Vacuum mattress

A vacuum mattress, or vacmat, is a medical device used for the immobilisation of patients, especially in case of a vertebra, pelvis or limb trauma (especially for femur trauma). It is also used for manual transportation of patients for short distances (it replaces the stretcher). It was invented by Loed and Haederlé, who called it "shell" mattress (matelas coquille in French).
Operation
It consists of a sealed polymer bag (bigger than an adult human body) that encloses small polystyrene balls, with a valve, straps and handles. It is washable and invisible to X-rays.
When the mattress is under pressure, the balls are free and the mattress can be moulded. Usually, the vacuum mattress is put on a stretcher, the patient is put on the mattress (e.g. with a scoop stretcher), and the sides of the mattress are moulded around the patient. Then, the air is pumped out through the valve and the valve is closed. The atmospheric pressure presses the balls together and the mattress becomes hard and rigid. The straps are then tied to secure the patient.
A sheet is usually put on the vacuum mattress, for three reasons:
- to protect the mattress. The casualty might have broken glass on their clothes or be wearing jewelry that might puncture the mattress,
- to avoid direct contact of the skin with plastic, e.g. for a sweating casualty,
- to help the patient transfer at the emergency room.
Use of the vacuum mattress
The full spine immobilisation (splint) is performed with:
- a rigid cervical collar
- a vacuum mattress
- a stretcher under it (the longitudinal stiffness of the mattress alone is not sufficient).
Preparation of the vacuum mattress

The vacuum mattress is put on a stretcher or possibly on a long spine board. The straps are put under the mattress, along its side, so they do not reach the ground. Then, the polystyrene balls are distributed evenly through the mattress by shaking its surface. A section with fewer balls would be less rigid. It is also possible to concentrate the balls in a given point to make this place more rigid. Finally, a sheet is put on the mattress. The sheet is folded so it will be possible to pull it to wrap the casualty into it; the profile has an S-shape.
The team member also checks that the pump (manual or electrical) works in the right direction.
Moulding the mattress
There are three ways to put the casualty on the vacuum mattress:
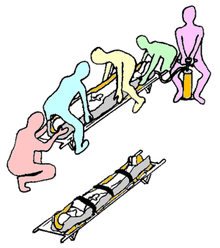
- lifting the casualty and pushing the stretcher under it. This method requires five team members (four lifting and one pushing the stretcher) and should be used when a spine or a pelvis trauma are suspected;
- the casualty is lifted with a scoop stretcher. The scoop stretcher is put on the mattress and opened to release the casualty;
- the casualty is lifted on a long spine board. The board is put on the mattress and the casualty is lifted (best with four team members) and one team member removes the board.
In all cases, the vacuum valve is up and at the feet of the casualty.
Once the casualty is on the mattress, the sheet is wrapped around him/her and the sides of the mattress are folded against their body. The top of the head must be kept clear (the mattress could retract when pumping out the air and thus compress the spine). The air is pumped until the mattress is rigid, then the valve is closed and the straps are fastened.
When only three team members are available and there is no scoop stretcher, the following procedure can be used:
- the vacuum mattress is put besides the casualty, on a protecting ground sheet, and partially depressed (three manual pumping) to make it more rigid and thinner. A sheet is put on the mattress, closer to the casualty;
- the casualty is put on their side, with a procedure that is similar to the recovery position;
- the team member at the legs pushes the mattress against the back of the casualty. The ground sheet helps to slide the mattress on the floor;
- the casualty is put on their back, overlapping the side of the mattress;
- the casualty is centred on the mattress; the sheet helps sliding the casualty on the mattress;
- the straps are tied to mould the mattress. The team leader moulds the sides of the head manually;
- the air is pumped;
- a long spine board is placed along the axis of the mattress. Two team members face each other and hold the mattress's handles at the head and at the thighs. They lift a few centimetres, the ground sheet is removed and the board is slid under the mattress to ensure longitudinal rigidity;
- the board can then be lifted (with the mattress on it), and put on the stretcher.
While the lifting methods can induce a flexing of the spine, this rolling method can be hazardous for several reasons: the risk of a torsion of the spine when rolling, the risk when sliding the casualty on the mattress, the risk of anteversion of the hips (and thus of flexing of the spine) due to the weight of the legs when lifting the mattress to slide the board.
Advantages and disadvantages
The vacuum mattress is an alternative to the use of a long spine board. Its advantages are:
- it is comfortable;
- it is adapted to all traumas, included spine and femoral traumas;
- the patient feels secured;
- it can be used instead of a stretcher for manual transportation (with the handles, e.g. in stairs) when longitudinal rigidity is not critical, or for short distances with six team members.
Its drawbacks are:
- it is relatively fragile, and becomes useless if only partially inflated (the vacuum requires a perfectly sealed envelope);
- It is more expensive than the traditional long spine board
- The process of vacuuming the bag is often longer than experienced individuals transferring a casualty to a standard spinal board.
See also
External links
- A photographic guide to pre-hospital spinal care (PDF file, 235p, 9 Mb)
| ||||||||||||||||||||