Actinomyces naeslundii
| Actinomyces naeslundii | |
|---|---|
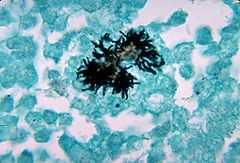 | |
| Histopathological changes due to A. naeslundii. | |
| Scientific classification | |
| Kingdom: | Bacteria |
| Phylum: | Actinobacteria |
| Order: | Actinomycetales |
| Family: | Actinomycetaceae |
| Genus: | Actinomyces |
| Species: | A. naeslundii |
| Binomial name | |
| Actinomyces naeslundii Thompson & Lovestedt 1951 | |
Actinomyces naeslundii is a Gram-positive, rod-shaped bacterium that occupies the oral cavity. The species has been implicated in periodontal disease, secondary enamel caries and primary root caries. These bacteria are also associated with good oral health. They are some of the first bacteria to occupy the oral cavity and colonize the tooth's surface.
Background
Gram-positive, pleomorphic nonspore-forming, nonacid-fast anaerobic or microaerophilic bacilli of the genus Actinomyces and the order Actinomycetales cause actinomycosis. Actinomycosis is a chronic bacterial disease, characterized by localized swelling with suppuration, abscess formation, tissue fibrosis, and draining sinuses.[1]
Infections of the oral and cervicofacial regions are the most commonly recognized infections; however, the thoracic region, abdominopelvic region, and the central nervous system also frequently can be involved. A. israelii, A. naeslundii, A. odontolyticus, A. viscosus, and A. meyeri are the most frequent microorganisms associated with human actinomycosis. A. gerencseriae also may cause disease in humans. Three coryneform bacteria now have been added to the Actinomyces genus and are thought to be potential causes for disease: A. neuii, A. radingae, and A. turicensis. A. radicidentis, a recently described species, has been isolated with polymerase chain reaction from patients with endodontic infections. Actinomyces species grow well in enriched media with brain-heart infusion and may be aided in growth by an atmosphere of 6-10% ambient carbon dioxide. They grow best at 37°C. Colonies can appear at three to seven days, but, to ensure that no growth is missed, cultures should be observed for up to 21 days. Actinomyces species are very closely related to Nocardia species, and at one time, both were considered to be fungal organisms. Propionibacterium propionicus and related species of bacteria also can cause actinomycosis-like disease. Aggregatibacter actinomycetemcomitans, Eikenella corrodens, species of Fusobacterium, Bacteroides, Capnocytophaga, Staphylococcus, Streptococcus, and Enterococcus are other bacteria concomitantly isolated with Actinomyces in clinical specimens of infected human tissues.
Pathophysiology
Actinomyces species that cause human disease do not exist freely in nature, but are normal flora of the oropharynx, gastrointestinal (GI) tract, and female genital tract. This is not an exogenous infection; therefore, no person-to-person spread of the pathogen occurs.
In general, Actinomyces species, being members of the normal flora, are agents of low pathogenicity and require disruption of the mucosal barrier to cause disease. Oral and cervicofacial diseases commonly are associated with dental procedures, trauma, oral surgery, or dental sepsis. Pulmonary infections usually arise after aspiration of oropharyngeal or GI secretions. GI infection frequently follows loss of mucosal integrity, such as with surgery, appendicitis, diverticulitis, trauma, or foreign bodies. Numerous reports have linked the use of intrauterine contraceptive devices to the development of actinomycosis of the female genital tract. The presence of a foreign body in this setting appears to trigger infection.
Other bacterial species that often are copathogens to Actinomyces species may aid spread of infection by inhibiting host defenses and reducing local oxygen tension. Once the organism is established locally, it spreads to surrounding tissues in a progressive manner, leading to a chronic, indurated, suppurative infection often with draining sinuses and fibrosis. In tissues, Actinomyces species grow in microscopic or macroscopic clusters of tangled filaments surrounded by neutrophils. When visible, these clusters are pale yellow and exude through sinus tracts; they are called sulfur granules. This is not an exclusive finding of actinomycosis, and its absence does not rule out the diagnosis. Other conditions, such as eumycetoma and nocardiosis, have been linked to the production of sulfur granules.