Ageing
| Part of a series on |
| Human growth and development |
|---|
| Stages |
| Biological milestones |
| Ageing | |
|---|---|
 A human face showing signs of ageing | |
| Classification and external resources | |
| MeSH | D000375 |
Ageing (British English) or aging (American English) is the process of becoming older. It represents the accumulation of changes in a person over time.[1][2] In humans, ageing refers to a multidimensional process of physical, psychological, and social change. Reaction time, for example, may slow with age, while knowledge of world events and wisdom may expand. Ageing is an important part of all human societies reflecting the biological changes that occur, but also reflecting cultural and societal conventions. Ageing is among the largest known risk factors for most human diseases.[3] Roughly 100,000 people worldwide die each day of age-related causes.[4]
Population ageing is the increase in the number and proportion of older people in society. Population ageing has three possible causes: migration, longer life expectancy (decreased death rate) and decreased birth rate. Ageing has a significant impact on society. Young people tend to have fewer legal privileges (if they are below the age of majority), they are more likely to push for political and social change, to develop and adopt new technologies, and to need education. Older people have different requirements from society and government, and frequently have differing values as well, such as for property and pension rights.[5]
Recent scientific successes in rejuvenation and extending the lifespan of model animals (mice 2.5 times, yeast and nematodes 10 times) and discovery of variety of species (including humans of advanced ages) having negligible senescence give hope to achieve negligible senescence (cancel ageing) for younger humans, reverse ageing, or at least significantly delay it. Regenerative medicine is a branch of medicine associated with the treatment of age-related diseases. Ageing is the major cause of mortality in the developed world.[6][7]
Senescence
In biology, senescence is the state or process of ageing. Cellular senescence is a phenomenon where isolated cells demonstrate a limited ability to divide in culture (the Hayflick Limit, discovered by Leonard Hayflick in 1961), while organismal senescence is the ageing of organisms. After a period of near perfect renewal (in humans, between 20 and 35 years of age), organismal senescence is characterised by the declining ability to respond to stress, increasing homeostatic imbalance and the increased risk of disease. Ageing is among the largest known risk factors for most human diseases.[3] This currently irreversible series of changes inevitably ends in death. Some researchers (specifically biogerontologists) are treating ageing as a disease. As genes that have an effect on ageing are discovered, ageing is increasingly being regarded in a similar fashion to other genetically influenced "conditions," potentially "treatable".
There are three main metabolic pathways which influence the rate of ageing: caloric restriction, the insulin/IGF-1-like signalling pathway, and the activity levels of the electron transport chain. Before these were discovered, ageing was considered to be a progressive decline in function. It is likely that these three pathways affect ageing separately, because targeting them simultaneously leads to additive increases in lifespan.[8]
Ageing and longevity are determined by a complex mixture of environmental and genetic factors. The genetic aspect has been demonstrated in studies of centenarians, and in model organisms where single-gene mutations have been shown to dramatically increase lifespan. These genes have homologues in the mammalian genome, making them useful both in studying ageing and in identifying potential targets for interventions which increase lifespan. These genes also increase lifespan in mice, and in some cases have been shown to associate with human longevity.[9]
Numerous species show very low signs of ageing ("negligible senescence"), the best known being trees like the bristlecone pine (however Hayflick states that the bristlecone pine has no cells older than 30 years), fish like the sturgeon and the rockfish, invertebrates like the quahog and sea anemone[10] and lobster.[11][12]
In humans and other animals, cellular senescence has been attributed to the shortening of telomeres with each cell cycle; when telomeres become too short, the cells die. The length of telomeres is therefore the "molecular clock", predicted by Hayflick. The quantity of the hematopoietic stem cells that produce the blood components residing in the bone marrow of human beings have been found to decline with ageing.[13] Stem cells regenerative capacity is affected by the age of the recipient.[2]
Other genes are known to affect the ageing process. The sirtuin family of genes have been shown to have a significant effect on the lifespan of yeast and nematodes. Over-expression of the RAS2 gene increases lifespan in yeast by 30%.[14]
In addition to genetic ties to lifespan, diet (specifically, caloric restriction) has been shown to substantially affect lifespan in many animals, including delay or prevention of many age-related diseases.[15] Typically, this involves caloric intake to 60–70% of what an ad libitum animal would consume, while still maintaining proper nutrient intake.[15] In rodents, it has been shown to increase lifespan by up to 50%;[16] it also works for many other species beyond mice, including species as diverse as yeast and Drosophila,[15] and likely includes primates as well.[15][17][18] There are two major studies of caloric restriction being performed in rhesus monkeys, one at the US National Institutes of Health, and the other at the University of Wisconsin-Madison.[17] The basis for caloric restriction remains unclear,[8] though it is likely mediated by nutrient-sensing pathways such as the mTOR pathway.[18]
Evidence in both animals and humans suggests that resveratrol may be a caloric restriction mimetic.[19]
In his book How and Why We Age, Hayflick says that caloric restriction may not be effective in humans, citing data from the Baltimore Longitudinal Study of Aging which shows that being thin does not favour longevity.[20]
Of the roughly 150,000 people who die each day across the globe, about two thirds—100,000 per day—die of age-related causes.[4] In industrialised nations, the proportion is much higher, reaching 90%.[4]
Biological basis of ageing

At present, the biological basis of ageing is unknown. The rate of ageing varies substantially across different species, and this, to a large extent, is genetically based. In model organisms and laboratory settings, researchers have demonstrated that selected alterations in specific genes can extend lifespan quite substantially in nematodes, less so in fruit flies and less again in mice. Life span extension can occur as the result of genetic alterations that increase DNA repair, reduce oxidative damage or reduce cell suicide (apoptosis) due to DNA damage.[21] Even in the relatively simple and short-lived organisms, the mechanisms of ageing remain to be elucidated. Less is known about mammalian ageing, in part due to the much longer lives in even small mammals such as the mouse (around 3 years).
A primary model organism for studying ageing is the nematode C. elegans, because of their short lifespan, the ability to easily perform genetic manipulations or knock down genes with RNA interference, and other factors.[22] Most known mutations and RNA interference targets that extend lifespan were first discovered in C. elegans.[23]
- Evolutionary theories: Many have argued that life-span, like other phenotypes, is selected.
