Abortion
| Induced abortion | |
|---|---|
| Classification and external resources | |
| ICD-10 | O04 |
| ICD-9 | 779.6 |
| DiseasesDB | 4153 |
| MedlinePlus | 002912 |
| eMedicine | article/252560 |
| Patient UK | Abortion |
Abortion is the ending of pregnancy by the removal or forcing out from the womb of a fetus or embryo before it is able to survive on its own.[note 1] An abortion can occur spontaneously, in which case it is often called a miscarriage. It can also be purposely caused in which case it is known as an induced abortion. The term abortion most commonly refers to the induced abortion of a human pregnancy. The similar procedure after the fetus may be able to survive on its own is medically known as a "late termination of pregnancy".[1][note 1]
Modern medicine uses medications or surgical methods for induced abortion. The two medications mifepristone and prostaglandin are as effective as a surgical method in the first trimester.[2][3] While the use of medications may be effective in the second trimester,[4] surgical methods appear to have a lower risk of side effects.[3] Birth control, including the pill and intrauterine devices can be started immediately after an abortion.[3] Abortion in the developed world has a long history of being among the safest procedures in medicine when allowed by local law.[5][6] Uncomplicated abortions do not cause either long term mental health or physical problems.[7] The World Health Organization recommends that this same level of safe and legal abortions be available to all women globally.[8] Unsafe abortions, however, result in approximately 47,000 maternal deaths[7] and 5 million hospital admissions per year globally.[9]
An estimated 44 million abortions are performed globally each year, with slightly under half of those performed unsafely.[10] Rates of abortions have changed little between 2003 and 2008,[10] after having previously spent decades declining as access to education regarding family planning and birth control improved.[11] As of 2008, forty percent of the world's women had access to legal induced abortions "without restriction as to reason".[12] There are; however, limits regarding how far along in pregnant they can be performed.[12]
Induced abortion has a long history. They have been performed by various methods, including herbal medicines, the use of sharpened tools, physical trauma, and other traditional methods since ancient times.[13] The laws surrounding abortion, how frequently they are performed, and their cultural and religious status vary greatly around the world. In some contexts, abortion is legal based on specific conditions, such as rape, problems with the fetus, socioeconomic factors, the risk to a mother's health or incest.[14] In many parts of the world there is prominent public controversy over the moral, ethical, and legal issues of abortion. Those who are against abortion generally state that an embryo or fetus is a human with the right to life and may compare abortion to murder.[15][16] Those who support abortion rights emphasize a woman's right to decide matters concerning her own body[17] as well as emphasizing human rights generally.[8]
Types
Induced
Approximately 205 million pregnancies occur each year worldwide. Over a third are unintended and about a fifth end in induced abortion.[10][18] Most abortions result from unintended pregnancies.[19][20] In the United Kingdom, 1 to 2% of abortions are done due to genetic problems in the fetus.[7] A pregnancy can be intentionally aborted in several ways. The manner selected often depends upon the gestational age of the embryo or fetus, which increases in size as the pregnancy progresses.[21][22] Specific procedures may also be selected due to legality, regional availability, and doctor or patient preference.
Reasons for procuring induced abortions are typically characterized as either therapeutic or elective. An abortion is medically referred to as a therapeutic abortion when it is performed to save the life of the pregnant woman; prevent harm to the woman's physical or mental health; terminate a pregnancy where indications are that the child will have a significantly increased chance of premature morbidity or mortality or be otherwise disabled; or to selectively reduce the number of fetuses to lessen health risks associated with multiple pregnancy.[23][24] An abortion is referred to as an elective or voluntary abortion when it is performed at the request of the woman for non-medical reasons.[24] Confusion sometimes arises over the term "elective" because "elective surgery" generally refers to all scheduled surgery, whether medically necessary or not.[25]
Spontaneous
Spontaneous abortion, also known as miscarriage, is the unintentional expulsion of an embryo or fetus before the 24th week of gestation.[26] A pregnancy that ends before 37 weeks of gestation resulting in a live-born infant is known as a "premature birth" or a "preterm birth".[27] When a fetus dies in utero after viability, or during delivery, it is usually termed "stillborn".[28] Premature births and stillbirths are generally not considered to be miscarriages although usage of these terms can sometimes overlap.[29]
Only 30% to 50% of conceptions progress past the first trimester.[30] The vast majority of those that do not progress are lost before the woman is aware of the conception,[24] and many pregnancies are lost before medical practitioners can detect an embryo.[31] Between 15% and 30% of known pregnancies end in clinically apparent miscarriage, depending upon the age and health of the pregnant woman.[32] 80% of these spontaneous abortions happen in the first trimester.[33]
The most common cause of spontaneous abortion during the first trimester is chromosomal abnormalities of the embryo or fetus,[24][34] accounting for at least 50% of sampled early pregnancy losses.[35] Other causes include vascular disease (such as lupus), diabetes, other hormonal problems, infection, and abnormalities of the uterus.[34] Advancing maternal age and a patient history of previous spontaneous abortions are the two leading factors associated with a greater risk of spontaneous abortion.[35] A spontaneous abortion can also be caused by accidental trauma; intentional trauma or stress to cause miscarriage is considered induced abortion or feticide.[36]
Methods
Medical
Medical abortions are those induced by abortifacient pharmaceuticals. Medical abortion became an alternative method of abortion with the availability of prostaglandin analogs in the 1970s and the antiprogestogen mifepristone in the 1980s.[37][38][39]
The most common early first-trimester medical abortion regimens use mifepristone in combination with a prostaglandin analog (misoprostol or gemeprost) up to 9 weeks gestational age, methotrexate in combination with a prostaglandin analog up to 7 weeks gestation, or a prostaglandin analog alone.[37] Mifepristone–misoprostol combination regimens work faster and are more effective at later gestational ages than methotrexate–misoprostol combination regimens, and combination regimens are more effective than misoprostol alone.[38] This regime is effective in the second trimester.[40]
In very early abortions, up to 7 weeks gestation, medical abortion using a mifepristone–misoprostol combination regimen is considered to be more effective than surgical abortion (vacuum aspiration), especially when clinical practice does not include detailed inspection of aspirated tissue.[41] Early medical abortion regimens using mifepristone, followed 24–48 hours later by buccal or vaginal misoprostol are 98% effective up to 9 weeks gestational age.[42] If medical abortion fails, surgical abortion must be used to complete the procedure.[43]
Early medical abortions account for the majority of abortions before 9 weeks gestation in Britain,[44][45] France,[46] Switzerland,[47] and the Nordic countries.[48] In the United States, the percentage of early medical abortions is far lower.[49][50]
Medical abortion regimens using mifepristone in combination with a prostaglandin analog are the most common methods used for second-trimester abortions in Canada, most of Europe, China and India,[39] in contrast to the United States where 96% of second-trimester abortions are performed surgically by dilation and evacuation.[51]
Surgical
.svg.png)
1: Amniotic sac
2: Embryo
3: Uterine lining
4: Speculum
5: Vacurette
6: Attached to a suction pump
Up to 15 weeks' gestation, suction-aspiration or vacuum aspiration are the most common surgical methods of induced abortion.[52] Manual vacuum aspiration (MVA) consists of removing the fetus or embryo, placenta, and membranes by suction using a manual syringe, while electric vacuum aspiration (EVA) uses an electric pump. These techniques differ in the mechanism used to apply suction, in how early in pregnancy they can be used, and in whether cervical dilation is necessary.
MVA, also known as "mini-suction" and "menstrual extraction", can be used in very early pregnancy, and does not require cervical dilation. Dilation and curettage (D&C), the second most common method of surgical abortion, is a standard gynecological procedure performed for a variety of reasons, including examination of the uterine lining for possible malignancy, investigation of abnormal bleeding, and abortion. Curettage refers to cleaning the walls of the uterus with a curette. The World Health Organization recommends this procedure, also called sharp curettage, only when MVA is unavailable.[53]
From the 15th week of gestation until approximately the 26th, other techniques must be used. Dilation and evacuation (D&E) consists of opening the cervix of the uterus and emptying it using surgical instruments and suction. Premature labor and delivery can be induced with prostaglandin; this can be coupled with injecting the amniotic fluid with hypertonic solutions containing saline or urea. After the 16th week of gestation, abortions can also be induced by intact dilation and extraction (IDX) (also called intrauterine cranial decompression), which requires surgical decompression of the fetus's head before evacuation. IDX is sometimes called "partial-birth abortion," which has been federally banned in the United States.
In the third trimester of pregnancy, abortion may be performed by IDX as described above, induction of labor, or by hysterotomy. Hysterotomy abortion is a procedure similar to a caesarean section and is performed under general anesthesia. It requires a smaller incision than a caesarean section and is used during later stages of pregnancy.[54]
First-trimester procedures can generally be performed using local anesthesia, while second-trimester methods may require deep sedation or general anesthesia.[50]
Other methods
Historically, a number of herbs reputed to possess abortifacient properties have been used in folk medicine: tansy, pennyroyal, black cohosh, and the now-extinct silphium (see history of abortion).[55] The use of herbs in such a manner can cause serious—even lethal—side effects, such as multiple organ failure, and is not recommended by physicians.[56]
Abortion is sometimes attempted by causing trauma to the abdomen. The degree of force, if severe, can cause serious internal injuries without necessarily succeeding in inducing miscarriage.[57] In Southeast Asia, there is an ancient tradition of attempting abortion through forceful abdominal massage.[58] One of the bas reliefs decorating the temple of Angkor Wat in Cambodia depicts a demon performing such an abortion upon a woman who has been sent to the underworld.[58]
Reported methods of unsafe, self-induced abortion include misuse of misoprostol, and insertion of non-surgical implements such as knitting needles and clothes hangers into the uterus. These methods are rarely seen in developed countries where surgical abortion is legal and available.[59]
Safety
The health risks of abortion depend on whether the procedure is performed safely or unsafely. The World Health Organization defines unsafe abortions as those performed by unskilled individuals, with hazardous equipment, or in unsanitary facilities.[60] Legal abortions performed in the developed world are among the safest procedures in medicine.[5][61] In the US, the risk of maternal death from abortion is 0.7 per 100,000 procedures,[6] making abortion about 13 times safer for women than childbirth (8.8 maternal deaths per 100,000 live births).[62][63] This is equivalent to the risk of death from driving about 1200 km (760 miles).[6] The risk of abortion-related mortality increases with gestational age, but remains lower than that of childbirth through at least 21 weeks' gestation.[64][65][66]
Vacuum aspiration in the first trimester is the safest method of surgical abortion, and can be performed in a primary care office, abortion clinic, or hospital. Complications are rare and can include uterine perforation, pelvic infection, and retained products of conception requiring a second procedure to evacuate.[67] Preventive antibiotics (such as doxycycline or metronidazole) are typically given before elective abortion,[68] as they are believed to substantially reduce the risk of postoperative uterine infection.[50][69] Complications after second-trimester abortion are similar to those after first-trimester abortion, and depend somewhat on the method chosen.
