Pelvimetry

Pelvimetry is the assessment of the female pelvis[1] in relation to the birth of a baby. Traditional obstetrical services relied heavily on pelvimetry in the conduct of delivery in order to decide if natural or operative vaginal delivery was possible or if and when to use a cesarean section.[2]
Use
Pelvimetry used to be performed routinely to discern if spontaneous labour was medically advisable. Women whose pelvises were deemed too small received caesarean sections instead of birthing naturally. Research indicates that pelvimetry is not a useful diagnostic tool for CPD (see below) and that in all cases spontaneous labour and birthing should be facilitated.[3]
A woman's pelvis loosens up before birth (with the help of hormones), and an upright and/or squatting woman can birth a considerably larger baby. A woman in the lithotomy (lying on her back, legs elevated) is more than likely not going to push a larger than average baby out, due to the size of outlet that this position creates.
Cephalo-pelvic disproportion: CPD
Cephalo-pelvic disproportion exists when the capacity of the pelvis is inadequate to allow the fetus to negotiate the birth canal.
Terminology
The terms used in pelvimetry are commonly used in obstetrics. Clinical pelvimetry attempts to assess the pelvis by clinical examination. Pelvimetry can also be done by radiography and MRI.
Pelvic planes
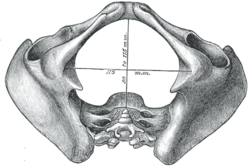
- Pelvic inlet: The line between the narrowest bony points formed by the sacral promontory and the inner pubic arch is termed obstetrical conjugate: It should be 11.5 cm or more. This anteroposterior line at the inlet is 2 cm less than the diagonal conjugate (distance from undersurface of pubic arch to sacral promontory). The transverse diameter of the pelvic inlet measures 13.5 cm.
- Midpelvis: The line between the narrowest bone points connects the ischial spines; it typically exceeds 12 cm.
- Pelvic outlet: The distance between the ischial tuberosities (normally > 10 cm), and the angulation of the pubic arch.
Pelvic types
Traditional obstetrics characterizes four types of pelvises:
- Gynecoid: Ideal shape, with round to slightly oval (obstetrical inlet slightly less transverse) inlet: best chances for normal vaginal delivery.
- Android: triangular inlet, and prominent ischial spines, more angulated pubic arch.
- Anthropoid: the widest transverse diameter is less than the anteroposterior (obstetrical) diameter.
- Platypelloid: Flat inlet with shortened obstetrical diameter.
ADDITION BY ROBERT NGABO from BSNM IN GENERAL NURSING_TYPES OF PELVIS
There are four classifications of pelvises. They are the gynecoid, most common female pelvis shape; the android, the most common male shape; the anthropoid, a long pelvis; and a platypelloid or flat-shaped pelvis
The Gynaecoid or genuine female pelvis
It has an almost round brim and will permit the passage of an average-sized baby with the least amount of trauma to the mother and baby in normal circumstances. The pelvic cavity (the inside of the pelvis) is usually shallow, with straight side walls and with the ischial spines not so prominent as to cause a problem as the baby moves through.
The Android pelvis
It has a heart-shaped brim and is quite narrow in front. This type of pelvis is likely to occur in tall women with narrow hips and is also found in African women. The pelvic cavity and outlet is often narrow, straight and long. The ischial spines are prominent. Women with this shape pelvis may have babies that lie with their backs against their mothers’ backs and may experience longer labours. It is important that these women take an active role during their labour and need to squat and move around as much as possible.
The Anthropoid pelvis
It has an oval brim and a slightly narrow pelvic cavity. The outlet is large, although some of the other diameters may be reduced. If the baby engages in the pelvis in an anterior position, labour would be expected to be straightforward in most cases.
The Platypelloid pelvis
It has a kidney-shaped brim and the pelvic cavity is usually shallow and may be narrow in the antero-posterior (front to back) diameter. The outlet is usually roomy. During labour the baby may have difficulty entering the pelvis, but once in, there should be no further difficulty
OTHER DESCRIPTION 1. The Gyneacoid Pelvis: As described above, is the true female pelvis. Its main features are the rounded brim, the generous fore – pelvis (the part in front of the transverse diameter), straight side walls, and a shallow cavity with a broad, well – curved sacrum, blunt ischial spines, a wide sciatic notch and a pubic arch of 90 degrees. It is found in women of average build and height with a shoe size of 4 or larger. It is well suited to child bearing.
2. The Android Pelvis: Is so called because it resembles the male pelvis. Its brim is heart shaped with a narrow fore – pelvis, and has a transverse diameter which is towards the back. The side walls coverage, making it a funnel shape with a deep cavity and a straight sacrum. The ischial spines are prominent and the sciatic notch is narrow. The angle of the pubic arch is less than 90 degrees.
It is found in short and heavily built women who have a tendency to be hirsute.
This type of pelvis predisposes to an occipito posterior position of the fetal head and is the least suited to child – bearing.
3. The Anthropoid Pelvis: Has a long, oval brim in which the antero posterior diameter is longer than the transverse. The side walls diverge and the sacrum is long and deeply concave. The ischial spines are not prominent and the sciatic notch is very wide, as is the sub – pubic angle. Women with this type of pelvis tend to be tall, with narrow shoulders. Labor does not usually present any difficulties, but a direct occipito – posterior position is often a feature.
4. The Platypelloid Pelvis: is flat, with a kidney shaped brim in which the anteroposterior diameter is reduced and the transverse increased. The side walls diverge, the sacrum is flat and the cavity shallow. The ischial spines are blunt, and the sciatic notch and the sub – pubic angle are both wide. The head must engage with the sagittal suture in the transverse diameter, but usually descends through the cavity without difficulty
Fetal relationship
- Engagement: The fetus is engaged if the widest leading part (typically the widest circumference of the head) is negotiating the inlet.
- Station: Relationship of the bony presenting part of the fetus to the maternal ischial spines. If at the level of the spines it is at “0 (zero)” station, if it passed it by 2cm it is at “+2” station.
- Attitude: Relationship of fetal head to spine: flexed, neutral (“military”), or extended attitudes are possible.
- Position: Relationship of presenting part to maternal pelvis, i.e. ROP=right occiput posterior, or LOA=left occiput anterior.
- Presentation: Relationship between the leading fetal part and the pelvic inlet: cephalic, breech (complete, incomplete, frank or footling), face, brow, mentum or shoulder presentation.
- Lie: Relationship between the longitudinal axis of fetus and long axis of the uterus: longitudinal, oblique, and transverse.
- Caput or Caput succedaneum: oedema typically formed by the tissue overlying the fetal skull during the vaginal birthing process.
See also
- Childbirth
- List of obstetric topics
- Pelvic Bone Width
- Human pelvis
- Pregnancy
- Pubic symphysis
- Sacroiliac joint
- Sacrum
References
- ↑ "pelvimetry" at Dorland's Medical Dictionary
- ↑ "Yale - The Pelvic Survey".
- ↑ Blackadar CS, Viera A: "A Retrospective Review of Performance and Utility of Routine Clinical Pelvimetry", AAFP, 2003, v36:7, p505
| |||||||||||||||||||||||||||||||||||||||||||||||||||