was introduced in 1975.[17] It was then included in 1977 as “effective dose equivalent” into Publication 26 by the ICRP. In 1991, ICRP publication 60 shortened the name to "effective dose." [18] This quantity is sometimes incorrectly referred to as the "dose equivalent" because of the earlier name, and that misnomer in turn causes confusion with equivalent dose. The tissue weighting factors were revised in 1990 and 2007 because of new data.
References
- ↑ ICRP publication 103, glossary
- ↑ ICRP publication 103, para 104 and 105
- ↑ ICRP publication, 103 para 103
- ↑ ICRP report 103 para 104 and 105
- ↑ ICRP publication 103 executive summary para 101
- ↑ ICRP publication 103 executive summary para j
- ↑ The UK Ionising Radiations Regulations 1999
- ↑ ICRP publication 103 para 101
- ↑ ICRP publication 103, para 22 & glossary
- ↑ ICRP publication 103 - Glossary.
- ↑ UNSCEAR-2008 Annex A page 40, table A1, retrieved 2011-7-20
- ↑ "1990 Recommendations of the International Commission on Radiological Protection". Annals of the ICRP. ICRP publication 60 21 (1-3). 1991. ISBN 978-0-08-041144-6. Retrieved 17 May 2012.
- ↑ "The 2007 Recommendations of the International Commission on Radiological Protection". Annals of the ICRP. ICRP publication 103 37 (2-4). 2007. ISBN 978-0-7020-3048-2. Retrieved 17 May 2012.
- ↑ 10 CFR 20.1003. US Nuclear Regulatory Commission. 2009. Retrieved 25 November 2012.
- ↑ "Report in Brief Beir VII: Health Risks from Exposure to Low Levels of Ionizing Radiation". Earth and Life Studies at the National Academies. The National Academies. Retrieved 25 August 2012.
- ↑ Health Risks from Exposure to Low Levels of Ionizing Radiation: BEIR VII – Phase 2. National Academies Press. 2006. p. 248. ISBN 0-309-53040-7.
- ↑ Jacobi W (1975). "The concept of effective dose - A proposal for the combination of organ doses". Radiat. Environ. Biophys (12): 101–109.
- ↑ ICRP publication 103 paragraph 101
See also
- Radioactivity
- Collective dose
- Total effective dose equivalent
- Deep-dose equivalent
- Cumulative dose
- Committed dose equivalent
- Committed effective dose equivalent
External links
- "The confusing world of radiation dosimetry" - M.A. Boyd, U.S. Environmental Protection Agency. An account of chronological differences between USA and ICRP dosimetry systems.
| ||||||||||||||||||||||||||||