There is little difference in terms of safety and efficacy between medical abortion using a combined regimen of mifepristone and misoprostol and surgical abortion (vacuum aspiration) in early first trimester abortions up to 9 weeks gestation.[41] Medical abortion using the prostaglandin analog misoprostol alone is less effective and more painful than medical abortion using a combined regimen of mifepristone and misoprostol or surgical abortion.[70][71]
Some purported risks of abortion are promoted primarily by anti-abortion groups, but lack scientific support.[72] For example, the question of a link between induced abortion and breast cancer has been investigated extensively. Major medical and scientific bodies (including the World Health Organization, the US National Cancer Institute, the American Cancer Society, the Royal College of Obstetricians and Gynaecologists and the American Congress of Obstetricians and Gynecologists) have concluded that abortion does not cause breast cancer,[73] although such a link continues to be promoted by anti-abortion groups.[72]
Similarly, evidence indicates that induced abortion does not cause mental-health problems.[7][74] The American Psychological Association has concluded that a single abortion is not a threat to women's mental health, and that women are no more likely to have mental-health problems after a first-trimester abortion than after carrying an unwanted pregnancy to term.[75][76] Abortions performed after the first trimester because of fetal abnormalities are not thought to cause mental-health problems.[77] Some proposed negative psychological effects of abortion have been referred to by anti-abortion advocates as a separate condition called "post-abortion syndrome", which is not recognized by any medical or psychological organization.[78]
Unsafe abortion

Women seeking to terminate their pregnancies sometimes resort to unsafe methods, particularly when access to legal abortion is restricted. They may attempt to self-abort or rely on another person who does not have proper medical training or access to proper facilities. This has a tendency to lead to severe complications, such as incomplete abortion, sepsis, hemorrhage, and damage to internal organs.[79]
Unsafe abortions are a major cause of injury and death among women worldwide. Although data are imprecise, it is estimated that approximately 20 million unsafe abortions are performed annually, with 97% taking place in developing countries.[5] Unsafe abortions are believed to result in millions of injuries.[5][80] Estimates of deaths vary according to methodology, and have ranged from 37,000 to 70,000 in the past decade;[5][9][81] deaths from unsafe abortion account for around 13% of all maternal deaths.[82] The World Health Organization believes that mortality has fallen since the 1990s.[83] To reduce the number of unsafe abortions, public health organizations have generally advocated emphasizing the legalization of abortion, training of medical personnel, and ensuring access to reproductive-health services.[84]
The legality of abortion is one of the main determinants of its safety. Countries with restrictive abortion laws have significantly higher rates of unsafe abortion (and similar overall abortion rates) compared to those where abortion is legal and available.[9][10][84][85][86][87] For example, the 1996 legalization of abortion in South Africa had an immediate positive impact on the frequency of abortion-related complications,[88] with abortion-related deaths dropping by more than 90%.[89] In addition, a lack of access to effective contraception contributes to unsafe abortion. It has been estimated that the incidence of unsafe abortion could be reduced by up to 75% (from 20 million to 5 million annually) if modern family planning and maternal health services were readily available globally.[90]
Forty percent of the world's women are able to access therapeutic and elective abortions within gestational limits,[12] while an additional 35 percent have access to legal abortion if they meet certain physical, mental, or socioeconomic criteria.[14] While maternal mortality seldom results from safe abortions, unsafe abortions result in 70,000 deaths and 5 million disabilities per year.[9] Complications of unsafe abortion account for approximately an eighth of maternal mortalities worldwide,[91] though this varies by region.[92] Secondary infertility caused by an unsafe abortion affects an estimated 24 million women.[86] The rate of unsafe abortions has increased from 44% to 49% between 1995 and 2008.[10] Health education, access to family planning, and improvements in health care during and after abortion have been proposed to address this phenomenon.[93]
Incidence
There are two commonly used methods of measuring the incidence of abortion:
- Abortion rate – number of abortions per 1000 women between 15 and 44 years of age
- Abortion percentage – number of abortions out of 100 known pregnancies (pregnancies include live births, abortions and miscarriages)
The number of abortions performed worldwide has remained stable in recent years, with 41.6 million having been performed in 2003 and 43.8 million having been performed in 2008.[10] The abortion rate worldwide was 28 per 1000 women, though it was 24 per 1000 women for developed countries and 29 per 1000 women for developing countries.[10] The same 2012 study indicated that in 2008, the estimated abortion percentage of known pregnancies was at 21% worldwide, with 26% in developed countries and 20% in developing countries.[10]
On average, the incidence of abortion is similar in countries with restrictive abortion laws and those with more liberal access to abortion. However, restrictive abortion laws are associated with increases in the percentage of abortions which are performed unsafely.[12][94][95] The unsafe abortion rate in developing countries is partly attributable to lack of access to modern contraceptives; according to the Guttmacher Institute, providing access to contraceptives would result in about 14.5 million fewer unsafe abortions and 38,000 fewer deaths from unsafe abortion annually worldwide.[96]
The rate of legal, induced abortion varies extensively worldwide. According to the report of employees of Guttmacher Institute it ranged from 7 per 1000 women (Germany and Switzerland) to 30 per 1000 women (Estonia) in countries with complete statistics in 2008. The proportion of pregnancies that ended in induced abortion ranged from about 10% (Israel, the Neatherlands and Switzerland) to 30% (Estonia) in the same group, though it might be as high as 36% in Hungary and Romania, whose statistics were deemed incomplete.[97][98]
The abortion rate may also be expressed as the average number of abortions a woman has during her reproductive years; this is referred to as total abortion rate (TAR).
Gestational age and method
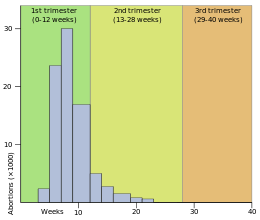
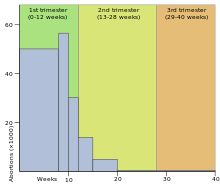
Abortion in the United States by gestational age, 2004. (Data source: Centers for Disease Control and Prevention) (right)
Abortion rates also vary depending on the stage of pregnancy and the method practiced. In 2003, the Centers for Disease Control and Prevention (CDC) reported that 26% of abortions in the United States were known to have been obtained at less than 6 weeks' gestation, 18% at 7 weeks, 15% at 8 weeks, 18% at 9 through 10 weeks, 9.7% at 11 through 12 weeks, 6.2% at 13 through 15 weeks, 4.1% at 16 through 20 weeks and 1.4% at more than 21 weeks. 90.9% of these were classified as having been done by "curettage" (suction-aspiration, dilation and curettage, dilation and evacuation), 7.7% by "medical" means (mifepristone), 0.4% by "intrauterine instillation" (saline or prostaglandin), and 1.0% by "other" (including hysterotomy and hysterectomy).[99] According to the CDC, due to data collection difficulties the data must be viewed as tentative and some fetal deaths reported beyond 20 weeks may be natural deaths erroneously classified as abortions if the removal of the fetus is accomplished by the same procedure as an induced abortion.[100]
The Guttmacher Institute estimated there were 2,200 intact dilation and extraction procedures in the US during 2000; this accounts for 0.17% of the total number of abortions performed that year.[101] Similarly, in England and Wales in 2006, 89% of terminations occurred at or under 12 weeks, 9% between 13 to 19 weeks, and 1.5% at or over 20 weeks. 64% of those reported were by vacuum aspiration, 6% by D&E, and 30% were medical.[102] There are more second trimester abortions in developing countries such as China, India and Vietnam than in developed countries.[103]
Motivation
Personal
The reasons why women have abortions are diverse and vary across the world.[100][104]

Some of the most common reasons are to postpone childbearing to a more suitable time or to focus energies and resources on existing children. Others include being unable to afford a child either in terms of the direct costs of raising a child or the loss of income while she is caring for the child, lack of support from the father, inability to afford additional children, desire to provide schooling for existing children, disruption of one's own education, relationship problems with their partner, a perception of being too young to have a child, unemployment, and not being willing to raise a child conceived as a result of rape or incest, among others.[104][105]
Societal
Some abortions are undergone as the result of societal pressures. These might include the preference for children of a specific sex or race,[106] disapproval of single or early motherhood, stigmatization of people with disabilities, insufficient economic support for families, lack of access to or rejection of contraceptive methods, or efforts toward population control (such as China's one-child policy). These factors can sometimes result in compulsory abortion or sex-selective abortion.[107]
An American study in 2002 concluded that about half of women having abortions were using a form of contraception at the time of becoming pregnant. Inconsistent use was reported by half of those using condoms and three-quarters of those using the birth-control pill; 42% of those using condoms reported failure through slipping or breakage.[108] The Guttmacher Institute estimated that "most abortions in the United States are obtained by minority women" because minority women "have much higher rates of unintended pregnancy."[109]
Maternal and fetal health
An additional factor is risk to maternal or fetal health, which was cited as the primary reason for abortion in over a third of cases in some countries and as a significant factor in only a single-digit percentage of abortions in other countries.[100][104]
In the U.S., the Supreme Court decisions in Roe vs Wade and Doe vs Bolton: "ruled that the state's interest in the life of the fetus became compelling only at the point of viability, defined as the point at which the fetus can survive independently of its mother. Even after the point of viability, the state cannot favor the life of the fetus over the life or health of the pregnant woman. Under the right of privacy, physicians must be free to use their "medical judgment for the preservation of the life or health of the mother." On the same day that the Court decided Roe, it also decided Doe v. Bolton, in which the Court defined health very broadly: "The medical judgment may be exercised in the light of all factors—physical, emotional, psychological, familial, and the woman's age—relevant to the well-being of the patient. All these factors may relate to health. This allows the attending physician the room he needs to make his best medical judgment."[110]:1200–1201
Public opinion shifted in America following television personality Sherri Finkbine's discovery during her fifth month of pregnancy that she had been exposed to thalidomide, unable to abort in the United States she traveled to Sweden. From 1962-65 there was an outbreak of German measles that left 15,000 babies with severe birth defects. In 1967, the American Medical Association publicly supported liberalization of abortion laws. A National Opinion Research Center poll in 1965 showed 73% supported abortion when the mothers life was at risk, 57% when birth defects were present and 59% for pregnancies resulting from rape or incest. [111]
Cancer
The rate of cancer during pregnancy is 0.02–1%, and in many cases, cancer of the mother leads to consideration of abortion to protect the life of the mother, or in response to the potential damage that may occur to the fetus during treatment. This is particularly true for cervical cancer, the most common type which occurs in 1 of every 2000-13000 pregnancies, for which initiation of treatment "cannot co-exist with preservation of fetal life (unless neoadjuvant chemotherapy is chosen)." Very early stage cervical cancers (I and IIa) may be treated by radical hysterectomy and pelvic lymph node dissection, radiation therapy, or both, while later stages are treated by radiotherapy. Chemotherapy may be used simultaneously. Treatment of breast cancer during pregnancy also involves fetal considerations, because lumpectomy is discouraged in favor of modified radical mastectomy unless late-term pregnancy allows follow-up radiation therapy to be administered after the birth.[112]
Exposure to a single chemotherapy drug is estimated to cause a 7.5–17% risk of teratogenic effects on the fetus, with higher risks for multiple drug treatments. Treatment with more than 40 Gy of radiation usually causes spontaneous abortion. Exposure to much lower doses during the first trimester, especially 8 to 15 weeks of development, can cause intellectual disability or microcephaly, and exposure at this or subsequent stages can cause reduced intrauterine growth and birth weight. Exposures above 0.005–0.025 Gy cause a dose-dependent reduction in IQ.[112] It is possible to greatly reduce exposure to radiation with abdominal shielding, depending on how far the area to be irradiated is from the fetus.[113][114]
