Cytochrome P450 reductase

Cytochrome P450 reductase [1] (EC 1.6.2.4; also known as NADPH:ferrihemoprotein oxidoreductase, NADPH:hemoprotein oxidoreductase, NADPH:P450 oxidoreductase, P450 reductase, POR, CPR, CYPOR) is a membrane-bound enzyme required for electron transfer from NADPH to cytochrome P450 in the endoplasmic reticulum[2] of the eukaryotic cell.
Function
| NADPH-hemoprotein reductase | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Identifiers | |||||||||
| EC number | 1.6.2.4 | ||||||||
| CAS number | 9023-03-4 | ||||||||
| Databases | |||||||||
| IntEnz | IntEnz view | ||||||||
| BRENDA | BRENDA entry | ||||||||
| ExPASy | NiceZyme view | ||||||||
| KEGG | KEGG entry | ||||||||
| MetaCyc | metabolic pathway | ||||||||
| PRIAM | profile | ||||||||
| PDB structures | RCSB PDB PDBe PDBsum | ||||||||
| Gene Ontology | AmiGO / EGO | ||||||||
| |||||||||
In Bacillus megaterium and Bacillus subtilis, POR is a C-terminal domain of CYP102, a single-polypeptide self-sufficient soluble P450 system (P450 is an N-terminal domain). The general scheme of electron flow in the POR/P450 system is:
The definitive evidence for the requirement of POR in cytochrome-P450-mediated reactions came from the work of Lu, Junk and Coon,[3] who dissected the P450-containing mixed function oxidase system into three constituent components: POR, cytochrome P450, and lipids.
Since all microsomal P450 enzymes require POR for catalysis, it is expected that disruption of POR would have devastating consequences. POR knockout mice are embryonic lethal,[4] probably due to lack of electron transport to extrahepatic P450 enzymes since liver-specific knockout of POR yields phenotypically and reproductively normal mice that accumulate hepatic lipids and have remarkably diminished capacity of hepatic drug metabolism.[5]
The reduction of cytochrome P450 is not the only physiological function of POR. The final step of heme oxidation by mammalian heme oxygenase requires POR and O2. In yeast, POR affects the ferrireductase activity, probably transferring electrons to the flavocytochrome ferric reductase.[6]
Gene organization
Human POR gene has 16 exons and the exons 2-16 code for a 677-amino acid [7] POR protein (NCBI NP_000932.2). There is a single copy of 50 kb POR gene (NCBI NM_000941.2) in humans on chromosome 7 (7q11.23).
Mutations and polymorphisms
Five missense mutations (A284P, R454H, V489E, C566Y, and V605F) and a splicing mutation in the POR genes have been found in patients who had hormonal evidence for combined deficiencies of two steroidogenic cytochrome P450 enzymes - P450c17 CYP17A1, which catalyzes steroid 17α-hydroxylation and 17,20 lyase reaction, and P450c21 21-Hydroxylase, which catalyzes steroid 21-hydroxylation.[8] Another POR missense mutation Y178D has also been identified.[9] Fifteen of nineteen patients having abnormal genitalia and disordered steroidogenesis were homozygous or apparent compound heterozygous for POR mutations that destroyed or dramatically inhibited POR activity.[10]
POR Deficiency – Mixed Oxidase Disease
POR deficiency is the newest form of congenital adrenal hyperplasia first described in 2004.[8] The index patient was a newborn 46,XX Japanese girl with craniosynostosis, hypertelorism, mid-face hypoplasia, radiohumeral synostosis, arachnodactyly and disordered steroidogenesis. However, the clinical and biochemical characteristics of patients with POR deficiency are long known in the literature as so-called mixed oxidase disease, as POR deficiency typically shows a steroid profile that suggests combined deficiencies of steroid 21-hydroxylase and 17α-hydroxylase/17,20 lyase activities. The clinical spectrum of POR deficiency ranges from severely affected children with ambiguous genitalia, adrenal insufficiency, and the Antley-Bixler skeletal malformation syndrome (ABS) to mildly affected individuals with polycystic ovary syndrome-like features. Some of the POR patients were born to mothers who became virilized during pregnancy, suggesting deficient placental aromatization of fetal androgens due to a lesion in microsomal aromatase resulting in low estrogen production, which was later confirmed by lower aromatase activities caused by POR mutations.[11] However, it has also been suggested that fetal and maternal virilization in POR deficiency might be caused by increased dihydrotestosterone synthesis by the fetal gonad through an alternative "backdoor" pathway first described in the marsupials and later confirmed in humans .[12] Gas chromatography/mass spectrometry analysis of urinary steroids from pregnant women carrying a POR-deficient fetus described in an earlier report also supports the existence of this pathway,[13] and the relevance of the "backdoor" pathway along with POR dependent steroidogenesis have become clearer from recent studies.[12] The role of POR mutations beyond CAH are being investigated; and questions such as how POR mutations cause bony abnormalities and what role POR variants play in drug metabolism by hepatic P450s are being addressed in recent publications.[14][15][16][17][18] However, reports of ABS in some offsprings of mothers who were treated with fluconazole, an antifungal agent which interferes with cholesterol biosynthesis at the level of CYP51 activity - indicate that disordered drug metabolism may result from deficient POR activity.
