Spondylolysis
| Spondylolysis | |
|---|---|
| Classification and external resources | |
 Spondylolysis | |
| ICD-10 | M43.0 |
| ICD-9 | 738.4 |
| DiseasesDB | 12322 |
| eMedicine | radio/650 |
| MeSH | D013169 |
Spondylolysis is a defect of a vertebra. More specifically it is defined as a defect in the pars interarticularis of the vertebral arch.[1] The great majority of cases occur in the lowest of the lumbar vertebrae (L5), but spondylolysis may also occur in the other lumbar vertebrae, as well as in the thoracic vertebrae.
Spondylolysis occurs in three to six percent of the population.[2][3]
Signs and symptoms
Spondylolysis pain can lead to reduced mobility and inactivity. Inactivity can result in weight gain, loss of bone density, and loss of muscle strength and flexibility of other areas of the body. Spondylolysis can progress until one or more vertebrae slip out of place which is then called spondylolisthesis.
Over time, degenerative changes of spondylolysis can cause serious complications including:[4]
- low back, mid back, and neck pain
- Spinal Stenosis – where the spinal canal becomes narrow and the spinal cord can become pinched; can occur in the neck or low back.
- Cauda equina syndrome – a syndrome where the nerves at the bottom of the spinal cord are compressed by an intervertebral disc or mass; rare but can cause severe nerve problems.
- Radiculopathy – a condition where one or more spinal nerves are compressed.
- Cervical Myelopathy – when the spinal canal narrows to the point that causes spinal cord injury.
Risk factors
Spondylolysis (spon-dee-low-lye-sis) also runs in families and is more prevalent in some populations, suggesting a hereditary component such as a tendency toward thin vertebral bone.
Although this condition can be caused by repetitive trauma done to the lumbar spine or strenuous sports such as football or gymnastics, anatomy also plays a major role. According to research done in 2007, genetic make up of the lumbar spine has much to do with the occurrence of spondylolysis in certain individuals.[citation needed] A study done on 115 male skeletons with L5 spondylolysis was proof that a slight tweek in the anatomy of the spine can increase the likelihood of spondylolysis. In those with spondylolysis, many times the inter-facet region of vertebra L4 is more trapezoidal in shape with a larger width than that of a normal vertebra. This also changes the iner-facet height, making them shorter and narrower. With this defect in the spine, a normal load applied to the spine will be greater compared to those without it. This is due to reduced surface area and torsional range of motion during twists and bends.
Spondylolysis has a higher occurrence in the following activities:
- Tennis
- Diving
- Cheerleading
- Gymnastics
- Football
- Soccer
- Wrestling
- Weightlifting
- Cricket (Fast Bowling)
- Rugby
- Volleyball
Age, sex, and genetic can also be risk factors. Males are more commonly affected by spondylolysis than women. Also individuals under the age of 26 are more likely affected and are commonly diagnosed by the age of 16. Studies have shown a certain defect in the C4 vertebra can be a risk factor for this disease. The defect includes an alteration in the size and shape of the neural arch, which includes a greater width and narrower articular facets.[5]
Pathophysiology

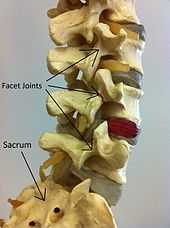
Spondylolysis is a defect of the lumbar vertebra in the spinal column. The lumbar vertebra consist of a body, pedicle, lamina, pars interarticularis, transverse process, spinous process and superior articular facets, which form joints that link the vertebrae together.