The process of birth itself may also put the mother at risk. "Vaginal delivery may result in dissemination of neoplastic cells into lymphovascular channels, haemorrhage, cervical laceration and implantation of malignant cells in the episiotomy site, while abdominal delivery may delay the initiation of non-surgical treatment."[115]
History


Induced abortion has long history, and can be traced back to civilizations as varied as China under Shennong (c. 2700 BCE), Ancient Egypt with its Ebers Papyrus (c. 1550 BCE), and the Roman Empire in the time of Juvenal (c. 200 CE).[13] There is evidence to suggest that pregnancies were terminated through a number of methods, including the administration of abortifacient herbs, the use of sharpened implements, the application of abdominal pressure, and other techniques. One of the earliest known artistic representations of abortion is in a bas relief at Angkor Wat (c. 1150). Found in a series of friezes that represent judgment after death in Hindu and Buddhist culture, it depicts the technique of abdominal abortion.[58]
Some medical scholars and abortion opponents have suggested that the Hippocratic Oath forbade Ancient Greek physicians from performing abortions;[13] other scholars disagree with this interpretation,[13] and state the medical texts of Hippocratic Corpus contain descriptions of abortive techniques.[117] Aristotle, in his treatise on government Politics (350 BCE), condemns infanticide as a means of population control. He preferred abortion in such cases, with the restriction[118] "[that it] must be practised on it before it has developed sensation and life; for the line between lawful and unlawful abortion will be marked by the fact of having sensation and being alive."[119] In Christianity, Pope Sixtus V (1585–90) was the first Pope to declare that abortion is homicide regardless of the stage of pregnancy;[120] the Catholic Church had previously been divided on whether it believed that abortion was murder, and did not begin vigorously opposing abortion until the 19th century.[13] Islamic tradition has traditionally permitted abortion until a point in time when Muslims believe the soul enters the fetus,[13] considered by various theologians to be at conception, 40 days after conception, 120 days after conception, or quickening.[121] However, abortion is largely heavily restricted or forbidden in areas of high Islamic faith such as the Middle East and North Africa.[122]
In Europe and North America, abortion techniques advanced starting in the 17th century. However, conservatism by most physicians with regards to sexual matters prevented the wide expansion of safe abortion techniques.[13] Other medical practitioners in addition to some physicians advertised their services, and they were not widely regulated until the 19th century, when the practice was banned in both the United States and the United Kingdom.[13] Church groups as well as physicians were highly influential in anti-abortion movements.[13] In the US, abortion was more dangerous than childbirth until about 1930 when incremental improvements in abortion procedures relative to childbirth made abortion safer.[note 2] The Soviet Union (1919), Iceland (1935) and Sweden (1938) were among the first countries to legalize certain or all forms of abortion.[123] In 1935 Nazi Germany, a law was passed permitting abortions for those deemed "hereditarily ill", while women considered of German stock were specifically prohibited from having abortions.[124] Beginning in the second half of the twentieth century, abortion was legalized in a greater number of countries.[13] A bill passed by the state legislature of New York legalizing abortion was signed by Governor Nelson Rockefeller in April 1970.[125]
Society and culture
Abortion debate
Induced abortion has long been the source of considerable debate, controversy, and activism. An individual's position concerning the complex ethical, moral, philosophical, biological, and legal issues which surround abortion is often related to his or her value system. Opinions of abortion may be described as being a combination of beliefs about abortion's morality, beliefs about the proper extent of governmental authority in public policy, and beliefs about the rights and responsibilities of the woman seeking to have an abortion. Religious ethics also has an influence both on personal opinion and on the greater debate over abortion.
In both public and private debate, arguments presented in favor of or against abortion access focus on either the moral permissibility of an induced abortion, or justification of laws permitting or restricting abortion. Abortion debates, especially pertaining to abortion laws, are often spearheaded by groups advocating one of these two positions. Anti-abortion groups who favor greater legal restrictions on abortion, including complete prohibition, most often describe themselves as "pro-life" while abortion rights groups who are against such legal restrictions describe themselves as "pro-choice". Generally, the former position argues that a human fetus is a human being with a right to live, making abortion morally the same as murder. The latter position argues that a woman has certain reproductive rights, especially the choice whether or not to carry a pregnancy to term.
Modern abortion law
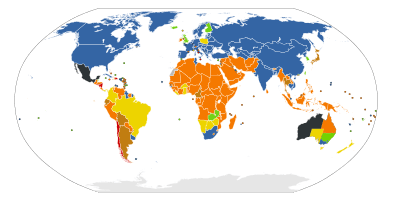
International status of abortion law
UN 2013 report on abortion law.[126]
Current laws pertaining to abortion are diverse. Religious, moral, and cultural sensibilities continue to influence abortion laws throughout the world. The right to life, the right to liberty, the right to security of person, and the right to reproductive health are major issues of human rights that are sometimes used as justification for the existence or absence of laws controlling abortion.
In jurisdictions where abortion is legal, certain requirements must often be met before a woman may obtain a safe, legal abortion (an abortion performed without the woman's consent is considered feticide). These requirements usually depend on the age of the fetus, often using a trimester-based system to regulate the window of legality. Some jurisdictions require a waiting period before the procedure, prescribe the distribution of information on fetal development, or require that parents be contacted if their minor daughter requests an abortion.[128] Other jurisdictions may require that a woman obtain the consent of the fetus' father before aborting the fetus, that abortion providers inform patients of health risks of the procedure—sometimes including "risks" not supported by the medical literature—and that multiple medical authorities certify that the abortion is either medically or socially necessary. Many restrictions are waived in emergency situations. China, which has a one-child policy, has at times incorporated mandatory abortions as part of their population control strategy.[129]
Other jurisdictions ban abortion almost entirely. Many, but not all, of these allow legal abortions in a variety of circumstances. These circumstances vary based on jurisdiction, but may include whether the pregnancy is a result of rape or incest, the fetus' development is impaired, the woman's physical or mental well-being is endangered, or socioeconomic considerations make childbirth a hardship.[14] In countries where abortion is banned entirely, such as Nicaragua, medical authorities have recorded rises in maternal death directly and indirectly due to pregnancy as well as deaths due to doctors' fears of prosecution if they treat other gynecological emergencies.[130][131] Some countries, such as Bangladesh, that nominally ban abortion, may also support clinics that perform abortions under the guise of menstrual hygiene.[132] This is also a terminology in traditional medicine.[133] In places where abortion is illegal or carries heavy social stigma, pregnant women may engage in medical tourism and travel to countries where they can terminate their pregnancies.[134] Women without the means to travel can resort to providers of illegal abortions or attempt to perform an abortion by themselves.[135]
Emergency contraception is generally available in countries that have not restricted abortion and is also sometimes available in countries that have otherwise banned abortion, such as Chile.[136][137] This has caused controversy, as some anti-abortion groups assert that certain forms of emergency contraception are not contraceptives but abortifacients (See, e.g., Abortion in the Dominican Republic.)
Sex-selective abortion
Sonography and amniocentesis allow parents to determine sex before childbirth. The development of this technology has led to sex-selective abortion, or the termination of a fetus based on sex. The selective termination of a female fetus is most common.
Sex-selective abortion is partially responsible for the noticeable disparities between the birth rates of male and female children in some countries. The preference for male children is reported in many areas of Asia, and abortion used to limit female births has been reported in Taiwan, South Korea, India, and China.[138] This deviation from the standard birth rates of males and females occurs despite the fact that the country in question may have officially banned sex-selective abortion or even sex-screening.[139][140][141][142] In China, a historical preference for a male child has been exacerbated by the one-child policy, which was enacted in 1979.[143]
Many countries have taken legislative steps to reduce the incidence of sex-selective abortion. At the International Conference on Population and Development in 1994 over 180 states agreed to eliminate "all forms of discrimination against the girl child and the root causes of son preference",[144] which was also condemned by a PACE resolution in 2011.[145] The World Health Organization and UNICEF, along with other United Nations agencies, have found that measures to reduce access to abortion are much less effective at reducing sex-selective abortions than measures to reduce gender inequality.[144]
Anti-abortion violence
In a number of cases, abortion providers and these facilities have been subjected to various forms of violence, including murder, attempted murder, kidnapping, stalking, assault, arson, and bombing. Anti-abortion violence is classified by both governmental and scholarly sources as terrorism.[146][147] Only a small fraction of those opposed to abortion commit violence.
In the United States, four physicians who performed abortions have been murdered: David Gunn (1993), John Britton (1994), Barnett Slepian (1998), and George Tiller (2009). Also murdered, in the U.S. and Australia, have been other personnel at abortion clinics, including receptionists and security guards such as James Barrett, Shannon Lowney, Lee Ann Nichols, and Robert Sanderson. Woundings (e.g., Garson Romalis) and attempted murders have also taken place in the United States and Canada. Hundreds of bombings, arsons, acid attacks, invasions, and incidents of vandalism against abortion providers have occurred.[148][149] Notable perpetrators of anti-abortion violence include Eric Robert Rudolph, Scott Roeder, Shelley Shannon, and Paul Jennings Hill, the first person to be executed in the United States for murdering an abortion provider.[150]
Legal protection of access to abortion has been brought into some countries where abortion is legal. These laws typically seek to protect abortion clinics from obstruction, vandalism, picketing, and other actions, or to protect patients and employees of such facilities from threats and harassment.
Far more common than physical violence is psychological pressure. In 2003, Chris Danze organized pro-life organizations throughout Texas to prevent the construction of a Planned Parenthood facility in Austin. The organizations released the personal information online, of those involved with construction, sending them up to 1200 phone calls a day and contacting their churches.[151] Some protestors record patients on camera.[151]
Other animals
Spontaneous abortion occurs in various animals. For example, in sheep, it may be caused by crowding through doors, or being chased by dogs.[152] In cows, abortion may be caused by contagious disease, such as Brucellosis or Campylobacter, but can often be controlled by vaccination.[153] Eating pine needles can also induce abortions in cows.[154][155] In horses, a fetus may be aborted or resorbed if it has lethal white syndrome (congenital intestinal aganglionosis). Foal embryos that are homozygous for the dominant white gene (WW) are theorized to also be aborted or resorbed before birth.[156]
Viral infection can cause abortion in dogs.[157] Cats can experience spontaneous abortion for many reasons, including hormonal imbalance. A combined abortion and spaying is performed on pregnant cats, especially in Trap-Neuter-Return programs, to prevent unwanted kittens from being born.[158][159][160] Female rodents may terminate a pregnancy when exposed to the smell of a male not responsible for the pregnancy, known as the Bruce effect.[161]
Abortion may also be induced in animals, in the context of animal husbandry. For example, abortion may be induced in mares that have been mated improperly, or that have been purchased by owners who did not realize the mares were pregnant, or that are pregnant with twin foals.[162] Feticide can occur in horses and zebras due to male harassment of pregnant mares or forced copulation,[163][164][165] although the frequency in the wild has been questioned.[166] Male gray langur monkeys may attack females following male takeover, causing miscarriage.[167]
References
Citations
- ↑ Grimes, DA; Stuart, G (2010). "Abortion jabberwocky: the need for better terminology". Contraception 81 (2): 93–6. doi:10.1016/j.contraception.2009.09.005. PMID 20103443.
