Cystic duct
| Cystic duct | |
|---|---|
 1: Right lobe of liver 2: Left lobe of liver 3: Quadrate lobe of liver 4: Round ligament of liver 5: Falciform ligament 6: Caudate lobe of liver 7: Inferior vena cava 8: Common bile duct 9: Hepatic artery 10: Portal vein 11: Cystic duct 12: Hepatic duct 13: Gallbladder | |
| Details | |
| Latin | ductus cysticus |
| cystic artery | |
| Identifiers | |
| Gray's | p.1198 |
| Dorlands /Elsevier | d_29/12314797 |
| TA | A05.8.02.011 |
| FMA | 14539 |
| Anatomical terminology | |
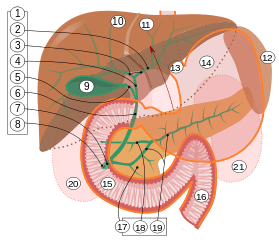
9. Gallbladder, 10–11. Right and left lobes of liver. 12. Spleen.
13. Esophagus. 14. Stomach. Small intestine: 15. Duodenum, 16. Jejunum
17. Pancreas: 18: Accessory pancreatic duct, 19: Pancreatic duct.
20–21: Right and left kidneys (silhouette).
The anterior border of the liver is lifted upwards (brown arrow). Gallbladder with Longitudinal section, pancreas and duodenum with frontal one. Intrahepatic ducts and stomach in transparency.
The cystic duct is the short duct that joins the gallbladder to the common bile duct. It usually lies next to the cystic artery. It is of variable length. It contains 'spiral valves of Heister,' which do not provide much resistance to the flow of bile.
Function
Bile can flow in both directions between the gallbladder and the common hepatic duct and the (common) bile duct.
In this way, bile is stored in the gallbladder in between meal times. The hormone cholecystokinin, when stimulated by a fatty meal, promotes bile secretion by increased production of hepatic bile, contraction of the gall bladder, and relaxation of the Sphincter of Oddi.
Clinical significance
Gallstones can enter and obstruct the cystic duct, preventing the flow of bile. The increased pressure in the gallbladder leads to swelling and pain. This pain, known as biliary colic, is sometimes referred to as a gallbladder "attack" because of its sudden onset.
During a cholecystectomy, the cystic duct is clipped two or three times and a cut is made between the clips, freeing the gallbladder to be taken out.
Postoperative cystic duct stump leaks
A postoperative cystic duct stump leak (CDSL) is a leak from the cystic duct stump in post cholecystectomy patients. It was rarely reported in open cholecystectomy patients. Since the advent of laparoscopic cholecystectomy the incidence of CDSL has increased with one study doing it to occur in 0.1 to 0.2% of patients.[1] Cystic duct stump leak is the commonest cause of bile leak and technical morbidity according to one study.[2] The cause may be not related the presence of emergency laparoscopic cholecystecomies as one study showed that only 46.6% of CDSL occurred with acute cholecystitis.[3]
Theories of the CDSL include:
1. Cystic duct displacement:
- 1a. Improper firing can cause the clip to displace as one study showed clipless cystic ducts after placement of 2 cystic duct clips.[4][5]
- 1b. Cystic duct displacement could be due to abnormal cystic duct morphological features. This could place constrictions which thus could lead to improper firing. A solution is to suture the duct or as last resort leave a T tube or Jackson-pratt drain intraoperatively.
2. Necrosis of cystic duct stump proximal to clip: This would occur proximal to the applied clip. Necrosis may be secondary to electrocautery creating a phenomenon called "clip-coupling" in which excessive electrocautery near the clips, conducted via the metal in the clips, causes necrosis of the proximal cystic duct.[6]
3. Ischemic necrosis secondary to devascularization: One study showed that blood flow can be disrupted from dissecting. One study showed a pseudoaneurysm of the right hepatic artery causing vascular disrupting blood supply to the cystic duct. A solution is dividing the cystic artery distally.[7]
4. Increased biliary pressure: This can be due to a retained common bile duct stone creating pressure in the biliary tree. This may be the most rare causes of CDSL.[8]
CDSL presentation
CDSL presents 3 to 4 days after operation with right upper quadrant pain, followed by nausea, vomiting, and fever. High WBC is described in 68% of patient. Liver function tests can be highly variable.[9]
Diagnosis and treatment of CDSL
Initial test is ultrasonography to screen out biloma, ascites, or retained stones. Computed tomgraphy has a high sensitivity approaching 100% for detecting leaks. The most successful imaging is from ERCP. ERCP has the additional value of allowing for treatment which often consists of sphincterotomy with common bile duct stenting.
See also
Additional images
-

Digestive system diagram showing the cystic duct
-
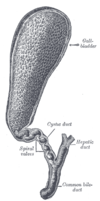
The gall-bladder and bile ducts laid open.
-
The portal vein and its tributaries.
-

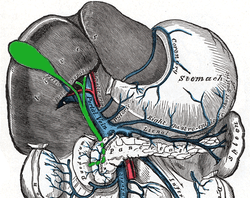
Cystic duct.Visceral surface of liver.
References
- ↑ http://archsurg.jamanetwork.com/article.aspx?articleid=402269
- ↑ http://onlinelibrary.wiley.com/doi/10.1111/j.1751-2980.2009.00387.x/full
- ↑ Wise Unger, S; Glick, G. L.; Landeros, M (1996). "Cystic duct leak after laparoscopic cholecystectomy. A multi-institutional study". Surgical endoscopy 10 (12): 1189–93. PMID 8939840.
- ↑ Hanazaki, K; Igarashi, J; Sodeyama, H; Matsuda, Y (1999). "Bile leakage resulting from clip displacement of the cystic duct stump: A potential pitfall of laparoscopic cholecystectomy". Surgical endoscopy 13 (2): 168–71. PMID 9918624.
- ↑ Li, J. H.; Liu, H. T. (2005). "Diagnosis and management of cystic duct leakage after laparoscopic cholecystectomy: Report of 3 cases". Hepatobiliary & pancreatic diseases international : HBPD INT 4 (1): 147–51. PMID 15730941.
- ↑ Woods, M. S.; Shellito, J. L.; Santoscoy, G. S.; Hagan, R. C.; Kilgore, W. R.; Traverso, L. W.; Kozarek, R. A.; Brandabur, J. J. (1994). "Cystic duct leaks in laparoscopic cholecystectomy". American journal of surgery 168 (6): 560–3; discussion 563–5. PMID 7977996.
- ↑ http://archsurg.jamanetwork.com/article.aspx?articleid=402269
- ↑ http://archsurg.jamanetwork.com/article.aspx?articleid=402269
- ↑ http://archsurg.jamanetwork.com/article.aspx?articleid=402269#ref-soa70074-3
External links
- cystic+duct at eMedicine Dictionary
- Anatomy figure: 38:06-03 at Human Anatomy Online, SUNY Downstate Medical Center - "The gallbladder and extrahepatic bile ducts."
- Anatomy photo:38:14-0106 at the SUNY Downstate Medical Center - "Stomach, Spleen and Liver: The Gallbladder and the Bile System"
- liver at The Anatomy Lesson by Wesley Norman (Georgetown University) (liverinferior, biliarysystem)
{kind=link}
{kind=link}
| ||||||||||||||||||||||||||||||||||||||