Specifically, spondylolysis involves pars interarticularis. When looking at the lumbar vertebra from the axial view, it is the bony mass between the facet joints, anterior to the lamina and posterior to the pedicle. When spondylolysis is present in the spine, it means that the pars interarticularis is detached and there is a separation of the joints. [citation needed]
It is typically caused by stress fracture of the bone, and is especially common in adolescents who overtrain in activities. It has been proposed that the pars interarticularis is especially vulnerable when the spine is in an extended position, and a force suddenly presses the vertebrae together, such as when landing on one's feet after a hop. This pressure acts like a nut-cracker on the pars interarticularis and can fracture it in susceptible individuals.[6]
Complications
Spondylolysis is the most common cause of spondylolisthesis in pediatric patients with a classic presentation that of a female gymnast. In the older population, degenerative disc disease commonly leads to spondylolisthesis without spondylolysis; in these instances, the spinal canal narrows because the spino-laminar arch at one level slides forward on the lower level effectively flattening the canal. The hereditary factor mentioned above is quite notable, since the frequency of spondylolisthesis among the Inuit peoples is 30–50%; however, there is controversy about this, as can be seen on the wiki page for spondylolisthesis: "(This statistic is controversial, however, because further anthropological studies have shown that the occurrence of spondylolysis in Inuit people living in Western-style communities is within the normal variancy at 7%. These people are hereditarily linked to the study group showing ~40%. It is theorized that the nomadic Inuit have a higher incidence of spondylolysis due to trauma acquired as infants by being carried in an amauti. While in an amauti, the baby is put into compressive extension with each step taken by the mother. Also, all other studies have shown a normal variance of spondylolysis within cultures of 6–10%, further suggesting that spondylolysis is an environmental abnormality and that a hereditary tie is very unlikely). [citation needed]
Treatment
Rehabilitation
The most notable non-surgical rehabilitation procedure done with an individual with spondylolysis is Physical Therapy. Therapy usually ranges from 3 to 6 months depending on the status of the injury. The main objective for rehabilitation is to strengthen core abdominal muscles so that they can stabilize the lower back and pelvis, improve motion in the hip joints and mid back so movement can occur above and below the site of injury, and most importantly, teach movement patterns that encourage stability of the spine while using motion in the hip joints and mid back instead. The goal is to minimize movement at the unstable pars defect. Besides physical therapy, treatments for acute spondylolysis include resting from sports participation or wearing a Boston overlap brace (anti-lordotic brace) (MassGeneral Hospital for Children). Medication such as ibuprofen and other pain relievers may also be used during these treatments to reduce the pain and decrease inflammation. During treatment, the patient is usually asked to stay off their feet and get as much rest as they can by lying down for the majority of the day. If for any reason the patient should do any sort of activity, the brace should be worn to prevent any excessive movement or bad bending. When the patient is done with Physical Therapy and has no sign of pain or inflammation in the lower back, they are cleared to continue with daily or athletic activities but may need to continue further lower back workouts assigned by the therapist. The Boston overlap brace may need to be worn some more if the patient wishes in order to prevent any faulty posture or excessive transverse movements. Approximately 80–85% of patients have shown pain relief after having these treatments. Surgery may be done to those who have not had success with treatments but this is rarely common.
Surgery
Most patients with spondylolysis do not require surgery but when symptoms are not relieved with non surgical treatments, then patients may require surgery. There are two types of surgery for this condition:[7]
- Laminectomy: This is a procedure to remove the lamina from the bony ring of the vertebra and release pressure. This pressure can be caused by nerve compression or herniated discs. The laminectomy is commonly performed on the vertebrae in the lower back and in the neck.
- Posterior Lumbar Fusion: Fusion is recommended when a set of vertebrae becomes loose or unstable. Spinal fusion is a procedure that joins two or more bones (vertebrae) together into one solid one which will prevent the joints and bones from moving. Surgeons apply metal screws, and rods to hold the bones securely while they fuse. This procedure is used to treat spine stability, fractures in the lumbar spine and, severe degenerative disc disease.
Epidemiology
In the US in 2009 there were 33,249 hospital admissions, 21, 507 in women and the remainder in men, with no in-hospital deaths. Of this number, only 137 were 1–17 years-old, as compared with 3,977 aged 18–44, and 14, 723 aged 45–64, 13, 810 aged 65–84, and 695 aged 85+. The average stay was between 3 and 4 days for all age groups.[8]
References
- ↑ "Spondylolisthesis". Retrieved 2007-07-05.
- ↑ Standaert CJ, Herring SA (2000). "Spondylolysis: a critical review". British journal of sports medicine 34 (6): 415–22. doi:10.1136/bjsm.34.6.415. PMC 1724260. PMID 11131228.
- ↑ Bono CM (1 February 2004). "Low-back pain in athletes". The Journal of bone and joint surgery. American volume 86–A (2): 382–96. PMID 14960688.
- ↑ http://www.emedicinehealth.com/spondylosis/page14_em.htm
- ↑ http://orthoinfo.aaos.org/topic.cfm?topic=a00053
- ↑ Schwab, FJ; Farcy, JP; Roye DP, Jr (Jul 15, 1997). "The sagittal pelvic tilt index as a criterion in the evaluation of spondylolisthesis. Preliminary observations.". Spine 22 (14): 1661–7. PMID 9253103.
- ↑ http://www.orthogate.org/patient-education/lumbar-spine/lumbar-spondylolysis.html
- ↑ http://www.hcup-us.ahrq.gov/tech_assist/tutorials.jsp
External links
- Information from the American Academy of Orthopaedic Surgeons
- A Patient's Guide to Lumbar Spondylolysis
- spondylosis treatement
- http://www.orthoseek.com/articles/spondyl.html
- http://www.hcup-us.ahrq.gov/tech_assist/tutorials.jsp
- http://www.orthonurse.org/portals/0/spondy.pdf Spondylolysis and Spondylolisthesis of the Lumbar Spine Pediatric Orthopaedic Department Massachusetts General Hospital] at the Mass General hospital for Children
- http://www.orthogate.org/patient-education/lumbar-spine/lumbar-spondylolysis.html
- http://www.emedicinehealth.com/spondylosis/page14_em.htm
| ||||||||||||||||||||||||||||