- ↑ Kulier, R; Kapp, N; Gülmezoglu, AM; Hofmeyr, GJ; Cheng, L; Campana, A (Nov 9, 2011). "Medical methods for first trimester abortion.". The Cochrane database of systematic reviews (11): CD002855. doi:10.1002/14651858.CD002855.pub4. PMID 22071804.
- ↑ 3.0 3.1 3.2 Kapp, N; Whyte, P; Tang, J; Jackson, E; Brahmi, D (Sep 2013). "A review of evidence for safe abortion care.". Contraception 88 (3): 350–63. doi:10.1016/j.contraception.2012.10.027. PMID 23261233.
- ↑ Wildschut, H; Both, MI; Medema, S; Thomee, E; Wildhagen, MF; Kapp, N (Jan 19, 2011). "Medical methods for mid-trimester termination of pregnancy.". The Cochrane database of systematic reviews (1): CD005216. doi:10.1002/14651858.CD005216.pub2. PMID 21249669.
- ↑ 5.0 5.1 5.2 5.3 5.4 Grimes, D. A.; Benson, J.; Singh, S.; Romero, M.; Ganatra, B.; Okonofua, F. E.; Shah, I. H. (2006). "Unsafe abortion: The preventable pandemic" (PDF). The Lancet 368 (9550): 1908–1919. doi:10.1016/S0140-6736(06)69481-6. PMID 17126724.
- ↑ 6.0 6.1 6.2 Raymond, EG; Grossman, D; Weaver, MA; Toti, S; Winikoff, B (Nov 2014). "Mortality of induced abortion, other outpatient surgical procedures and common activities in the United States.". Contraception 90 (5): 476–479. doi:10.1016/j.contraception.2014.07.012. PMID 25152259.
- ↑ 7.0 7.1 7.2 7.3 Lohr, P. A.; Fjerstad, M.; Desilva, U.; Lyus, R. (2014). "Abortion". BMJ 348: f7553. doi:10.1136/bmj.f7553.
- ↑ 8.0 8.1 Organization, World Health (2012). Safe abortion: technical and policy guidance for health systems (PDF) (2nd ed. ed.). Geneva: World Health Organization. p. 8. ISBN 9789241548434.
- ↑ 9.0 9.1 9.2 9.3 Shah, I.; Ahman, E. (December 2009). "Unsafe abortion: global and regional incidence, trends, consequences, and challenges" (PDF). Journal of Obstetrics and Gynaecology Canada 31 (12): 1149–58. PMID 20085681.
- ↑ 10.0 10.1 10.2 10.3 10.4 10.5 10.6 10.7 Sedgh, G.; Singh, S.; Shah, I. H.; Åhman, E.; Henshaw, S. K.; Bankole, A. (2012). "Induced abortion: Incidence and trends worldwide from 1995 to 2008" (PDF). The Lancet 379 (9816): 625–632. doi:10.1016/S0140-6736(11)61786-8. PMID 22264435.
- ↑ Sedgh G, Henshaw SK, Singh S, Bankole A, Drescher J (September 2007). "Legal abortion worldwide: incidence and recent trends". Int Fam Plan Perspect 33 (3): 106–116. doi:10.1363/ifpp.33.106.07. PMID 17938093.
- ↑ 12.0 12.1 12.2 12.3 Culwell KR, Vekemans M, de Silva U, Hurwitz M (July 2010). "Critical gaps in universal access to reproductive health: Contraception and prevention of unsafe abortion". International Journal of Gynecology & Obstetrics 110: S13–16. doi:10.1016/j.ijgo.2010.04.003. PMID 20451196.
- ↑ 13.0 13.1 13.2 13.3 13.4 13.5 13.6 13.7 13.8 13.9 Joffe, Carole (2009). "1. Abortion and medicine: A sociopolitical history". In MPaul, ES Lichtenberg, L Borgatta, DA Grimes, PG Stubblefield, MD Creinin. Management of Unintended and Abnormal Pregnancy (PDF) (1st ed.). Oxford, United Kingdom: John Wiley & Sons, Ltd. ISBN 978-1-4443-1293-5. Archived from the original on 21 October 2011.
- ↑ 14.0 14.1 14.2 Boland, R.; Katzive, L. (2008). "Developments in Laws on Induced Abortion: 1998–2007". International Family Planning Perspectives 34 (3): 110–120. doi:10.1363/ifpp.34.110.08. PMID 18957353.
- ↑ Pastor Mark Driscoll (18 October 2013). "What do 55 million people have in common?". Fox News. Retrieved 2 July 2014.
- ↑ Dale Hansen (18 March 2014). "Abortion: Murder, or Medical Procedure?". Huffington Post. Retrieved 2 July 2014.
- ↑ Sifris, Ronli Noa (2013). Reproductive Freedom, Torture and International Human Rights Challenging the Masculinisation of Torture. Hoboken: Taylor and Francis. p. 3. ISBN 9781135115227.
- ↑ Cheng L. (1 November 2008). "Surgical versus medical methods for second-trimester induced abortion". The WHO Reproductive Health Library. World Health Organization. Archived from the original on 17 June 2011. Retrieved 17 June 2011.
- ↑ Bankole et al. (1998). "Reasons Why Women Have Induced Abortions: Evidence from 27 Countries". International Family Planning Perspectives 24 (3): 117–127 & 152. doi:10.2307/3038208.
- ↑ Finer, Lawrence B.; Frohwirth, Lori F.; Dauphinee, Lindsay A.; Singh, Susheela; Moore, Ann M. (2005). "Reasons U.S. Women Have Abortions: Quantitative and Qualitative Perspectives" (PDF). Perspectives on Sexual and Reproductive Health 37 (3): 110–118. doi:10.1111/j.1931-2393.2005.tb00045.x. PMID 16150658.
- ↑ Stubblefield, Phillip G. (2002). "10. Family Planning". In Berek, Jonathan S. Novak's Gynecology (13 ed.). Lippincott Williams & Wilkins. ISBN 978-0-7817-3262-8.
- ↑ Bartlett, LA; Berg, CJ; Shulman, HB; Zane, SB; Green, CA; Whitehead, S; Atrash, HK (2004). "Risk factors for legal induced abortion-related mortality in the United States" (PDF). Obstetrics & Gynecology 103 (4): 729–37. doi:10.1097/01.AOG.0000116260.81570.60. PMID 15051566.
- ↑ Roche, Natalie E. (28 September 2004). "Therapeutic Abortion". eMedicine. Archived from the original on 14 December 2004. Retrieved 19 June 2011.
- ↑ 24.0 24.1 24.2 24.3 Schorge, John O.; Schaffer, Joseph I.; Halvorson, Lisa M.; Hoffman, Barbara L.; Bradshaw, Karen D.; Cunningham, F. Gary, eds. (2008). "6. First-Trimester Abortion". Williams Gynecology (1 ed.). McGraw-Hill Medical. ISBN 978-0-07-147257-9.
- ↑ "Elective surgery". Encyclopedia of Surgery. Retrieved 17 December 2012. "An elective surgery is a planned, non-emergency surgical procedure. It may be either medically required (e.g., cataract surgery), or optional (e.g., breast augmentation or implant) surgery.
- ↑ Churchill Livingstone medical dictionary. Edinburgh New York: Churchill Livingstone Elsevier. 2008. ISBN 978-0-443-10412-1.
The preferred term for unintentional loss of the product of conception prior to 24 weeks' gestation is miscarriage.
- ↑ Annas, George J.; Elias, Sherman (2007). "51. Legal and Ethical Issues in Obstetric Practice". In Gabbe, Steven G.; Niebyl, Jennifer R.; Simpson, Joe Leigh. Obstetrics: Normal and Problem Pregnancies (5 ed.). Churchill Livingstone. p. 669. ISBN 978-0-443-06930-7.
A preterm birth is defined as one that occurs before the completion of 37 menstrual weeks of gestation, regardless of birth weight.
- ↑ "Stillbirth". Concise Medical Dictionary. Oxford University Press. 2010.
birth of a fetus that shows no evidence of life (heartbeat, respiration, or independent movement) at any time later than 24 weeks after conception
- ↑ "Documenting Stillbirth (Fetal Death)". United States Department of State. 18 February 2011. Archived from the original (PDF) on 27 June 2011. Retrieved 27 June 2011.
- ↑ Annas, George J.; Elias, Sherman (2007). "24. Pregnancy loss". In Gabbe, Steven G.; Niebyl, Jennifer R.; Simpson, Joe Leigh. Obstetrics: Normal and Problem Pregnancies (5 ed.). Churchill Livingstone. ISBN 978-0-443-06930-7.
- ↑ Katz, Vern L. (2007). "16. Spontaneous and Recurrent Abortion – Etiology, Diagnosis, Treatment". In Katz, Vern L.; Lentz, Gretchen M.; Lobo, Rogerio A.; Gershenson, David M. Katz: Comprehensive Gynecology (5 ed.). Mosby. ISBN 978-0-323-02951-3.
- ↑ Stovall, Thomas G. (2002). "17. Early Pregnancy Loss and Ectopic Pregnancy". In Berek, Jonathan S. Novak's Gynecology (13 ed.). Lippincott Williams & Wilkins. ISBN 978-0-7817-3262-8.
- ↑ Cunningham, F. Gary; Leveno, Kenneth J.; Bloom, Steven L.; Spong, Catherine Y.; Dashe, Jodi S.; Hoffman, Barbara L.; Casey, Brian M.; Sheffield, Jeanne S., eds. (2014). Williams Obstetrics (24th ed.). McGraw Hill Education. ISBN 978-0-07-179893-8.
- ↑ 34.0 34.1 Stöppler, Melissa Conrad. Shiel, William C., Jr., ed. "Miscarriage (Spontaneous Abortion)". MedicineNet.com. WebMD. Retrieved 7 April 2009.
- ↑ 35.0 35.1 Jauniaux E, Kaminopetros P, El-Rafaey H (1999). "Early pregnancy loss". In Whittle MJ, Rodeck CH. Fetal medicine: basic science and clinical practice. Edinburgh: Churchill Livingstone. p. 837. ISBN 978-0-443-05357-3. OCLC 42792567.
- ↑ "Fetal Homicide Laws". National Conference of State Legislatures. Archived from the original on 29 March 2009. Retrieved 7 April 2009.
- ↑ 37.0 37.1 Kulier R, Kapp N, Gülmezoglu AM, Hofmeyr GJ, Cheng L, Campana A (2011). "Medical methods for first trimester abortion". Cochrane Database Syst Rev 11 (11): CD002855. doi:10.1002/14651858.CD002855.pub4. PMID 22071804.