- Telomere theory: Telomeres have experimentally been shown to shorten with each successive cell division.[24] Shortened telomeres activate a mechanism that prevents further cell multiplication.[25][26] This may be particularly limiting to tissues such as bone marrow and the arterial lining where cell division occurs repeatedly throughout life.[27] Importantly though, mice lacking telomerase enzyme do not show a dramatically reduced lifespan,[28] invalidating at least simple versions of the telomere theory of ageing. Laboratory mice may be an exception for the theory, as they have long hypervariable telomeres,[29] which prolong the period after which telomere shortening would affect life-span. However, wild mouse strains do not, and telomere length in these breeds is unrelated to lifespan[30]
- Reproductive-cell cycle theory: The idea that ageing is regulated by reproductive hormones that act in an antagonistic pleiotropic manner via cell cycle signalling, promoting growth and development early in life to achieve reproduction, but later in life, in a futile attempt to maintain reproduction, become dysregulated and drive senescence (dyosis).[1][31] The endocrine dyscrasia that follows the loss of follicles with menopause, and the loss of Leydig and Sertoli cells during andropause, drive aberrant cell cycle signaling that leads to cell death and dysfunction, tissue dysfunction (disease) and ultimately death. Moreover, the hormones that regulate reproduction also regulate cellular metabolism, explaining the increases in fat deposition during pregnancy through to the deposition of centralized adiposity with the dysregulation of the HPG axis following menopause and during andropause (Atwood and Bowen, 2006). This theory, which introduced a new definition of aging, has facilitated the conceptualization of why and how aging occurs at the evolutionary, physiological and molecular levels.[1] In essence, this theory proposes that reproductive hormones not only regulate reproduction and metabolism, but also modulate the life and function of cells, and in so doing, the life of the organism, thereby tying reproduction, metabolism and longevity together in an evolutionary manner that allows for the continued survival of the species.
- DNA damage theory of ageing: Genetic damage has two types. Mutations, are damages to the DNA sequence, while epimutations which are damages to the DNA scaffolding which regulates gene expression in the cell. Both ultimately harm our health by causing abnormal gene expressions. Some (epi-)mutations leads to cancers, which are the uncontrolled growth and division of cell. Lifelong studies of mice suggest that most mutations happen during embryonic and childhood development, when cells divide often, as each cell division is a chance for errors in DNA replication.[32] Known causes of cancer (radiation, chemical and viral) account for about 30% of the total cancer burden and for about 30% of the total DNA damage. DNA damage causes the cells to stop dividing or induce apoptosis, often affecting stem cell pools and hence hindering regeneration.[2] DNA damage is thought to be the common pathway causing both cancer and ageing. Viral infection would appear to be the most likely cause of the other 70% of DNA damage especially in cells that are not exposed to smoking and sun light. It has been argued, too, that intrinsic causes of DNA damage are more important drivers of ageing.[33][34][35]
- Gene loss theory of ageing: It has been measured that dogs lose approximately 3.3% of the DNA in their heart muscle annually while humans lose approximately 0.6% of their heart muscle DNA each year. This number is very similar to the ratio of the maximum longevities of the two species (120 years vs. 20 years, a 6/1 ratio). The comparative percentage is also similar between the dog and human for yearly DNA loss in the brain and lymphocytes. As stated by lead author, Bernard L. Strehler, "....genetic damage (particularly gene loss) is almost certainly (or probably the) central cause of aging."[36]
- Autoimmune theory: The idea that ageing results from an increase in autoantibodies that attack the body's tissues. A number of diseases associated with ageing, such as atrophic gastritis and Hashimoto's thyroiditis, are probably autoimmune in this way. While inflammation is very much evident in old mammals, even SCID mice in SPF colonies still experience senescence.
- mTOR theory: mTOR, a protein that inhibits autophagy has been linked to ageing through the insulin signalling pathway. It has been found, in various model species, that caloric restriction leads to longer lifespans, an effect that is likely mediated by the nutrient-sensing function of the mTOR pathway.[18] mTOR functions through nutrient and growth cues leading scientists to believe that dietary restriction and mTOR are related in terms of longevity. When organisms restrict their diet, mTOR activity is reduced, which allows an increased level of autophagy. This recycles old or damaged cell parts, which increases longevity and decreases the chances of being obese. This is thought to prevent spikes of glucose concentration in the blood, leading to reduced insulin signalling. This has been linked to less mTOR activation as well. Therefore, longevity has been connected to caloric restriction and insulin sensitivity inhibiting mTOR, which in turns allows autophagy to occur more frequently. It may be that mTOR inhibition and autophagy reduce the effects of reactive oxygen species on the body, which damage DNA and other organic material, so longevity would be increased.[37]

- It has been argued that ageing is programmed: that an internal clock detects a time to end investing in the organism, leading to death. This ageing-clock theory suggests, as in a clock, an ageing sequence is built into the operation of the nervous or endocrine system of the body. In rapidly dividing cells, shortening of the telomeres would provide such a clock. This idea is in contradiction with the evolutionary based theory of ageing.[38][39]
- Accumulative-waste theory: The biological theory of ageing that points to a buildup of cells of waste products that presumably interferes with metabolism. Evidence supporting this theory is the presence of a waste product called lipofuscin leading to age pigment. Lipofuscin is formed by a complex reaction that binds fat in the cells to proteins. This waste accumulates in the cells as small granules and increases in size as a person ages[40]
- Wear-and-tear theory: The very general idea that changes associated with ageing are the result of chance damage that accumulates over time.
- Error accumulation theory: The idea that ageing results from chance events that escape proof reading mechanisms, which gradually damages the genetic code.
- Cross-linkage theory: The idea that ageing results from accumulation of cross-linked compounds that interfere with normal cell function.[39][41]
- Free-radical theory: The idea that free radicals (unstable and highly reactive organic molecules), or more generally reactive oxygen species or oxidative stress create damage that gives rise to symptoms we recognise as ageing.[39][42] Michael Ristow's group has provided evidence that the effect of calorie restriction may be due to increased formation of free radicals within the mitochondria causing a secondary induction of increased antioxidant defence capacity.[43]
- Misrepair-accumulation theory: Wang et al.[44] suggest that ageing is the result of the accumulation of "misrepair". Important in this theory is to distinguish among "damage" which means a newly emerging defect BEFORE any reparation has taken place and "misrepair" which describes the remaining defective structure AFTER (incorrect) repair. The key points in this theory are:
- There is no original damage left unrepaired in a living being. If damage was left unrepaired a life-threatening condition (such as bleeding, infection, or organ failure) would develop.
- Misrepair, the repair with less accuracy, does not happen accidentally. It is a necessary measure of the reparation system to achieve sufficiently quick reparation in situations of serious or repeated damage, to maintain the integrity and basic function of a structure, which is important for the survival of the living being.
- Hence the appearance of misrepair increases the chance for the survival of individual, by which the individual can live at least up to the reproduction age, which is critically important for the survival of species. Therefore the misrepair mechanism was selected by nature due to its evolutionary advantage.
