Pelvic tilt
From Wikipedia, the free encyclopedia
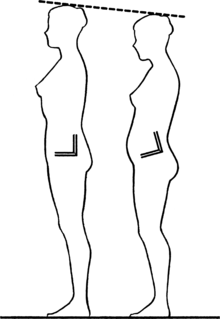
A visual comparison between a neutral and anterior pelvic tilt and how it can affect height.
In anatomy, pelvic tilt is the orientation of the pelvis in respect to the femurs it rests upon and in space. It can tilt in four basic directions.
Forms
- Anterior pelvic tilt is when the front of the pelvis drops and the back of the pelvis rises. This happens when the hip flexors shorten and the hip extensors lengthen.
- Posterior pelvic tilt is the opposite, when the front of the pelvis rises and the back of the pelvis drops. This happens when the hip flexors lengthen and the hip extensors shorten, particularly the gluteus maximus which is the primary hyperextensor of the hip.

A hemihyperplasia patient demonstrating lateral pelvic tilt.
- Lateral pelvic tilt describes tilting in both directions and is associated with scoliosis or people who have legs of different length. It can also happen when one leg is bent while the other remains straight, in that case the bent side's hip can follow the femur as knee lowers towards the ground.
- Left pelvic tilt is when the right side of the pelvis is elevated higher than the left side.
- Right pelvic tilt is when the left side of the pelvis is elevated higher than the right side.
Balance
- To keep balance standing upright with anterior tilt, the spine is hyper-extended with the rectus abdominis lengthening and the erector spinae shortening. This is associated with lordosis. Lordosis does not always occur with anterior tilt when the weight is borne in other ways, such as when supported by the arms, or when the hips drift backward (posterior femur tilt) or when enough hip flexion occurs that a kyphotic spine can be balanced over an anterior tilted pelvis.
- To keep balance with posterior tilt, the spine is rounded with the rectus shortened and the erector spinae lengthened. This leads to a kyphotic posture. Kyphosis does not always occur in tandem with posterior tilt, when the weight is born in other ways, such as on the hands, which can allow a posteriorly tilted pelvis with a neutral or even lordotic spine.
- To keep balance with lateral tilt, rather than remaining upright the femur usually tilts to keep the weight centered over it. This requires a muscular effort by the hip abductors (glutei medii and minimi of either side) to pull the pelvis up onto the femur. Otherwise, the pelvis would drop towards the airborne leg.
See also
- Adho Mukha Śvānāsana involves anterior pelvic tilt while the spine remains neutral (in axial extension) so there is not lordosis.
- Bridge (exercise) and Chakrāsana involves posterior pelvic tilt, unlike standing the spine is extended rather than rounded because it is not being balanced upright, the weight is born between the feet and hands rather than the pelvis.
- Ūrdhvadhanurāsana and Uṣṭhāsana also involve this to a less contorted degree.
- Scoliosis
- Uttānāsana and other inverted forward bend poses combine anterior pelvic tilt with kyphosis because the intention is not to remain upright.
External links
- Exercise Info on ExRx.net explanation of postural deficiencies
- Exercises for correcting anterior pelvic tilt
- Exercising pelvic tilt related to Rolfing.
This article is issued from Wikipedia. The text is available under the Creative Commons Attribution/Share Alike; additional terms may apply for the media files.