Williams syndrome
Williams syndrome is a genetic disorder characterized by the deletion of genetic material approximately 1.2 Mb from the POR gene (POR). Cells with this genetic deletion show reduced transcription of POR, it seems, due to the loss of a cis-regulatory element that alters expression of this gene.[19] Some persons with Williams syndrome show characteristics of POR deficiency, including radio-ulnar synostosis and other skeletal abnormalities.[20] Cases of mild impairment of cortisol and androgen synthesis have been noted,[21] however, despite the fact that deficient POR impairs androgen synthesis, patients with Williams syndrome often show increased androgen levels.[22] A similar increase in testosterone has been observed in a mouse model that has globally decreased POR expression.[23]
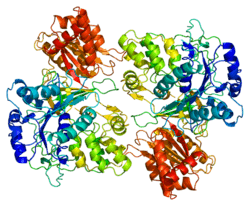
Structure
The 3D crystal structure of human POR has been determined.[24] The molecule is composed of four structural domains: the FMN-binding domain, the connecting domain, the FAD-binding domain, and NADPH-binding domain. The FMN-binding domain is similar to the structure of FMN-containing protein flavodoxin, whereas the FAD-binding domain and NADPH-binding domains are similar to those of flavoprotein ferredoxin-NADP+ reductase (FNR). The connecting domain is situated between the flavodoxin-like and FNR-like domains.
POR homologs
The other enzymes containing homologs of POR are nitric oxide synthase (EC 1.14.13.39), NADPH:sulfite reductase (EC 1.8.1.2), and methionine synthase reductase (EC 1.16.1.8).
See also
References
- ↑ Pandey AV, Flück CE (May 2013). "NADPH P450 oxidoreductase: structure, function, and pathology of diseases.". Pharmacology & therapeutics 138 (2): 229–54. doi:10.1016/j.pharmthera.2013.01.010. PMID 23353702.
- ↑ Jensen K, Møller BL (February 2010). "Plant NADPH-cytochrome P450 oxidoreductases". Phytochemistry 71 (2-3): 132–41. doi:10.1016/j.phytochem.2009.10.017. PMID 19931102.
CPR was shown to be localized in the endoplasmic reticulum in the early 1960s (Williams and Kamin, 1962).
- ↑ Lu AY, Junk KW, Coon MJ (1969). "Resolution of the cytochrome P-450-containing ω-hydroxylation system of liver microsomes into three components". J. Biol. Chem. 244 (13): 3714–3721. PMID 4389465.
- ↑ Shen AL, O'Leary KA, Kasper CB (2002). "Association of multiple developmental defects and embryonic lethality with loss of microsomal NADPH-cytochrome P450 oxidoreductase". J. Biol. Chem. 277 (8): 6536–6541. doi:10.1074/jbc.M111408200. PMID 11742006.