- However, since misrepair as a defective structure is invisible for the reparation system, it accumulates with time and causes gradually the disorganisation of a structure (tissue, cell, or molecule); this is the actual source of ageing.
- Ageing hence is the side-effect for survival, but important for species survival. Thus misrepair might represent the mechanism by which organisms are not programmed to die but to survive (as long as possible) and ageing is just the price to be paid.
- Reliability theory of ageing and longevity: A general theory about systems failure. It allows researchers to predict the age-related failure kinetics for a system of given architecture (reliability structure) and given reliability of its components. Reliability theory predicts that even those systems that are entirely composed of non-ageing elements (with a constant failure rate) will nevertheless deteriorate (fail more often) with age, if these systems are redundant in irreplaceable elements. Ageing, therefore, is a direct consequence of systems redundancy. Reliability theory also predicts the late-life mortality deceleration with subsequent levelling-off, as well as the late-life mortality plateaus, as an inevitable consequence of redundancy exhaustion at extreme old ages. The theory explains why mortality rates increase exponentially with age (the Gompertz law) in many species, by taking into account the initial flaws (defects) in newly formed systems. It also explains why organisms "prefer" to die according to the Gompertz law, while technical devices usually fail according to the Weibull (power) law. Reliability theory allows to specify conditions when organisms die according to the Weibull distribution: organisms should be relatively free of initial flaws and defects. The theory makes it possible to find a general failure law applicable to all adult and extreme old ages, where the Gompertz and the Weibull laws are just special cases of this more general failure law. The theory explains why relative differences in mortality rates of compared populations (within a given species) vanish with age (compensation law of mortality), and mortality convergence is observed due to the exhaustion of initial differences in redundancy levels.
Some aspects of bacterial senescence may lend support to contemporary theories of ageing, including the free radical, antagonistic pleiotropy, and disposable soma theories.[45]
Effects of ageing

Age is a major risk factor for most common neurodegenerative diseases, including Mild cognitive impairment, Alzheimer's disease, cerebrovascular disease, Parkinson's disease and Lou Gehrig's disease. Steady decline in many cognitive processes is seen across the lifespan, accelerating from the twenties or even thirties.[46] Research has focused in particular on memory and ageing and has found decline in many types of memory with ageing, but not in semantic memory or general knowledge such as vocabulary definitions, which typically increases or remains steady until the late adulthood.[47] Early studies on changes in cognition with age generally found declines in intelligence in the elderly, but studies were cross-sectional rather than longitudinal and thus results may be an artefact of cohort rather than a true example of decline. However, longitudinal studies could be confounded due to prior test experience.[48] Intelligence may decline with age, though the rate may vary depending on the type and may in fact remain steady throughout most of the lifespan, dropping suddenly only as people near the end of their lives. Individual variations in rate of cognitive decline may therefore be explained in terms of people having different lengths of life.[49] There are changes to the brain: though neuron loss is minor after 20 years of age there is a 10% reduction each decade in the total length of the brain's myelinated axons.[50]
Age can result in communication barriers, such as due to hearing loss and visual impairment.[51] Sensory impairments include hearing and vision deficits. Changes in cognition, hearing, and vision are associated with healthy ageing and can cause problems when diagnosing dementia and aphasia due to the similarities.[52] Common conditions that can increase the risk of hearing loss in elderly people are high blood pressure, diabetes or the use of certain medications harmful to the ear.[53] Hearing aids are commonly referred to as personal amplifying systems, which can generally improve hearing by about 50%. In visual impairment, non-verbal communication is reduced, which can lead to isolation and possible depression. Macular degeneration is a common cause of vision loss in elderly people. This degeneration is caused by systemic changes in the circulation of waste products and growth of abnormal vessels around the retina causing the photoreceptors not to receive proper images.[54]
The term "ageing" is somewhat ambiguous. Distinctions may be made between "universal ageing" (age changes that all people share) and "probabilistic ageing" (age changes that may happen to some, but not all people as they grow older including age-related diseases). Chronological ageing may also be distinguished from "social ageing" (cultural age-expectations of how people should act as they grow older) and "biological ageing" (an organism's physical state as it ages).[55] There is also a distinction between "proximal ageing" (age-based effects that come about because of factors in the recent past) and "distal ageing" (age-based differences that can be traced back to a cause early in person's life, such as childhood poliomyelitis).[49] Chronological age does not correlate perfectly with functional age, i.e. two people may be of the same age, but differ in their mental and physical capacities.
The evolution of ageing
Because evolution is the unifying theory of biology, understanding how evolution works is essential for explaining why we age. Ageing evolves because of the interaction of two effects. First, natural selection is stronger on the young than on the old; this explains why the autosomal dominant disease, Huntington's disease, can persist even though it is inexorably lethal. Second, any genetic, developmental, or physiological effect that increases the reproductive performance of the young will evolve so long as the costs that it imposes on the old are not too great.[56] Or put another way, traits that benefit early survival and reproduction will be selected for even if they contribute to an earlier death. Such genetic effects are called antagonistic pleiotropy. "Antagonistic" refers to the impact on fitness in the young, which is positive and the negative effect on the old. Genetic pleiotropy refers to genes that have multiple effects. Antagonistic pleiotropy has been identified both in model organisms and in humans.[57] In humans, some of the genetic variants that increase fertility in the young are now known to increase cancer risk in the old. Such genes include p53[58] and BRCA1.[59]
The biological mechanisms which regulate lifespan evolved several hundred million years ago.[23]
Society and culture

Different cultures express age in different ways. The age of an adult human is commonly measured in whole years since the day of birth. Arbitrary divisions set to mark periods of life may include: juvenile (via infancy, childhood, preadolescence, adolescence), early adulthood, middle adulthood, and late adulthood. More casual terms may include "teenagers," "tweens," "twentysomething", "thirtysomething", etc. as well as "vicenarian", "tricenarian", "quadragenarian", etc.
Most legal systems define a specific age for when an individual is allowed or obliged to do particular activities. These age specifications include voting age, drinking age, age of consent, age of majority, age of criminal responsibility, marriageable age, age of candidacy, and mandatory retirement age. Admission to a movie for instance, may depend on age according to a motion picture rating system. A bus fare might be discounted for the young or old. Each nation, government and non-governmental organisation has different ways of classifying age.