- ↑ 38.0 38.1 Creinin MD, Gemzell-Danielsson K (2009). "Medical abortion in early pregnancy". In Paul M, Lichtenberg ES, Borgatta L, Grimes DA, Stubblefield PG, Creinin MD (eds.). Management of unintended and abnormal pregnancy: comprehensive abortion care. Oxford: Wiley-Blackwell. pp. 111–134. ISBN 1-4051-7696-2.
- ↑ 39.0 39.1 Kapp N, von Hertzen H (2009). "Medical methods to induce abortion in the second trimester". In Paul M, Lichtenberg ES, Borgatta L, Grimes DA, Stubblefield PG, Creinin MD (eds.). Management of unintended and abnormal pregnancy: comprehensive abortion care. Oxford: Wiley-Blackwell. pp. 178–192. ISBN 1-4051-7696-2.
- ↑ Wildschut, H; Both, MI; Medema, S; Thomee, E; Wildhagen, MF; Kapp, N (19 January 2011). "Medical methods for mid-trimester termination of pregnancy.". Cochrane database of systematic reviews (Online) (1): CD005216. doi:10.1002/14651858.CD005216.pub2. PMID 21249669.
- ↑ 41.0 41.1 WHO Department of Reproductive Health and Research (23 November 2006). Frequently asked clinical questions about medical abortion (PDF). Geneva: World Health Organization. ISBN 92-4-159484-5. Retrieved 22 November 2011.
- ↑ Fjerstad M, Sivin I, Lichtenberg ES, Trussell J, Cleland K, Cullins V (September 2009). "Effectiveness of medical abortion with mifepristone and buccal misoprostol through 59 gestational days". Contraception 80 (3): 282–286. doi:10.1016/j.contraception.2009.03.010. PMC 3766037. PMID 19698822. The regimen (200 mg of mifepristone, followed 24–48 hours later by 800 mcg of vaginal misoprostol) previously used by Planned Parenthood clinics in the United States from 2001 to March 2006 was 98.5% effective through 63 days gestation—with an ongoing pregnancy rate of about 0.5%, and an additional 1% of patients having uterine evacuation for various reasons, including problematic bleeding, persistent gestational sac, clinician judgment or patient request. The regimen (200 mg of mifepristone, followed 24–48 hours later by 800 mcg of buccal misoprostol) currently used by Planned Parenthood clinics in the United States since April 2006 is 98.3% effective through 59 days gestation.
- ↑ Holmquist S, Gilliam M (2008). "Induced abortion". In Gibbs RS, Karlan BY, Haney AF, Nygaard I (eds.). Danforth's obstetrics and gynecology (10th ed.). Philadelphia: Lippincott Williams & Wilkins. pp. 586–603. ISBN 978-0-7817-6937-2.
- ↑ "Abortion statistics, England and Wales: 2010". London: Department of Health, United Kingdom. 24 May 2011. Retrieved 22 November 2011.
- ↑ "Abortion statistics, year ending 31 December 2010" (PDF). Edinburgh: ISD, NHS Scotland. 31 May 2011. Retrieved 22 November 2011.
- ↑ Vilain A, Mouquet M-C (22 June 2011). "Voluntary terminations of pregnancies in 2008 and 2009" (PDF). Paris: DREES, Ministry of Health, France. Retrieved 22 November 2011.
- ↑ . (5 July 2011). "Abortions in Switzerland 2010". Neuchâtel: Office of Federal Statistics, Switzerland. Retrieved 22 November 2011.
- ↑ Gissler M, Heino A (21 February 2011). "Induced abortions in the Nordic countries 2009" (PDF). Helsinki: National Institute for Health and Welfare, Finland. Retrieved 22 November 2011.
- ↑ Jones RK, Kooistra K (March 2011). "Abortion incidence and access to services in the United States, 2008" (PDF). Perspect Sex Reprod Health 43 (1): 41–50. doi:10.1363/4304111. PMID 21388504. Retrieved 22 November 2011.
- ↑ 50.0 50.1 50.2 Templeton, A.; Grimes, D. A. (2011). "A Request for Abortion". New England Journal of Medicine 365 (23): 2198–2204. doi:10.1056/NEJMcp1103639.
- ↑ Hammond C, Chasen ST (2009). "Dilation and evacuation". In Paul M, Lichtenberg ES, Borgatta L, Grimes DA, Stubblefield PG, Creinin MD (eds.). Management of unintended and abnormal pregnancy: comprehensive abortion care. Oxford: Wiley-Blackwell. pp. 178–192. ISBN 1-4051-7696-2.
- ↑ Healthwise (2004). "Manual and vacuum aspiration for abortion". WebMD. Archived from the original on 28 October 2008. Retrieved 5 December 2008.
- ↑ World Health Organization (2003). "Dilatation and curettage". Managing Complications in Pregnancy and Childbirth: A Guide for Midwives and Doctors. Geneva: World Health Organization. ISBN 978-92-4-154587-7. OCLC 181845530. Retrieved 5 December 2008.
- ↑ McGee, Glenn; Jon F. Merz. "Abortion". Encarta. Microsoft. Archived from the original on 31 October 2009. Retrieved 5 December 2008.
- ↑ Riddle, John M. (1997). Eve's herbs: a history of contraception and abortion in the West. Cambridge, Massachusetts: Harvard University Press. ISBN 978-0-674-27024-4. OCLC 36126503.
- ↑ Ciganda C, Laborde A (2003). "Herbal infusions used for induced abortion". J. Toxicol. Clin. Toxicol. 41 (3): 235–239. doi:10.1081/CLT-120021104. PMID 12807304.
- ↑ Smith JP (1998). "Risky choices: The dangers of teens using self-induced abortion attempts". Journal of Pediatric Health Care 12 (3): 147–151. doi:10.1016/S0891-5245(98)90245-0. PMID 9652283.
- ↑ 58.0 58.1 58.2 58.3 Potts, M.; Graff, M.; Taing, J. (2007). "Thousand-year-old depictions of massage abortion". Journal of Family Planning and Reproductive Health Care 33 (4): 233–234. doi:10.1783/147118907782101904. PMID 17925100.
- ↑ Thapa, S. R.; Rimal, D.; Preston, J. (2006). "Self induction of abortion with instrumentation". Australian Family Physician 35 (9): 697–698. PMID 16969439.
- ↑ "The Prevention and Management of Unsafe Abortion" (PDF). World Health Organization. April 1995. Archived (PDF) from the original on 30 May 2010. Retrieved 1 June 2010.
- ↑ Grimes, DA; Creinin, MD (2004). "Induced abortion: an overview for internists". Ann. Intern. Med. 140 (8): 620–6. doi:10.7326/0003-4819-140-8-200404200-00009. PMID 15096333.
- ↑ Raymond, E. G.; Grimes, D. A. (2012). "The Comparative Safety of Legal Induced Abortion and Childbirth in the United States". Obstetrics & Gynecology 119 (2, Part 1): 215–219. doi:10.1097/AOG.0b013e31823fe923. PMID 22270271.
- ↑ Grimes DA (January 2006). "Estimation of pregnancy-related mortality risk by pregnancy outcome, United States, 1991 to 1999". Am. J. Obstet. Gynecol. 194 (1): 92–4. doi:10.1016/j.ajog.2005.06.070. PMID 16389015.
- ↑ Bartlett LA; Berg CJ; Shulman HB et al. (April 2004). "Risk factors for legal induced abortion-related mortality in the United States". Obstet Gynecol 103 (4): 729–37. doi:10.1097/01.AOG.0000116260.81570.60. PMID 15051566.
- ↑ Trupin, Suzanne (27 May 2010). "Elective Abortion". eMedicine. Retrieved 1 June 2010.
At every gestational age, elective abortion is safer for the mother than carrying a pregnancy to term.
- ↑ Pittman, Genevra (23 January 2012). "Abortion safer than giving birth: study". Reuters. Retrieved 4 February 2012.
- ↑ Westfall JM, Sophocles A, Burggraf H, Ellis S (1998). "Manual vacuum aspiration for first-trimester abortion". Arch Fam Med 7 (6): 559–62. doi:10.1001/archfami.7.6.559. PMID 9821831.
- ↑ ACOG Committee on Practice Bulletins—Gynecology (May 2009). "ACOG practice bulletin No. 104: antibiotic prophylaxis for gynecologic procedures". Obstet Gynecol 113 (5): 1180–9. doi:10.1097/AOG.0b013e3181a6d011. PMID 19384149.
- ↑ Sawaya GF, Grady D, Kerlikowske K, Grimes DA (May 1996). "Antibiotics at the time of induced abortion: the case for universal prophylaxis based on a meta-analysis". Obstet Gynecol 87 (5 Pt 2): 884–90. PMID 8677129.
- ↑ Grossman D (3 September 2004). "Medical methods for first trimester abortion: RHL commentary". Reproductive Health Library. Geneva: World Health Organization. Retrieved 22 November 2011.
- ↑ Chien P, Thomson M (15 December 2006). "Medical versus surgical methods for first trimester termination of pregnancy: RHL commentary". Reproductive Health Library. Geneva: World Health Organization. Archived from the original on 17 May 2010. Retrieved 1 June 2010.
- ↑ 72.0 72.1 Jasen P (October 2005). "Breast cancer and the politics of abortion in the United States". Med Hist 49 (4): 423–44. doi:10.1017/S0025727300009145. PMC 1251638. PMID 16562329.
- ↑ Position statements of major medical bodies on abortion and breast cancer include:
- World Health Organization: "Induced abortion does not increase breast cancer risk (Fact sheet N°240)". World Health Organization. Archived from the original on 13 February 2011. Retrieved 6 January 2011.
- National Cancer Institute: "Abortion, Miscarriage, and Breast Cancer Risk". National Cancer Institute. Archived from the original on 21 December 2010. Retrieved 11 January 2011.
- American Cancer Society: "Is Abortion Linked to Breast Cancer?". American Cancer Society. 23 September 2010. Archived from the original on 5 June 2011. Retrieved 20 June 2011.
At this time, the scientific evidence does not support the notion that abortion of any kind raises the risk of breast cancer.
- Royal College of Obstetricians and Gynaecologists: "The Care of Women Requesting Induced Abortion" (PDF). Royal College of Obstetricians and Gynaecologists. p. 9. Retrieved 29 June 2008.
Induced abortion is not associated with an increase in breast cancer risk.
- American Congress of Obstetricians and Gynecologists: "ACOG Finds No Link Between Abortion and Breast Cancer Risk". American Congress of Obstetricians and Gynecologists. 31 July 2003. Archived from the original on 2 January 2011. Retrieved 11 January 2011.
- ↑ Cockburn, Jayne; Pawson, Michael E. (2007). Psychological Challenges to Obstetrics and Gynecology: The Clinical Management. Springer. p. 243. ISBN 978-1-84628-807-4.
- ↑ "APA Task Force Finds Single Abortion Not a Threat to Women's Mental Health" (Press release). American Psychological Association. 12 August 2008. Retrieved 7 September 2011.