- ↑ Gu J, Weng Y, Zhang QY, Cui H, Behr M, Wu L, Yang W, Zhang L, Ding X (July 2003). "Liver-specific deletion of the NADPH-cytochrome P450 reductase gene: impact on plasma cholesterol homeostasis and the function and regulation of microsomal cytochrome P450 and heme oxygenase". J. Biol. Chem. 278 (28): 25895–901. doi:10.1074/jbc.M303125200. PMID 12697746.
- ↑ Lesuisse E, Casteras-Simon M, Labbe P (November 1997). "Cytochrome P-450 reductase is responsible for the ferrireductase activity associated with isolated plasma membranes of Saccharomyces cerevisiae". FEMS Microbiol. Lett. 156 (1): 147–52. doi:10.1016/S0378-1097(97)00418-7. PMID 9368374.
- ↑ Haniu M, McManus ME, Birkett DJ, Lee TD, Shively JE (1989). "Structural and functional analysis of NADPH-cytochrome P-450 reductase from human liver: complete sequence of human enzyme and NADPH-binding sites". Biochemistry 28 (21): 8639–8645. doi:10.1021/bi00447a054. PMID 2513880.
- ↑ 8.0 8.1 Flück CE, Tajima T, Pandey AV, Arlt W, Okuhara K, Verge CF, Jabs EW, Mendonça BB, Fujieda K, Miller WL (2004). "Mutant P450 oxidoreductase causes disordered steroidogenesis with and without Antley-Bixler syndrome". Nature Genetics 36 (3): 228–230. doi:10.1038/ng1300. PMID 14758361.
- ↑ Arlt W, Walker EA, Draper N, Ivison HE, Ride JP, Hammer F, Chalder SM, Borucka-Mankiewicz M, Hauffa BP, Malunowicz EM, Stewart PM, Shackleton CH (2004). "Congenital adrenal hyperplasia caused by mutant P450 oxidoreductase and human androgen synthesis: analytical study". Lancet 363 (9427): 2128–2135. doi:10.1016/S0140-6736(04)16503-3. PMID 15220035.
- ↑ Huang N, Pandey AV, Agrawal V, Reardon W, Lapunzina PD, Mowat D, Jabs EW, Van Vliet G, Sack J, Flück CE, Miller WL (2005). "Diversity and function of mutations in P450 oxidoreductase in patients with Antley-Bixler syndrome and disordered steroidogenesis". Am. J. Hum. Genet. 76 (5): 729–749. doi:10.1086/429417. PMC 1199364. PMID 15793702.
- ↑ Pandey AV, Kempná P, Hofer G, Mullis PE, Flück CE (October 2007). "Modulation of human CYP19A1 activity by mutant NADPH P450 oxidoreductase". Mol. Endocrinol. 21 (10): 2579–95. doi:10.1210/me.2007-0245. PMID 17595315.
- ↑ 12.0 12.1 Flück CE, Meyer-Böni M, Pandey AV, Kempná P, Miller WL, Schoenle EJ, Biason-Lauber A (August 2011). "Why boys will be boys: two pathways of fetal testicular androgen biosynthesis are needed for male sexual differentiation". Am. J. Hum. Genet. 89 (2): 201–18. doi:10.1016/j.ajhg.2011.06.009. PMC 3155178. PMID 21802064.
- ↑ Shackleton C, Marcos J, Arlt W, Hauffa BP (August 2004). "Prenatal diagnosis of P450 oxidoreductase deficiency (ORD): a disorder causing low pregnancy estriol, maternal and fetal virilization, and the Antley-Bixler syndrome phenotype". Am. J. Med. Genet. A 129A (2): 105–12. doi:10.1002/ajmg.a.30171. PMID 15316970.
- ↑ Flück CE, Mullis PE, Pandey AV (October 2010). "Reduction in hepatic drug metabolizing CYP3A4 activities caused by P450 oxidoreductase mutations identified in patients with disordered steroid metabolism". Biochem. Biophys. Res. Commun. 401 (1): 149–53. doi:10.1016/j.bbrc.2010.09.035. PMID 20849814.