Economics
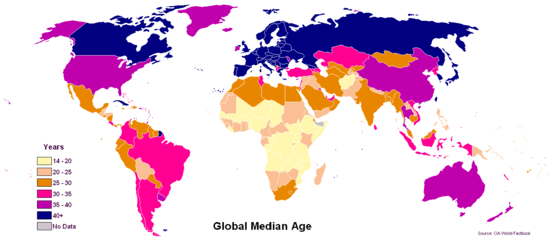
As life expectancy rises and birth rates decline in developed countries, the median age itself rises accordingly. According to the United Nations, this process is taking place in nearly every country in the world.[60] A rising median age can have significant social and economic implications, as the workforce gets progressively older and the number of old workers and retirees grows relative to the number of young workers. Older people generally incur more health-related costs than do younger people in the workplace and can also cost more in worker's compensation and pension liabilities.[61] In most developed countries an older workforce is somewhat inevitable. In the United States for instance, the Bureau of Labor Statistics estimates that one in four American workers will be 55 or older by 2020.[61]
Sociology
In the field of sociology and mental health, aging is seen in five different views: aging as maturity, aging as decline, aging as a life-cycle event, aging as generation, and aging as survival.[62] Positive correlates with aging often include economics, employment, marriage, children, education, and sense of control, as well as many others.
Health care demand
Many societies in Western Europe and Japan have ageing populations. While the effects on society are complex, there is a concern about the impact on health care demand. The large number of suggestions in the literature for specific interventions to cope with the expected increase in demand for long-term care in ageing societies can be organised under four headings: improve system performance; redesign service delivery; support informal caregivers; and shift demographic parameters.[63]
However, the annual growth in national health spending is not mainly due to increasing demand from ageing populations, but rather has been driven by rising incomes, costly new medical technology, a shortage of health care workers and informational asymmetries between providers and patients.[64] A number of health problems become more prevalent as people get older. These include mental health problems as well as physical health problems, especially dementia.
It has been estimated that population ageing only explains 0.2 percentage points of the annual growth rate in medical spending of 4.3 percent since 1970. In addition, certain reforms to the Medicare system in the United States decreased elderly spending on home health care by 12.5 percent per year between 1996 and 2000.[65]
Perceptions of ageing
Positive self-perception of health has been correlated with higher well-being and reduced mortality in the elderly.[66][67] Various reasons have been proposed for this association; people who are objectively healthy may naturally rate their health better than that of their ill counterparts, though this link has been observed even in studies which have controlled for socioeconomic status, psychological functioning and health status.[68] This finding is generally stronger for men than women,[67] though this relationship is not universal across all studies and may only be true in some circumstances.[68]
As people age, subjective health remains relatively stable, even though objective health worsens.[69] In fact, perceived health improves with age when objective health is controlled in the equation.[70] This phenomenon is known as the "paradox of ageing." This may be a result of social comparison;[71] for instance, the older people get, the more they may consider themselves in better health than their same-aged peers.[72] Elderly people often associate their functional and physical decline with the normal ageing process.[73][74]
Successful ageing
The concept of successful ageing can be traced back to the 1950s and was popularised in the 1980s. Previous research into ageing exaggerated the extent to which health disabilities, such as diabetes or osteoporosis, could be attributed exclusively to age, and research in gerontology exaggerated the homogeneity of samples of elderly people.[75][76] Other research shows that even late in life, potential exists for physical, mental, and social growth and development.[77]
Traditional definitions of successful aging have emphasized absence of physical and cognitive disabilities.[78] In their 1987 article, Rowe and Kahn characterized successful aging as involving three components: a) freedom from disease and disability, b) high cognitive and physical functioning, and c) social and productive engagement.[76]
Other
The social science of aging includes disengagement theory, activity theory, selectivity theory, and continuity theory.
Retirement, a common transition faced by the elderly, may have both positive and negative consequences.[79]
Prevention and reversal

Since ageing is a cause or major risk factor of the age related diseases and many other causes of mortality, there are growing efforts in ageing research to slow ageing and extend healthy lifespan.[80][81] [82] There are several prizes for extending lifespan and slowing ageing in mammals such as Mprize of Methuselah Foundation, Palo Alto Longevity Prize,[83] and others. Several companies and organisations, such as Google Calico, Human Longevity, Craig Venter, Quantum Pharmaceuticals,[84] SENS Research Foundation, and Science for Life Extension in Russia,[85] declared stopping or delaying ageing as their goal.
Many scientists who study the biology of ageing believe that the development of interventions which slow ageing is inevitable.[37] Several drugs and food supplements have been shown to retard or reverse the biological effects of ageing in animal models, but none has yet been proven to do so in humans.
There are three main signalling pathways which influence the rate of ageing: caloric restriction, the insulin/IGF-1-like signalling pathway, and the activity levels of the electron transport chain.[8]
The US National Institute on Aging currently funds an intervention testing program, whereby investigators nominate compounds (based on specific molecular ageing theories) to have evaluated with respect to their effects on lifespan and age-related biomarkers in outbred mice.[86] Previous age-related testing in mammals has proved largely irreproducible, because of small numbers of animals and lax mouse husbandry conditions. The intervention testing program aims to address this by conducting parallel experiments at three internationally recognised mouse ageing-centres, the Barshop Institute at UTHSCSA, the University of Michigan at Ann Arbor and the Jackson Laboratory.