- ↑ "Report of the APA Task Force on Mental Health and Abortion" (PDF). Washington, DC: American Psychological Association. 13 August 2008.
- ↑ Steinberg, J. R. (2011). "Later Abortions and Mental Health: Psychological Experiences of Women Having Later Abortions—A Critical Review of Research". Women's Health Issues 21 (3): S44–S48. doi:10.1016/j.whi.2011.02.002. PMID 21530839.
- ↑ Cohen, Susan A. (Summer 2006). "Abortion and Mental Health: Myths and Realities". Guttmacher Policy Review. Retrieved 12 April 2015.
- ↑ Okonofua, F. (2006). "Abortion and maternal mortality in the developing world" (PDF). Journal of Obstetrics and Gynaecology Canada 28 (11): 974–979. PMID 17169222.
- ↑ Haddad, LB.; Nour, NM. (2009). "Unsafe abortion: unnecessary maternal mortality". Rev Obstet Gynecol 2 (2): 122–6. PMC 2709326. PMID 19609407.
- ↑ Lozano, R (15 December 2012). "Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010.". Lancet 380 (9859): 2095–128. doi:10.1016/S0140-6736(12)61728-0. PMID 23245604.
- ↑ Darney, Leon Speroff, Philip D. (2010). A clinical guide for contraception (5th ed. ed.). Philadelphia, Pa.: Lippincott Williams & Wilkins. p. 406. ISBN 1-60831-610-6.
- ↑ World Health Organisation (2011). Unsafe abortion: global and regional estimates of the incidence of unsafe abortion and associated mortality in 2008 (PDF) (6th ed.). World Health Organisation. p. 27. ISBN 978-92-4-150111-8.
- ↑ 84.0 84.1 Berer M (2000). "Making abortions safe: a matter of good public health policy and practice". Bull. World Health Organ. 78 (5): 580–92. PMC 2560758. PMID 10859852.
- ↑ Sedgh G, Henshaw S, Singh S, Ahman E, Shah IH (2007). "Induced abortion: estimated rates and trends worldwide". Lancet 370 (9595): 1338–45. doi:10.1016/S0140-6736(07)61575-X. PMID 17933648.
- ↑ 86.0 86.1 "Unsafe abortion: Global and regional estimates of the incidence of unsafe abortion and associated mortality in 2003" (PDF). World Health Organization. 2007. Archived (PDF) from the original on 16 February 2011. Retrieved 7 March 2011.
- ↑ Berer M (November 2004). "National laws and unsafe abortion: the parameters of change". Reprod Health Matters 12 (24 Suppl): 1–8. doi:10.1016/S0968-8080(04)24024-1. PMID 15938152.
- ↑ Jewkes R, Rees H, Dickson K, Brown H, Levin J (March 2005). "The impact of age on the epidemiology of incomplete abortions in South Africa after legislative change". BJOG 112 (3): 355–9. doi:10.1111/j.1471-0528.2004.00422.x. PMID 15713153.
- ↑ Bateman C (December 2007). "Maternal mortalities 90% down as legal TOPs more than triple". S. Afr. Med. J. 97 (12): 1238–42. PMID 18264602.
- ↑ "Facts on Investing in Family Planning and Maternal and Newborn Health" (PDF). Guttmacher Institute. 2010. Retrieved 24 May 2012.
- ↑ Maclean, Gaynor (2005). "XI. Dimension, Dynamics and Diversity: A 3D Approach to Appraising Global Maternal and Neonatal Health Initiatives". In Balin, Randell E. Trends in Midwifery Research. Nova Publishers. pp. 299–300. ISBN 978-1-59454-477-4.
- ↑ Salter, C., Johnson, H.B., and Hengen, N. (1997). "Care for Postabortion Complications: Saving Women's Lives". Population Reports (Johns Hopkins School of Public Health) 25 (1). Archived from the original on 1 September 2011.
- ↑ UNICEF, United Nations Population Fund, WHO, World Bank (2010). "Packages of interventions: Family planning, safe abortion care, maternal, newborn and child health". Retrieved 31 December 2010.
- ↑ Shah I, Ahman E (December 2009). "Unsafe abortion: global and regional incidence, trends, consequences, and challenges". J Obstet Gynaecol Can 31 (12): 1149–58. PMID 20085681.
However, a woman's chance of having an abortion is similar whether she lives in a developed or a developing region: in 2003 the rates were 26 abortions per 1000 women aged 15 to 44 in developed areas and 29 per 1000 in developing areas. The main difference is in safety, with abortion being safe and easily accessible in developed countries and generally restricted and unsafe in most developing countries
- ↑ Rosenthal, Elizabeth (12 October 2007). "Legal or Not, Abortion Rates Compare". The New York Times. Retrieved 18 July 2011.
- ↑ "Facts on Investing in Family Planning and Maternal and Newborn Health" (PDF). Guttmacher Institute. November 2010. Retrieved 24 October 2011.
- ↑ Sedgh, G.; Singh, S.; Henshaw, S. K.; Bankole, A. (2011). "Legal Abortion Worldwide in 2008: Levels and Recent Trends". Perspectives on Sexual and Reproductive Health 43 (3): 188–198. doi:10.1363/4318811. PMID 21884387.
- ↑ National Institute of Statistics, Romanian Statistical Yearbook, chapter 2, page 62, 2011
- ↑ Strauss, L. T.; Gamble, S. B.; Parker, W. Y.; Cook, D. A.; Zane, S. B.; Hamdan, S.; Centers for Disease Control Prevention (2006). "Abortion surveillance—United States, 2003". Morbidity and Mortality Weekly Report Surveillance Summaries 55 (SS11): 1–32. PMID 17119534.
- ↑ 100.0 100.1 100.2 "The Limitations of U.S. Statistics on Abortion". Issues in Brief. New York: The Guttmacher Institute. 1997. Archived from the original on 4 April 2012.
- ↑ Finer, L. B.; Henshaw, S. K. (2003). "Abortion Incidence and Services in the United States in 2000". Perspectives on Sexual and Reproductive Health 35 (1): 6–15. doi:10.1363/3500603. PMID 12602752.
- ↑ Department of Health (2007). "Abortion statistics, England and Wales: 2006". Retrieved 12 October 2007.
- ↑ Cheng, Linan (November 1, 2008). "Surgical versus medical methods for second-trimester induced abortion: RHL commentary". The WHO Reproductive Health Library. Geneva: World Health Organization. Retrieved February 10, 2009. commentary on:
Lohr, Patricia A.; Hayes, Jennifer L.; Gemzell-Danielsson, Kristina (January 23, 2008). "Surgical versus medical methods for second trimester abortion". Cochrane Database of Systematic Reviews (1): CD006714. doi:10.1002/14651858.CD006714.pub2. PMID 18254113. - ↑ 104.0 104.1 104.2 Bankole, Akinrinola; Singh, Susheela; Haas, Taylor (1998). "Reasons Why Women Have Induced Abortions: Evidence from 27 Countries". International Family Planning Perspectives 24 (3): 117–127; 152. doi:10.2307/3038208.
- ↑ Finer, L. B.; Frohwirth, L. F.; Dauphinee, L. A.; Singh, S.; Moore, A. M. (2005). "Reasons U.S. Women Have Abortions: Quantitative and Qualitative Perspectives". Perspectives on Sexual and Reproductive Health 37 (3): 110–118. doi:10.1111/j.1931-2393.2005.tb00045.x. PMID 16150658.
- ↑ "Nuremberg and the Crime of Abortion". U. Toledo. L. Rev. 42: 283. Retrieved 12 July 2014.
- ↑ Oster, Emily (September 2005). "Explaining Asia's "Missing Women": A New Look at the Data – Comment" (PDF). Population and Development Review 31 (3): 529, 535. doi:10.1111/j.1728-4457.2005.00082.x. Retrieved 19 May 2009.
- ↑ Jones, R. K.; Darroch, J. E.; Henshaw, S. K. (2002). "Contraceptive Use Among U.S. Women Having Abortions in 2000–2001" (PDF). Perspectives on Sexual and Reproductive Health 34 (6): 294–303. doi:10.2307/3097748. PMID 12558092.
- ↑ Cohen, SA (2008). "Abortion and Women of Color: The Bigger Picture". Guttmacher Policy Review 11 (3).
- ↑ George J. Annas and Sherman Elias. Legal and Ethical Issues in Obstetrical Practice. Chapter 54 in Obstetrics: Normal and Problem Pregnancies, 6th edition. Eds. Steven G. Gabbe, et al. 2012 Saunders, an imprint of Elsevier. ISBN 978-1-4377-1935-2
- ↑ Doan 2007, p. 57.
- ↑ 112.0 112.1 Weisz, B; Schiff, E; Lishner, M (2001). "Cancer in pregnancy: maternal and fetal implications" (PDF). Hum Reprod Update 7 (4): 384–393. doi:10.1093/humupd/7.4.384. PMID 11476351.
- ↑ Mayr, NA; Wen, BC; CB (1998). "Radiation therapy during pregnancy". Obstet Gynecol Clin North Am. 25 (2): 301–21. PMID 9629572.
- ↑ Fenig E, Mishaeli M, Kalish Y, Lishner M (2001). "Pregnancy and radiation.". Cancer Treat Rev 27 (1): 1–7. doi:10.1053/ctrv.2000.0193. PMID 11237773.
- ↑ Li WW, Yau TN, Leung CW, Pong WM, Chan MY (2009). "Large-cell neuroendocrine carcinoma of the uterine cervix complicating pregnancy". Hong Kong Med J 15 (1): 69–72. PMID 19197101.
- ↑ Mould R (1996). Mould's Medical Anecdotes. CRC Press. p. 406. ISBN 978-0-85274-119-1.
- ↑ Miles, Steven (2005). The Hippocratic Oath and the Ethics of Medicine. Oxford University Press. ISBN 978-0-19-518820-2.
- ↑ Carrick, Paul (2001). Medical Ethics in the Ancient World. Georgetown University Press. ISBN 978-0-87840-849-8.
- ↑ Rackham, H. (1944). "Aristotle, Politics". Harvard University Press. Retrieved 21 June 2011.
- ↑ Brind'Amour, Katherine (2007). "Effraenatam". Embryo Project Encyclopedia. Arizona State University. Archived from the original on 1 February 2012.
- ↑ "Religions – Islam: Abortion". BBC. Retrieved 10 December 2011.
- ↑ Dabash, Rasha; Roudi-Fahimi, Farzaneh (2008). "Abortion in the Middle East and North Africa" (PDF). Population Research Bureau. Archived (PDF) from the original on 8 July 2011.
- ↑ "Abortion Law, History & Religion". Childbirth By Choice Trust. Archived from the original on 8 February 2008. Retrieved 23 March 2008.
- ↑ For sources describing abortion policy in Nazi Germany, see:
- Friedlander, Henry (1995). The origins of Nazi genocide: from euthanasia to the final solution. Chapel Hill: University of North Carolina Press. p. 30. ISBN 978-0-8078-4675-9. OCLC 60191622.