- ↑ Tomalik-Scharte D, Maiter D, Kirchheiner J, Ivison HE, Fuhr U, Arlt W (December 2010). "Impaired hepatic drug and steroid metabolism in congenital adrenal hyperplasia due to P450 oxidoreductase deficiency". Eur. J. Endocrinol. 163 (6): 919–24. doi:10.1530/EJE-10-0764. PMC 2977993. PMID 20844025.
- ↑ Nicolo C, Flück CE, Mullis PE, Pandey AV (June 2010). "Restoration of mutant cytochrome P450 reductase activity by external flavin". Mol. Cell. Endocrinol. 321 (2): 245–52. doi:10.1016/j.mce.2010.02.024. PMID 20188793.
- ↑ Sandee D, Morrissey K, Agrawal V, Tam HK, Kramer MA, Tracy TS, Giacomini KM, Miller WL (November 2010). "Effects of genetic variants of human P450 oxidoreductase on catalysis by CYP2D6 in vitro". Pharmacogenet. Genomics 20 (11): 677–86. doi:10.1097/FPC.0b013e32833f4f9b. PMID 20940534.
- ↑ Agrawal V, Choi JH, Giacomini KM, Miller WL (October 2010). "Substrate-specific modulation of CYP3A4 activity by genetic variants of cytochrome P450 oxidoreductase". Pharmacogenet. Genomics 20 (10): 611–8. doi:10.1097/FPC.0b013e32833e0cb5. PMC 2940949. PMID 20697309.
- ↑ Merla G, Howald C, Henrichsen CN, Lyle R, Wyss C, Zabot MT, Antonarakis SE, Reymond A (August 2006). "Submicroscopic deletion in patients with Williams-Beuren syndrome influences expression levels of the nonhemizygous flanking genes". Am. J. Hum. Genet. 79 (2): 332–41. doi:10.1086/506371. PMC 1559497. PMID 16826523.
- ↑ Charvat KA, Hornstein L, Oestreich AE (1991). "Radio-ulnar synostosis in Williams syndrome. A frequently associated anomaly". Pediatr Radiol 21 (7): 508–10. doi:10.1007/bf02011725. PMID 1771116.
- ↑ Ichinose M, Tojo K, Nakamura K, Matsuda H, Tokudome G, Ohta M, Sakai S, Sakai O (June 1996). "Williams syndrome associated with chronic renal failure and various endocrinological abnormalities". Intern. Med. 35 (6): 482–8. doi:10.2169/internalmedicine.35.482. PMID 8835601.
- ↑ Partsch CJ, Pankau R, Blum WF, Gosch A, Wessel A (July 1994). "Hormonal regulation in children and adults with Williams-Beuren syndrome". Am. J. Med. Genet. 51 (3): 251–7. doi:10.1002/ajmg.1320510316. PMID 8074154.
- ↑ Wu L, Gu J, Cui H, Zhang QY, Behr M, Fang C, Weng Y, Kluetzman K, Swiatek PJ, Yang W, Kaminsky L, Ding X (January 2005). "Transgenic mice with a hypomorphic NADPH-cytochrome P450 reductase gene: effects on development, reproduction, and microsomal cytochrome P450". J. Pharmacol. Exp. Ther. 312 (1): 35–43. doi:10.1124/jpet.104.073353. PMID 15328377.
- ↑ PDB 3QE2); Xia C, Panda SP, Marohnic CC, Martásek P, Masters BS, Kim JJ (August 2011). "Structural basis for human NADPH-cytochrome P450 oxidoreductase deficiency". Proc. Natl. Acad. Sci. U.S.A. 108 (33): 13486–91. doi:10.1073/pnas.1106632108. PMC 3158178. PMID 21808038.
External links
- Cytochrome P450 Reductase at the US National Library of Medicine Medical Subject Headings (MeSH)
- GeneReviews/NCBI/NIH/UW entry on Cytochrome P450 Oxidoreductase Deficiency
| ||||||||||||||||||||||||||||||||||||
| ||||||
| |||||||||||||||||||||||||||||||||