Ronald A. DePinho, a cancer geneticist at the Dana-Farber Cancer Institute and Harvard Medical School, published a paper in Nature magazine in November 2010 which indicated that the organs of genetically altered mice, designed to activate telomerase after feeding them with a chemical, were rejuvenated. Shrivelled testes grew back to normal and the animals regained their fertility. Other organs, such as the spleen, liver, intestines and brain, recuperated from their degenerated state. In this experiment mice were engineered to not produce telomerase naturally but after a chemical "switch" the system would then restore telomerase. Importantly, this chemical does not have the ability to produce telomerase in animals that are not genetically altered. Moreover, telomerase activation is also associated with the growth of cancerous tumours which could prevent anti-ageing treatments using this discovery.[87]
mTOR inhibition and the frequent activation of autophagy has been shown to increase longevity in model organisms such as yeast, flies and mice. mTor inhibition and autophagy have also been linked to insulin sensitivity and the reduction of reactive oxygen species (ROS) damage, which is another major proposed cause to ageing. It has become clear that autophagy activation in the body by mTOR inhibition increases longevity. mTOR inhibition reduces ROS damage by activating autophagy, which will recycle the damaged parts of cells and re use them for functioning parts. This process reduces ROS damage to a reasonable amount, therefore increasing longevity. mTOR inhibition has also been linked to other major ageing diseases. mTOR inhibition has helped treat neurodegenerative diseases like Alzheimer’s in mice. It has also been used to reduce tumor growth in several cancers including renal, breast and several other rare cancers. Finally mTOR inhibition is also linked to reducing obesity and increasing immune function. The mTOR inhibition reduces the likelihood of diet induced and age induced obesity in mice, but in some cases led to glucose intolerance. Caloric restriction and exercise are two ways to activate autophagy and inhibit mTOR which can help resolve all of these common age related health issues.[37]
The cellular balance between energy generation and consumption (energy homeostasis) requires tight regulation during ageing. In 2011, it was demonstrated that acetylation levels of AMP-activated protein kinase change with age in yeast and that preventing this change slows yeast ageing.[88]
Caloric restriction substantially affects lifespan in many animals, including the ability to delay or prevent many age-related diseases.[15] Evidence in both animals and humans suggests that resveratrol may be a caloric restriction mimetic.[19]
Most known genetic interventions in C. elegans increase lifespan by 1.5 to 2.5-fold. As of 2009, the record for lifespan extension in C. elegans is a single-gene mutation which increases adult survival by tenfold.[23] The strong conservation of some of the mechanisms of ageing discovered in model organisms imply that they may be useful in the enhancement of human survival. However, the benefits may not be proportional; longevity gains are typically greater in C. elegans than fruit flies, and greater in fruit flies than in mammals. One explanation for this is that mammals, being much longer-lived, already have many traits which promote lifespan. However, there are still opportunities for healthy human life to be extended beyond its current levels by pharmacological interventions.[23]
Recently, the $1 Million Palo Alto Longevity Prize was launched. It is a research incentive prize to encourage teams from all over the world to compete in an all-out effort to “hack the code” that regulates our health and lifespan. It was founded by Joon Yun.[83][89][90][91][92]
See also
- Aging brain
- Aging movement control
- Aging of Europe
- Anti-aging movement
- Biodemography
- Biodemography of human longevity
- Biological clock
- Biological immortality
- Biomarkers of aging
- Clinical Geropsychology
- Death
- DNA repair-deficiency disorder
- Endocrinology of reproduction
- Frailty syndrome
- Genetics of aging
- Gerontology
- Life expectancy
- List of life extension-related topics
- Longevity
- Memory and aging
- Old age
- Old man smell
- Population aging
- Progeria
- Retirement
- Senescence
- Software aging
- Stem cell theory of aging
- Supercentenarian
- Transgenerational design
References
- ↑ 1.0 1.1 1.2 Bowen, Richard L.; Atwood, Craig S. (2004). "Living and Dying for Sex". Gerontology 50 (5): 265–90. doi:10.1159/000079125. PMID 15331856.
- ↑ 2.0 2.1 2.2 Birbrair, A.; Zhang, T.; Wang, Z.-M.; Messi, M. L.; Mintz, A.; Delbono, O. (2013). "Type-1 pericytes participate in fibrous tissue deposition in aged skeletal muscle". AJP: Cell Physiology 305 (11): C1098. doi:10.1152/ajpcell.00171.2013.
- ↑ 3.0 3.1 Dillin A, Gottschling DE, Nyström T; Gottschling; Nyström (2014). "The good and the bad of being connected: the integrons of aging". Curr Opin Cell Biol 26: 107–12. doi:10.1016/j.ceb.2013.12.003. PMC 3927154. PMID 24529252.
- ↑ 4.0 4.1 4.2 De Grey, Aubrey D.N.J (2007). "Life Span Extension Research and Public Debate: Societal Considerations". Studies in Ethics, Law, and Technology 1. doi:10.2202/1941-6008.1011.
- ↑ Vincent, John A. (2005). "Understanding generations: Political economy and culture in an ageing society". The British Journal of Sociology 56 (4): 579–99. doi:10.1111/j.1468-4446.2005.00084.x. PMID 16309437.
- ↑ Lopez, Alan D; Mathers, Colin D; Ezzati, Majid; Jamison, Dean T; Murray, Christopher JL (2006). "Global and regional burden of disease and risk factors, 2001: Systematic analysis of population health data". The Lancet 367 (9524): 1747–57. doi:10.1016/S0140-6736(06)68770-9. PMID 16731270.
- ↑ Brunet Lab: Molecular Mechanisms of Longevity and Age Related Diseases. Stanford.edu. Retrieved on 11 April 2012.
- ↑ 8.0 8.1 8.2 Taylor RC, Dillin A (2011). "Aging as an event of proteostasis collapse.". Cold Spring Harb Perspect Biol 3 (5): a004440. doi:10.1101/cshperspect.a004440. PMC 3101847. PMID 21441594.
- ↑ Bartke A (2011). "Single-gene mutations and healthy ageing in mammals.". Philos Trans R Soc Lond B Biol Sci 366 (1561): 28–34. doi:10.1098/rstb.2010.0281. PMC 3001310. PMID 21115527.
- ↑ Timiras, Paola S. (2003) Physiological Basis of Ageing and Geriatrics. Informa Health Care. ISBN 0-8493-0948-4. p. 26.
- ↑ Silverman, Jacob. "Is there a 400 pound lobster out there?". howstuffworks.
- ↑ Wallace, David Foster (2005). Consider the Lobster and Other Essays. Little, Brown & Company. ISBN 0-316-15611-6.
- ↑ Dedeepiya, Vidyasagar Devaprasad; Rao, Yegneswara Yellury; Jayakrishnan, Gosalakkal A.; Parthiban, Jutty K. B. C.; Baskar, Subramani; Manjunath, Sadananda Rao; Senthilkumar, Rajappa; Abraham, Samuel J. K. (2012). "Index of CD34+ Cells and Mononuclear Cells in the Bone Marrow of Spinal Cord Injury Patients of Different Age Groups: A Comparative Analysis". Bone Marrow Research 2012: 1–8. doi:10.1155/2012/787414. PMC 3398573. PMID 22830032.
- ↑ J Sun; Kale, SP; Childress, AM; Pinswasdi, C; Jazwinski, SM (15 July 1994). "Divergent roles of RAS1 and RAS2 in yeast longevity". Journal of Biological Chemistry 269 (28): 18638–45. PMID 8034612.
- ↑ 15.0 15.1 15.2 15.3 15.4 Guarente L, Picard F; Picard (2005). "Calorie restriction—the SIR2 connection". Cell 120 (4): 473–82. doi:10.1016/j.cell.2005.01.029. PMID 15734680.
- ↑ Agarwal B, Baur JA; Baur (2011). "Resveratrol and life extension". Ann N Y Acad Sci 1215 (1): 138–43. Bibcode:2011NYASA1215..138A. doi:10.1111/j.1749-6632.2010.05850.x. PMID 21261652.