- Proctor, Robert (1988). Racial Hygiene: Medicine Under the Nazis. Cambridge, Massachusetts: Harvard University Press. pp. 122, 123 and 366. ISBN 978-0-674-74578-0. OCLC 20760638.
- Arnot, Margaret L.; Cornelie Usborne (1999). Gender and Crime in Modern Europe. New York: Routledge. p. 231. ISBN 978-1-85728-745-5. OCLC 186748539.
- DiMeglio, Peter M. (1999). "Germany 1933–1945 (National Socialism)". In Helen Tierney. Women's studies encyclopedia. Westport, Connecticut: Greenwood Press. p. 589. ISBN 978-0-313-31072-0. OCLC 38504469.
- ↑ Smith, Richard Norton On His Own Terms: A Life of Nelson Rockefeller pages 560-561
- ↑ "World Abortion Policies 2013" (PDF). United Nations Department of Economic and Social Affairs, Population Division. Retrieved 31 July 2013.
- ↑ World Abortion Policies 2007, United Nations, Department of Economic and Social Affairs, Population Division.
- ↑ Theodore J. Joyce, Stanley K. Henshaw, Amanda Dennis, Lawrence B. Finer and Kelly Blanchard (April 2009). "The Impact of State Mandatory Counseling and Waiting Period Laws on Abortion: A Literature Review". Guttmacher Institute. Archived from the original (PDF) on 14 January 2011. Retrieved 31 December 2010.
- ↑ Restivo, Sal P., ed. (2005). Science, Technology, and Society: An Encyclopedia. Oxford University Press. p. 2. ISBN 9780195141931.
- ↑ "European delegation visits Nicaragua to examine effects of abortion ban". Ipas. 26 November 2007. Archived from the original on 17 April 2008. Retrieved 15 June 2009.
More than 82 maternal deaths had been registered in Nicaragua since the change. During this same period, indirect obstetric deaths, or deaths caused by illnesses aggravated by the normal effects of pregnancy and not due to direct obstetric causes, have doubled.
- ↑ "Nicaragua: "The Women's Movement Is in Opposition"". Montevideo: Inside Costa Rica. IPS. 28 June 2008.
- ↑ "Surgical Abortion: History and Overview". National Abortion Federation. Archived from the original on 22 September 2006. Retrieved 4 September 2006.
- ↑ Nations MK, Misago C, Fonseca W, Correia LL, Campbell OM. (June 1997). "Women's hidden transcripts about abortion in Brazil". Soc Sci Med 44 (12): 1833–45. doi:10.1016/s0277-9536(96)00293-6. PMID 9194245.
Two folk medical conditions, "delayed" (atrasada) and "suspended" (suspendida) menstruation, are described as perceived by poor Brazilian women in Northeast Brazil. Culturally prescribed methods to "regulate" these conditions and provoke menstrual bleeding are also described ...
- ↑ Henshaw, S. K. (1991). "The Accessibility of Abortion Services in the United States". Family Planning Perspectives 23 (6): 246–263. doi:10.2307/2135775.
- ↑ Marcy Bloom (25 February 2008). "Need Abortion, Will Travel". RH Reality Check. Retrieved 15 June 2009.
- ↑ Ross, Jen (12 September 2006). "In Chile, free morning-after pills to teens". The Christian Science Monitor. Retrieved 7 December 2006.
- ↑ Gallardoi, Eduardo (26 September 2006). "Morning-After Pill Causes Furor in Chile". The Washington Post. Retrieved 7 December 2006.
- ↑ Banister, Judith. (16 March 1999). Son Preference in Asia – Report of a Symposium. Retrieved 12 January 2006.
- ↑ Reaney, Patricia. "Selective abortion blamed for India's missing girls". Reuters. Archived from the original on 20 February 2006. Retrieved 3 December 2008.
- ↑ Sudha, S.; Rajan, S. Irudaya (July 1999). "Female Demographic Disadvantage in India 1981–1991: Sex Selective Abortions and Female Infanticide". Development and Change 30 (3): 585–618. doi:10.1111/1467-7660.00130. PMID 20162850. Archived from the original on 1 January 2003. Retrieved 3 December 2008.
- ↑ "Sex Selection & Abortion: India". Library of Congress. 4 April 2011. Retrieved 18 July 2011.
- ↑ "China Bans Sex-selection Abortion." (22 March 2002). Xinhua News Agency.'.' Retrieved 12 January 2006.
- ↑ Graham, Maureen J.; Larsen; Xu (June 1998). "Son Preference in Anhui Province, China". International Family Planning Perspectives 24 (2): 72–77. doi:10.2307/2991929. Archived from the original on 21 October 2011.
- ↑ 144.0 144.1 "Preventing gender-biased sex selection" (PDF). UNFPA. Retrieved 1 November 2011.
- ↑ "Prenatal sex selection" (PDF). PACE. Retrieved 27 April November 2012. Check date values in:
|accessdate=(help) - ↑ Smith, G. Davidson (Tim) (1998). "Single Issue Terrorism Commentary". Canadian Security Intelligence Service. Archived from the original on 15 October 2007. Retrieved 1 September 2011.
- ↑ Wilson, M.; Lynxwiler, J. (1988). "Abortion clinic violence as terrorism". Studies in Conflict & Terrorism 11 (4): 263–273. doi:10.1080/10576108808435717.
- ↑ "The Death of Dr. Gunn". New York Times. 12 March 1993.
- ↑ "Incidence of Violence & Disruption Against Abortion Providers in the U.S. & Canada" (PDF). National Abortion Federation. 2009. Retrieved 9 February 2010.
- ↑ Borger, Julian (3 February 1999). "The bomber under siege". The Guardian (London).
- ↑ 151.0 151.1 Alesha E. Doan (2007). Opposition and Intimidation:The abortion wars and strategies of political harassment. University of Michigan. p. 2.
- ↑ Spencer, James B. (1908). Sheep Husbandry in Canada. p. 114. OCLC 798508694.
- ↑ "Beef cattle and Beef production: Management and Husbandry of Beef Cattle". Encyclopaedia of New Zealand. 1966.
- ↑ Myers, Brandon; Beckett, Jonathon (2001). "Pine needle abortion". Animal Health Care and Maintenance (PDF). Tucson, AZ: Arizona Cooperative Extension, University of Arizona. pp. 47–50. Retrieved 10 April 2013.
- ↑ Kim, Ill-Hwa; Choi, Kyung-Chul; An, Beum-Soo; Choi, In-Gyu; Kim, Byung-Ki; Oh, Young-Kyoon; Jeung, Eui-Bae (2003). "Effect on abortion of feeding Korean pine needles to pregnant Korean native cows". Canadian Journal of Veterinary Research (Canadian Veterinary Medical Association) 67 (3): 194–197. PMC 227052. PMID 12889725.
- ↑ Overton, Rebecca (March 2003). "By a Hair" (PDF). Paint Horse Journal. Retrieved 19 December 2012.
- ↑ "Herpesvirus in dog pups". petMD. Retrieved 18 December 2012.
- ↑ "Spaying Pregnant Females". Carol's Ferals. Retrieved 17 December 2012.
- ↑ Coates, Jennifer (7 May 2007). "Feline abortion: often an unnerving necessity". petMD. Retrieved 18 December 2012.
- ↑ Khuly, Patty (1 April 2011). "Feline abortion: often an unnerving necessity (Part 2)". petMD. Retrieved 18 December 2012.
- ↑ Schwagmeyer, P. L. (1979). "The Bruce Effect: An Evaluation of Male/Female Advantages". The American Naturalist 114 (6): 932–938. doi:10.1086/283541. JSTOR 2460564.
- ↑ McKinnon, Angus O.; Voss, James L. (1993). Equine Reproduction. Wiley-Blackwell. p. 563. ISBN 0-8121-1427-2.
- ↑ Berger, Joel W; Vuletić, L; Boberić, J; Milosavljević, A; Dilparić, S; Tomin, R; Naumović, P (5 May 1983). "Induced abortion and social factors in wild horses". Nature 303 (5912): 59–61. doi:10.1038/303059a0. PMID 6682487.
- ↑ Pluháček, Jan; Bartos, L (2000). "Male infanticide in captive plains zebra, Equus burchelli" (PDF). Animal Behaviour 59 (4): 689–694. doi:10.1006/anbe.1999.1371. PMID 10792924.
- ↑ Pluháček, Jan (2005). "Further evidence for male infanticide and feticide in captive plains zebra, Equus burchelli" (PDF). Folia Zool. 54 (3): 258–262.
- ↑ Kirkpatrick, J. F.; Turner, J. W. (1991). "Changes in Herd Stallions among Feral Horse Bands and the Absence of Forced Copulation and Induced Abortion". Behavioral Ecology and Sociobiology 29 (3): 217–219. doi:10.1007/BF00166404. JSTOR 4600608.
- ↑ Agoramoorthy, G.; Mohnot, S. M.; Sommer, V.; Srivastava, A. (1988). "Abortions in free ranging Hanuman langurs (Presbytis entellus) – a male induced strategy?". Human Evolution 3 (4): 297–308. doi:10.1007/BF02435859.
Notes
- ↑ 1.0 1.1 Definitions of abortion, as with many words, vary from source to source. Language used to define abortion often reflects societal and political opinions (not only scientific knowledge). The following is a partial list of definitions as stated by obstetrics and gynecology (OB/GYN) textbooks, dictionaries, and other sources:
- Major OB/GYN textbooks
- The National Center for Health Statistics defines an "abortus" as "[a] fetus or embryo removed or expelled from the uterus during the first half of gestation—20 weeks or less, or in the absence of accurate dating criteria, born weighing < 500 g." They also define "birth" as "[t]he complete expulsion or extraction from the mother of a fetus after 20 weeks' gestation. ... in the absence of accurate dating criteria, fetuses weighing <500 g are usually not considered as births, but rather are termed abortuses for purposes of vital statistics." Cunningham, FG; Leveno, KJ; Bloom, SL et al., eds. (2010). "1. Overview of Obstetrics". Williams Obstetrics (23 ed.). McGraw-Hill Medical. ISBN 978-0-07-149701-5.
- "[T]he standard medical definition of abortion [is] termination of a pregnancy when the fetus is not viable". Annas, George J.; Elias, Sherman (2007). "51. Legal and Ethical Issues in Obstetric Practice". In Gabbe, Steven G.; Niebyl, Jennifer R.; Simpson, Joe Leigh. Obstetrics: Normal and Problem Pregnancies (5 ed.). Churchill Livingstone. ISBN 978-0-443-06930-7.
- "Termination of a pregnancy, whether spontaneous or induced." Kottke, Melissa J.; Zieman, Mimi (2008). "33. Management of Abortion". In Rock, John A.; Jones III, Howard W. TeLinde's Operative Gynecology (10 ed.). Lippincott Williams & Wilkins. ISBN 978-0-7817-7234-1.
- Other OB/GYN textbooks
- "Termination of pregnancy before 20 weeks' gestation calculated from date of onset of last menses. An alternative definition is delivery of a fetus with a weight of less than 500 g. If abortion occurs before 12 weeks' gestation, it is called early; from 12 to 20 weeks it is called late." Katz, Vern L. (2007). "16. Spontaneous and Recurrent Abortion – Etiology, Diagnosis, Treatment". In Katz, Vern L.; Lentz, Gretchen M.; Lobo, Rogerio A. et al. Katz: Comprehensive Gynecology (5 ed.). Mosby. ISBN 978-0-323-02951-3.