- ↑ 17.0 17.1 Kemnitz JW (2011). "Calorie restriction and aging in nonhuman primates.". ILAR J 52 (1): 66–77. doi:10.1093/ilar.52.1.66. PMC 3278796. PMID 21411859.
- ↑ 18.0 18.1 18.2 Fontana L, Partridge L, Longo VD; Partridge; Longo (2010). "Extending healthy life span—from yeast to humans". Science 328 (5976): 321–6. Bibcode:2010Sci...328..321F. doi:10.1126/science.1172539. PMC 3607354. PMID 20395504.
- ↑ 19.0 19.1 Lam YY, Peterson CM, Ravussin E; Peterson; Ravussin (2013). "Resveratrol vs. calorie restriction: data from rodents to humans". Exp Gerontol 48 (10): 1018–24. doi:10.1016/j.exger.2013.04.005. PMID 23624181.
- ↑ Hayflick, Leonard. (1994). How and why we age. New York: Ballantine Books. p. 261. ISBN 978-0-345-33918-8. OCLC 29908633.
- ↑ Bernstein C, Bernstein H. (2004) Aging and Sex, DNA Repair in. See page 58. Encyclopedia of Molecular Cell Biology and Molecular Medicine, 2nd edition. Robert A. Meyers (Editor) pages 55–98. Wiley-VCH. ISBN 3-527-30543-2 ISBN 978-3-527-30543-8
- ↑ Deepti S. Wilkinson; Rebecca C. Taylor; Andrew Dillin (2012). "Analysis of Aging in Caenorhabditis elegans". In Joel H. Rothman and Andrew Singson. Caenorhabditis Elegans: Cell Biology and Physiology. Academic Press. pp. 353–381. ISBN 978-0-12-394620-1.
- ↑ 23.0 23.1 23.2 23.3 Shmookler Reis RJ, Bharill P, Tazearslan C, Ayyadevara S; Bharill; Tazearslan; Ayyadevara (2009). "Extreme-longevity mutations orchestrate silencing of multiple signaling pathways". Biochim Biophys Acta 1790 (10): 1075–83. doi:10.1016/j.bbagen.2009.05.011. PMC 2885961. PMID 19465083.
- ↑ Stibich, Mark (19 April 2009) Telomere Shortening – The Secret to Aging?. About.com
- ↑ m. Mikhelson, Victor; Gamaley, Irina (2013). "Telomere Shortening is a Sole Mechanism of Aging in Mammals". Current Aging Science 5 (3): 203–8. doi:10.2174/1874609811205030006. PMID 23387887.
- ↑ "Mitochondrial Theory of Aging and Other Aging Theories". 1Vigor. Retrieved 4 October 2013.
- ↑ Minamino, Tohru; Komuro, I (2008). "Role of telomeres in vascular senescence". Frontiers in Bioscience 13 (13): 2971–9. doi:10.2741/2902. PMID 17981770.
- ↑ Blasco, María A; Lee, Han-Woong; Hande, M.Prakash; Samper, Enrique; Lansdorp, Peter M; Depinho, Ronald A; Greider, Carol W (1997). "Telomere Shortening and Tumor Formation by Mouse Cells Lacking Telomerase RNA". Cell 91 (1): 25–34. doi:10.1016/S0092-8674(01)80006-4. PMID 9335332.
- ↑ Kipling, David; Cooke, Howard J. (1990). "Hypervariable ultra-long telomeres in mice". Nature 347 (6291): 400–2. Bibcode:1990Natur.347..400K. doi:10.1038/347400a0. PMID 2170845.
- ↑ Hemann, M. T.; Greider, CW (2000). "Wild-derived inbred mouse strains have short telomeres". Nucleic Acids Research 28 (22): 4474–8. doi:10.1093/nar/28.22.4474. PMC 113886. PMID 11071935.
- ↑ Atwood, Craig S.; Bowen, Richard L. (2011). "The reproductive-cell cycle theory of aging: An update". Experimental Gerontology 46 (2–3): 100–7. doi:10.1016/j.exger.2010.09.007. PMID 20851172.
- ↑ L. Robert, J. Labat-Robert, A. M. Robert (2010). "Genetic, epigenetic and posttranslational mechanisms of aging". Biogerontology 11 (4): 387–399. doi:10.1007/s10522-010-9262-y. PMID 20157779.
- ↑ Gensler, Helen L.; Bernstein, Harris (1981). "DNA Damage as the Primary Cause of Aging". The Quarterly Review of Biology 56 (3): 279–303. doi:10.1086/412317. JSTOR 2826464. PMID 7031747.
- ↑ Sinha, Jitendra Kumar; Ghosh, Shampa; Swain, Umakanta; Giridharan, Nappan Veethil; Raghunath, Manchala (2014). "Increased macromolecular damage due to oxidative stress in the neocortex and hippocampus of WNIN/Ob, a novel rat model of premature aging". Neuroscience 269: 256–64. doi:10.1016/j.neuroscience.2014.03.040. PMID 24709042.
- ↑ Freitas, Alex A.; De Magalhães, João Pedro (2011). "A review and appraisal of the DNA damage theory of ageing". Mutation Research/Reviews in Mutation Research 728 (1–2): 12–22. doi:10.1016/j.mrrev.2011.05.001. PMID 21600302.
- ↑ Strehler, Bernard L. (1986). "Genetic instability as the primary cause of human aging". Experimental Gerontology 21 (4–5): 283–319. doi:10.1016/0531-5565(86)90038-0. PMID 3545872.
- ↑ 37.0 37.1 37.2 Johnson, Simon C.; Rabinovitch, Peter S.; Kaeberlein, Matt (2013). "MTOR is a key modulator of ageing and age-related disease". Nature 493 (7432): 338–45. Bibcode:2013Natur.493..338J. doi:10.1038/nature11861. PMC 3687363. PMID 23325216.
- ↑ Hayflick, L. (1987) Origins of longevity. In Warner, H.R., Butler, R.N., Sprott, R.L. and Schneider, E.L. (eds), Modern Biological Theories of Aging. Raven Press, New York, pp. 21–34. ISBN 0-88167-310-2 PMC 2995895
- ↑ 39.0 39.1 39.2 Bernstein C, Bernstein H. (1991) Aging, Sex, and DNA Repair. Academic Press, San Diego. ISBN 0-12-092860-4. pp. 314, 320 and 326
- ↑ Gavrilov, L. A.; Gavrilova, N. S. (2006), Reliability Theory of Aging and Longevity. In-Handbook of the Biology of Aging, ed. Masoro E. J. and Austad S. N, Academic Press, San Diego, CA, pp. 3-42.