- "Abortion is the spontaneous or induced termination of pregnancy before fetal viability. Because popular use of the word abortion implies a deliberate pregnancy termination, some prefer the word miscarriage to refer to spontaneous fetal loss before viability ... The National Center for Health Statistics, the Centers for Disease Control and Prevention (CDC), and the World Health Organization (WHO) define abortion as pregnancy termination prior to 20 weeks' gestation or a fetus born weighing less than 500 g. Despite this, definitions vary widely according to state laws." Schorge, John O.; Schaffer, Joseph I.; Halvorson, Lisa M.; Hoffman, Barbara L.; Bradshaw, Karen D.; Cunningham, F. Gary, eds. (2008). "6. First-Trimester Abortion". Williams Gynecology (1 ed.). McGraw-Hill Medical. ISBN 978-0-07-147257-9.
- Major medical dictionaries
- "The spontaneous or induced termination of pregnancy before the fetus reaches a viable age." "Taber's Medical Dictionary: abortion". Taber's Cyclopedic Medical Dictionary. F.A. Davis. Archived from the original on 14 June 2011. Retrieved 14 June 2011.
- "Expulsion from the uterus an embryo or fetus prior to the stage of viability (20 weeks' gestation or fetal weight <500g). A distinction made between [abortion] and premature birth: premature infants are those born after the stage of viability but prior to 37 weeks." Stedman's Medical Dictionary (27 ed.). Lippincott Williams & Wilkins. ISBN 0-683-40008-8.
- "[P]remature expulsion from the uterus of the products of conception, either the embryo or a nonviable fetus." Dorland's Illustrated Medical Dictionary (31 ed.). Saunders. 2007. ISBN 978-1-4160-2364-7.
- Other medical dictionaries
- "[T]he termination of a pregnancy after, accompanied by, resulting in, or closely followed by the death of the embryo or fetus". "Medical Dictionary". Merriam-Webster's Medical Dictionary. Springfield, Mass.: Merriam-Webster. Archived from the original on 15 June 2011. Retrieved 15 June 2011.
- "Induced termination of pregnancy, involving destruction of the embryo or fetus." "abortion." The American Heritage Science Dictionary. Boston: Houghton Mifflin. 2005. ISBN 978-0-618-45504-1.
- "Interruption of pregnancy before the fetus has attained a stage of viability, usually before the 24th gestational week." "abortion." Cambridge Dictionary of Human Biology and Evolution. Cambridge; New York: Cambridge University Press. 2005. OCLC 54374716.
- "[A] spontaneous or deliberate ending of pregnancy before the fetus can be expected to survive." "abortion." Mosby's Emergency Dictionary. Philadelphia: Elsevier Health Sciences. 1998. OCLC 37553784.
- "[A] situation where a fetus leaves the uterus before it is fully developed, especially during the first 28 weeks of pregnancy, or a procedure which causes this to happen ... [T]o have an abortion to have an operation to make a fetus leave the uterus during the first period of pregnancy." ""abortion"". Dictionary of Medical Terms. London: A & C Black. 2005. OCLC 55634250.
- "1. Induced termination of a pregnancy with destruction of the fetus or embryo; therapeutic abortion. 2. Spontaneous abortion." The American Heritage Medical Dictionary (reprint ed.). Houghton Mifflin. 2008. p. 2. ISBN 0-618-94725-6. OCLC 608212441.
- "Although the term abortion is generic and implies a premature termination of pregnancy for any reason, the lay public better understands the word 'miscarriage' for involuntary fetal loss or fetal wastage." The Dictionary of Modern Medicine. Parthenon Publishing. 1992. p. 3. ISBN 1-85070-321-3.
- "The termination of pregnancy or premature expulsion of the products of conception by any means, usually before fetal viability." Churchill's Medical Dictionary. Churchill Livingstone. 1989. p. 3. ISBN 0-443-08691-5.
- Bibliographies
- "An abortion refers to the termination of a pregnancy. It can be induced (see Definitions, Terminology, and Reference Resources) through a pharmacological or a surgical procedure, or it may be spontaneous (also called miscarriage)." "Definitions of abortion vary across and within countries as well as among different institutions. Language used to refer to abortion often also reflects societal and political opinions and not only scientific knowledge (Grimes and Gretchen 2010). Popular use of the word abortion implies a deliberate pregnancy termination, whereas a miscarriage is used to refer to spontaneous fetal loss when the fetus is not viable (i.e., not yet unable to survive independently outside the womb)." Kulczycki, Andrzej. "Abortion". Oxford Bibliographies. Retrieved 9 April 2014.
- Major English dictionaries (general-purpose)
- "1. a. The expulsion or removal from the womb of a developing embryo or fetus, spec. (Med.) in the period before it is capable of independent survival, occurring as a result either of natural causes (more fully spontaneous abortion) or of a deliberate act (more fully induced abortion); the early or premature termination of pregnancy with loss of the fetus; an instance of this." "abortion, n.". Oxford English Dictionary (Third ed.). Oxford University Press. September 2009; online version September 2011. Check date values in:
|date=(help) - "[A]n operation or other procedure to terminate pregnancy before the fetus is viable" or "[T]he premature termination of pregnancy by spontaneous or induced expulsion of a nonviable fetus from the uterus". "abortion". Collins English Dictionary – Complete & Unabridged 11th Edition. HarperCollins Publishers. Retrieved 7 October 2012.
- "[T]he removal of an embryo or fetus from the uterus in order to end a pregnancy" or "[A]ny of various surgical methods for terminating a pregnancy, especially during the first six months." "abortion". Dictionary.com Unabridged. Random House, Inc. 27 June 2011.
- "1. medicine the removal of an embryo or fetus from the uterus before it is sufficiently developed to survive independently, deliberately induced by the use of drugs or by surgical procedures. Also called termination or induced abortion. 2. medicine the spontaneous expulsion of an embryo or fetus from the uterus before it is sufficiently developed to survive independently. Also called miscarriage, spontaneous abortion." Chambers 21st Century Dictionary. London: Chambers Harrap, 2001.
- "a medical operation to end a pregnancy so that the baby is not born alive". Longman Dictionary of Contemporary English, online edition.
- Other dictionaries
- "The deliberate termination of a pregnancy, usually before the embryo or fetus is capable of independent life." The American Heritage New Dictionary of Cultural Literacy (3rd ed.). Houghton Mifflin Company. 2005.
- "A term that, in philosophy, theology, and social debates, often means the deliberate termination of pregnancy before the fetus is able to survive outside the uterus. However, participants in these debates sometimes use the term abortion simply to mean the termination of pregnancy before birth, regardless of whether the fetus is viable or not." "abortion." Dictionary of World Philosophy. London: Routledge, 2001.
- "1. An artificially induced termination of a pregnancy for the purpose of destroying an embryo or fetus. 2. The spontaneous expulsion of an embryo or fetus before viability;" Garner, Bryan A. (June 2009). Black's Law Dictionary (9th ed.). Thomson West. ISBN 978-0-314-19949-2.
- Encyclopedias
- "[T]he expulsion of a fetus from the uterus before it has reached the stage of viability (in human beings, usually about the 20th week of gestation)." "Abortion (pregnancy)". Encyclopædia Britannica Online. Encyclopædia Britannica. 2011. Archived from the original on 26 June 2011. Retrieved 26 June 2011.
- "Expulsion of the products of conception before the embryo or fetus is viable. Any interruption of human pregnancy prior to the 28th week is known as abortion." "Abortion". The Columbia Encyclopedia. New York: Columbia University Press. 2008.
- "The expulsion or removal of a fetus from the womb before it is capable of independent survival." "Abortion". World Encyclopedia. Oxford University Press. 2008.
- "[Abortion] is commonly misunderstood outside medical circles. In general terms, the word 'abortion' simply means the failure of something to reach fulfilment or maturity. Medically, abortion means loss of the fetus, for any reason, before it is able to survive outside the womb. The term covers accidental or spontaneous ending, or miscarriage, of pregnancy as well as deliberate termination. The terms 'spontaneous abortion' and 'miscarriage' are synonymous and are defined as loss of the fetus before the twenty-eighth week of pregnancy. This definition implies a legal perception of the age at which a fetus can survive out of the womb. With great advances in recent years in the ability to keep very premature babies alive, this definition is in need of revision." "Abortion and miscarriage". The Royal Society of Medicine Health Encyclopedia. London: Bloomsbury Publishing. 2000.
- "Abortion is the intentional removal of a fetus or an embryo from a mother's womb for purposes other than that of either producing a live birth or disposing of a dead embryo." "Abortion". Encyclopedia of Human Rights Issues since 1945 (1 ed.). Santa Barbara, California: Routledge. 1999. ISBN 978-1-57958-166-4.
- Journal articles about terminology
- "Abortion can be performed up to viability; thereafter, according to standard dictionaries, other terms should be used for uterine evacuation. "Late" is an acceptable descriptor for abortion; "late-term" is not. Gestational age should be expressed in completed cardinal days, weeks or months; ordinal numbers (and trimesters) should be avoided. "Intact D&E" should be used instead of the oxymoronic "partial-birth abortion" or the mysterious "D&X." " (internal citations removed) Grimes, DA; Stuart, G (2010). "Abortion jabberwocky: the need for better terminology". Contraception 81 (2): 93–96. doi:10.1016/j.contraception.2009.09.005. PMID 20103443.
- ↑ By 1930, medical procedures in the US had improved for both childbirth and abortion but not equally, and induced abortion in the first trimester had become safer than childbirth. In 1973, Roe vs. Wade acknowledged that abortion in the first trimester was safer than childbirth:
- "The 1970s". Time communication 1940–1989: retrospective. Time, Inc. 1989.
Blackmun was also swayed by the fact that most abortion prohibitions were enacted in the 19th century when the procedure was more dangerous than now.
- Will, George (1990). Suddenly: the American idea abroad and at home, 1986–1990. Free Press. p. 312. ISBN 0-02-934435-2.
- Lewis, J.; Shimabukuro, Jon O. (28 January 2001). "Abortion Law Development: A Brief Overview". Congressional Research Service. Archived from the original on 14 May 2011. Retrieved 1 May 2011.
*Schultz, David Andrew (2002). Encyclopedia of American law. Infobase Publishing. p. 1. ISBN 0-8160-4329-9. - Lahey, Joanna N. (24 September 2009). "Birthing a Nation: Fertility Control Access and the 19th Century Demographic Transition" (PDF; PRELIMINARY VERSION). Colloquium. Pomona College.
- "The 1970s". Time communication 1940–1989: retrospective. Time, Inc. 1989.
External links
- Organization, World Health (2012). Safe abortion: technical and policy guidance for health systems (PDF) (2nd ed. ed.). Geneva: World Health Organization. ISBN 9789241548434.
- Abortion Policies: A Global Review, published by the United Nations
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||