- ↑ Bjorksten, Johan; Tenhu, Heikki (1990). "The crosslinking theory of aging — Added evidence". Experimental Gerontology 25 (2): 91–5. doi:10.1016/0531-5565(90)90039-5. PMID 2115005.
- ↑ Harman, D. (1981). "The aging process". Proceedings of the National Academy of Sciences 78 (11): 7124–8. Bibcode:1981PNAS...78.7124H. doi:10.1073/pnas.78.11.7124. PMC 349208. PMID 6947277.
- ↑ Schulz, Tim J.; Zarse, Kim; Voigt, Anja; Urban, Nadine; Birringer, Marc; Ristow, Michael (2007). "Glucose Restriction Extends Caenorhabditis elegans Life Span by Inducing Mitochondrial Respiration and Increasing Oxidative Stress". Cell Metabolism 6 (4): 280–93. doi:10.1016/j.cmet.2007.08.011. PMID 17908557.
- ↑ Wang, Jicun; Michelitsch, Thomas; Wunderlin, Arne; Mahadeva, Ravi (2009). "Aging as a consequence of misrepair – a novel theory of aging" 0904. p. 575. arXiv:0904.0575. Bibcode:2009arXiv0904.0575W.
- ↑ Nyström, T. (2003). "The free-radical hypothesis of aging goes prokaryotic". Cellular and Molecular Life Sciences (CMLS) 60 (7): 1333–41. doi:10.1007/s00018-003-2310-X. PMID 12943222.
- ↑ Salthouse, Timothy A. (2009). "When does age-related cognitive decline begin?". Neurobiology of Aging 30 (4): 507–14. doi:10.1016/j.neurobiolaging.2008.09.023. PMC 2683339. PMID 19231028.
- ↑ Schaie, K. Warner (2005). Developmental Influences on Adult Intelligence. doi:10.1093/acprof:oso/9780195156737.001.0001. ISBN 978-0-19-515673-7.
- ↑ Desjardins, Richard; Warnke, Arne Jonas (2012). "Ageing and Skills". OECD Education Working Papers. doi:10.1787/5k9csvw87ckh-en.
- ↑ 49.0 49.1 Stuart-Hamilton, Ian (2006). The Psychology of Ageing: An Introduction. London: Jessica Kingsley Publishers. ISBN 1-84310-426-1.
- ↑ Marner, Lisbeth; Nyengaard, Jens R.; Tang, Yong; Pakkenberg, Bente (2003). "Marked loss of myelinated nerve fibers in the human brain with age". The Journal of Comparative Neurology 462 (2): 144–52. doi:10.1002/cne.10714. PMID 12794739.
- ↑ Worrall, L.,& Hickson, L. M. (2003). "Theoretical foundations of communication disability in aging", pp. 32–33 in Linda E. Worrall & Louise M. Hickson(Eds.). Communication disability in aging: from prevention to intervention. Clifton Park, NY: Delmar Learning
- ↑ Worrall, L. and Hickson, L. M. (2003). "Implications for theory, practice, and policy", pp. 297–298 in Linda E. Worrall & Louise M. Hickson (Eds.). Communication disability in aging: from prevention to intervention. Clifton Park, NY: Delmar Learning
- ↑ Worrall, L.,& Hickson, L. M. (2003). "Communication activity limitations", pp. 141–142 in Linda E. Worrall & Louise M. Hickson (Eds.). Communication disability in aging: from prevention to intervention. Clifton Park, NY: Delmar Learning
- ↑ Nussbaum, J. F., Thompson, T. L., & Robinson, J. D. (1989). "Barriers to conversation", pp. 234–253 in Jon F. Nussbaum, Teresa Thompson, James D. Robinson (Eds.). Communication and aging. New York: Harper & Row
- ↑ Phillips, Judith, Kristine Ajrouch, and Sarah Hillcoat-Nallétamby (2010) Key Concepts in Social Gerontology. SAGE Publications.ISBN 9781446204283. pp. 12–13.
- ↑ Williams, George C. (1957). "Pleiotropy, Natural Selection, and the Evolution of Senescence". Evolution 11 (4): 398–411. doi:10.2307/2406060. JSTOR 2406060.
- ↑ Kirkwood, T. B. L.; Rose, M. R. (1991). "Evolution of Senescence: Late Survival Sacrificed for Reproduction". Philosophical Transactions of the Royal Society B: Biological Sciences 332 (1262): 15–24. doi:10.1098/rstb.1991.0028. PMID 1677205.
- ↑ Kang, H.-J.; Feng, Z.; Sun, Y.; Atwal, G.; Murphy, M. E.; Rebbeck, T. R.; Rosenwaks, Z.; Levine, A. J.; Hu, W. (2009). "Single-nucleotide polymorphisms in the p53 pathway regulate fertility in humans". Proceedings of the National Academy of Sciences 106 (24): 9761–6. doi:10.1073/pnas.0904280106. PMC 2700980. PMID 19470478.
- ↑ Smith, K. R.; Hanson, H. A.; Mineau, G. P.; Buys, S. S. (2011). "Effects of BRCA1 and BRCA2 mutations on female fertility". Proceedings of the Royal Society B: Biological Sciences 279 (1732): 1389–95. doi:10.1098/rspb.2011.1697. PMC 3282366. PMID 21993507.
- ↑ "UN Human Development Report 2005" (PDF). United Nations Development Programme. Archived from the original (PDF) on 27 May 2008. Retrieved 7 October 2010.
- ↑ 61.0 61.1 Chosewood, L. Casey. "Safer and Healthier at Any Age: Strategies for an Aging Workforce". NIOSH Science Blog. National Institute for Occupational Safety and Health. Retrieved 6 August 2012.
- ↑ Scheid, Teresa L.; Brown, Tony N. (2010). A Handbook for the Study of Mental Health (Second ed.). New York: Cambridge University Press.
- ↑ Chawla, Mukesh; Dubois, Hans F. W.; Chawla, Richard B. (2006). "The Impact of Aging on Long-Term Care in Europe and Some Potential Policy Responses". International Journal of Health Services 36 (4): 719–46. doi:10.2190/AUL1-4LAM-4VNB-3YH0. PMID 17175843.
- ↑ Reinhardt, U. E. (2003). "Does the Aging of the Population Really Drive the Demand for Health Care?". Health Affairs 22 (6): 27–39. doi:10.1377/hlthaff.22.6.27. PMID 14649430.
- ↑ Meara, E.; White, C.; Cutler, D. M. (2004). "Trends in Medical Spending by Age, 1963–2000". Health Affairs 23 (4): 176–83. doi:10.1377/hlthaff.23.4.176. PMID 15318578.
- ↑ Idler, E. L. (2003). "Discussion: Gender Differences in Self-Rated Health, in Mortality, and in the Relationship Between the Two". The Gerontologist 43 (3): 372–375. doi:10.1093/geront/43.3.372.
- ↑ 67.0 67.1 Deeg, D. J. H.; Bath, P. A. (2003). "Self-Rated Health, Gender, and Mortality in Older Persons: Introduction to a Special Section". The Gerontologist 43 (3): 369–71. doi:10.1093/geront/43.3.369. PMID 12810900.
- ↑ 68.0 68.1 Benyamini, Y.; Blumstein, T.; Lusky, A.; Modan, B. (2003). "Gender Differences in the Self-Rated Health-Mortality Association: Is It Poor Self-Rated Health That Predicts Mortality or Excellent Self-Rated Health That Predicts Survival?". The Gerontologist 43 (3): 396–405; discussion 372–5. doi:10.1093/geront/43.3.396. PMID 12810904.
- ↑ Kunzmann, Ute; Little, Todd D; Smith, Jacqui (2000). "Is age-related stability of subjective well-being a paradox? Cross-sectional and longitudional evidence from the Berlin Aging Study.". Psychology and Aging 15 (3): 511–526. doi:10.1037/0882-7974.15.3.511.
- ↑ Jylhä, Marja; Guralnik, Jack M; Balfour, Jennifer; Fried, Linda P (2001). "Walking Difficulty, Walking Speed, and Age as Predictors of Self-Rated Health: The Women’s Health and Aging Study". Journal of Gerontology 56A (10): 609. PMID 11584033.
- ↑ Heckhausen, Jutta (1999). Developmental Regulation in Adulthood: Age-Normative and Sociostructural Constraints as Adaptive Challenges. Cambridge University Press. ISBN 9780521027137.
- ↑ Sargent-Cox, Kerry; Anstey, Kaarin; Luszcz, Mary (2008). "Determinants of Self-Rated Health Items With Different Points of Reference". Journal of Aging and Health 20 (6): 739–761. doi:10.1177/0898264308321035.
- ↑ Idler, Ellen L (1993). "Age differences in self-assessments of health: Age changes, cohort difference, or survivorship?". Journal of Gerontology 48 (6): S289. doi:10.1093/geronj/48.6.s289.
- ↑ Williamson, JD; Fried, LP (1996). "Characterization of older adults who attribute functional decrements to "old age"". Journal of the American Geriatrics Society 44 (12): 1429.
- ↑ Strawbridge, W. J.; Wallhagen, M. I.; Cohen, R. D. (2002). "Successful Aging and Well-Being: Self-Rated Compared with Rowe and Kahn". The Gerontologist 42 (6): 727–33. doi:10.1093/geront/42.6.727. PMID 12451153.
- ↑ 76.0 76.1 Rowe, J.; Kahn, R. (1987). "Human aging: Usual and successful". Science 237 (4811): 143–9. doi:10.1126/science.3299702. PMID 3299702.
- ↑ Papalia, Diane. "Physical and Cognitive Development in Late Adulthood". Human Development. Mc-Graw Hill.
- ↑ Baltes, Paul B.; Baltes, Margret M. (1990). "Psychological perspectives on successful aging: The model of selective optimization with compensation". In Baltes, Paul B.; Baltes, Margret M. Successful Aging. pp. 1–34. doi:10.1017/CBO9780511665684.003. ISBN 978-0-511-66568-4.
- ↑ Panek, Paul E.; Hayslip, Bert (1989). Adult development and aging. San Francisco: Harper & Row. ISBN 0-06-045012-6.
- ↑ Blagosklonny, M. V. (2009). "Validation of anti-aging drugs by treating age-related diseases". Aging 1 (3): 281–8. PMC 2806014. PMID 20157517.
- ↑ Kogan,Valeria et al. (August 2014) "Stability analysis of a model gene network links aging, stress resistance, and negligible senescence". arxiv.org.
- ↑ "Scientists' Open Letter on Aging". imminst.org.
- ↑ 83.0 83.1 "FAQ – Palo Alto Longevity Prize". Palo Alto Longevity Prize. Retrieved October 1, 2014.
- ↑ "Ageing". Quantum Pharmaceuticals. Retrieved 2015-02-04.
- ↑ Science against aging foundation "Science for Life Extension". Retrieved 2015-02-03.
- ↑ Miller, Richard A.; Harrison, David E.; Astle, Clinton M.; Floyd, Robert A.; Flurkey, Kevin; Hensley, Kenneth L.; Javors, Martin A.; Leeuwenburgh, Christiaan; Nelson, James F.; Ongini, Ennio; Nadon, Nancy L.; Warner, Huber R.; Strong, Randy (2007). "An aging Interventions Testing Program: Study design and interim report". Aging Cell 6 (4): 565–75. doi:10.1111/j.1474-9726.2007.00311.x. PMID 17578509.
- ↑ Callaway, Ewen (2010). "Telomerase reverses ageing process". Nature. doi:10.1038/news.2010.635.
- ↑ Mair W, Steffen KK, Dillin A; Steffen; Dillin (2011). "SIP-ing the elixir of youth". Cell 146 (6): 859–60. doi:10.1016/j.cell.2011.08.026. PMID 21925309.
- ↑ Ashlee Vance (September 9, 2014). "Silicon Valley Investor Backs $1 Million Prize to End Death". Bloomberg Businessweek. Retrieved October 1, 2014.
- ↑ "$1 Million Longevity Prize Seeks To "Hack The Aging Code"" (Press release). Yahoo! Finance. September 9, 2014. Retrieved October 1, 2014.
- ↑ Aaron Kinney (September 14, 2014). "Silicon Valley launches another bid to 'hack' aging, cheat death". San Jose Mercury News. Retrieved October 1, 2014.
- ↑ Victoria Thorp (November 23, 2014). "The Palo Alto Prize: A ‘Moonshot’ at Increasing Longevity". Palo Alto Pulse. Retrieved December 8, 2014.
External links
| Wikiquote has quotations related to: Ageing |
- Global AgeWatch Statistics on population ageing and life expectancy
- HelpAge International and UNFPA (2012). Ageing in the 21st Century – A Celebration and A Challenge.
-
 The dictionary definition of ageing at Wiktionary
The dictionary definition of ageing at Wiktionary -
 Media related to Ageing at Wikimedia Commons
Media related to Ageing at Wikimedia Commons
| ||||||||||||||||||||||||||