Muscles of respiration
The various muscles of respiration aid in both inspiration and expiration, which require changes in the pressure within the thoracic cavity. The respiratory muscles work to achieve this by changing the dimensions of the thoracic cavity.
The principal muscles are the diaphragm, the external intercostal and the interchondral part of the internal intercostal muscles. Both the external intercostal muscles and the intercondral elevate the ribs, thus increasing the width of the thoracic cavity, while the diaphragm contracts to increase the vertical dimensions of the thoracic cavity, and also aids in the elevation of the lower ribs.
Accessory muscles are typically only used when the body needs to process energy quickly (e.g. during strenuous exercise, during the stress response, or during an asthma attack). The accessory muscles of inspiration can also become engaged in everyday breathing when a breathing pattern disorder exists.
Diaphragm
| Diaphragm | |
|---|---|
 | |
| Respiratory system | |
| Latin | diaphragma |
| Gray's | subject #117 404 |
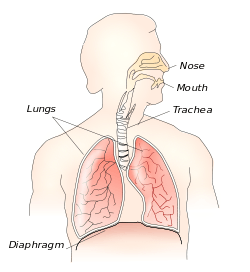
The diaphragm is crucial for breathing and respiration. It's responsible for 45% of the air that enters the lungs during quiet breathing. During inhalation, the diaphragm contracts, thus enlarging the thoracic cavity (the external intercostal muscles also participate in this enlargement). This reduces intra-thoracic pressure: in other words, enlarging the cavity creates suction that draws air into the lungs. When the diaphragm relaxes, air is exhaled by elastic recoil of the lung and the tissues lining the thoracic cavity in conjunction with the abdominal muscles which act as an antagonist paired with the diaphragm's contraction.
It is not responsible for all the breathing related to voice. One has more voluntary control over the abdominals and intercostals than the actual diaphragm,[1] which has relatively few proprioceptive nerve endings (citation?). Because of this, there may be little difference between "chest" breathing and "diaphragmatic" breathing. There is a more prominent vertical movement of the ribcage in "chest" breathing compared to "diaphragmatic" breathing, while the movement of the diaphragm is about the same in both types of breathing.[1] The action of the diaphragm can be indirectly controlled by training proper posture and balance in the rest of the body. The diaphragm naturally strengthens and works in concert with surrounding structures rather than in isolation.
The diaphragm is also involved in non-respiratory functions, helping to expel vomit, feces, and urine from the body by increasing intra-abdominal pressure, and preventing acid reflux by exerting pressure on the esophagus as it passes through the esophageal hiatus.
Intercostal muscles
Along with the diaphragm, the intercostal muscles are one of the most important groups of respiratory muscles. The external intercostals are responsible for ~25% of the air that enters the lungs during quiet breathing. These muscles are attached between each rib and are important in manipulating the width of the thoracic cage. There are three layers of intercostal muscles:
- The external intercostal have fibres that go forward and downward (obliquely downward and forward from rib to rib).[2] These fibres are called the antero-inferior, and are sometimes referred to as the front pocket muscle since the fibres mimic the direction a hand would enter a front pocket. The external intercostals assist in deep inspiration by increasing the anterioposterior diameter of the chest.
- The internal intercostal also have fibres, which go backward and downward (obliquely downward and posteriorly from rib to rib).[2] These are called the postero-superior[citation needed], or the back pocket muscles. The internal intercostals assist in expiration by pulling the ribcage down.
- The last layer is the innermost intercostals and consists of three separate parts; the subcostal (posteriorly), the innermost intercostal (laterally, which often causes confusion with the innermost intercostal referring to all twenty groups) and the transversus thoracis (anteriorly).
The antero-inferior fibres have the effect of lifting up the ribs during contraction. Anteriorly, the external intercostal muscles do not directly attach to the sternum, but are replaced by the anterior intercostal membrane.
The innermost intercostal muscles are also "back pocket" muscles. The internal and innermost intercostals have the opposite effect of the external intercostals and aid in forced expiration. The internal intercostal is replaced by the posterior intercostal membrane posteriorly.
Accessory muscles of inspiration
There is some controversy as to which muscles may be considered accessory muscles of inspiration (Kendalll, McCreary, Provance, Rodgers, Romani, 2005). Part of the problem may stem from the difficulty to fully relax the neck muscles during the recording of respiration (even in supine position; especially, when a mouthpiece is used).[3] The sternocleidomastoid (elevated sternum) and the scalene muscles (anterior, middle and posterior scalene) are typically considered accessory muscles of breathing.[4] The involvement of these muscles seems to depend on the respiratory activity. During quiet breathing, the scalenes are consistently phasically active, while the sternocleidomastoids are quiet.[5] With an increase in the respiratory volume, sternocleidomastoids also become active.[3] Both muscles are simultaneously activated with when one breathes in at the maximal flow rate.[5] Apart from these neck muscles, the following muscles have also been observed contributing to the breathing: serratus anterior, pectoralis major & minor, upper trapezius, latissimus dorsi, erector spinae (thoracic), iliocostalis lumborum, quadratus lumborum, serratus posterior superior and inferior, levatores costarum, transversus thoracis, subclavius (Kendall et al., 2005). The abdominal muscles relax.
Scalene muscle activation coincides with the diaphragm even at rest in most humans, suggesting it could be considered a primary muscle of respiration[6]
If a breathing pattern disorder exists, as in the event of an asthma attack, the accessory muscles of inspiration may become overused.
Muscles of expiration
During quiet breathing, there is little or no muscle contraction/relaxation involved in expiration. This process is simply driven by the elastic recoil of the lungs in healthy individuals. In certain conditions the elasticity of the lung can be lost, such as in emphysema. Forced or active expiration occurs in such individuals as well as occurring during exercise. The abdominal muscles and the internal and innermost intercostal muscles help expel air.
References
- ↑ 1.0 1.1 Wade, O. L. (1954). Movements of the thoracic cage and diaphragm in respiration. The Journal of physiology, 124(2), 193.
- ↑ 2.0 2.1 Kim E. Barrett; Susan M. Barman; Scott Boitano; Heddwen Brooks (24 July 2009). "35. Pulmonary Function". Ganong's Review of Medical Physiology, 23rd Edition. McGraw-Hill Companies,Incorporated. ISBN 978-0-07-160567-0.
- ↑ 3.0 3.1 Campbell, E. J. M. (1955). The role of the scalene and sternomastoid muscles in breathing in normal subjects. An electromyographic study. Journal of Anatomy, 89, 378.
- ↑ Netter FH. Atlas of Human Anatomy 3rd ed. Icon Learning Systems. Teterboro, New Jersey 2003 - plate 191
- ↑ 5.0 5.1 Raper, A. J., Thompson, W. T., Shapiro, W., & Patterson, J. L. (1966). Scalene and sternomastoid muscle function. Journal of Applied Physiology, 21, 497-502.
- ↑ De Troyer A: Respiratory muscle function. In: Gibson J, Geddes DM, Costabel U, et al ed. Respiratory Medicine, London: Saunders; 2003:119-129.
Further reading
- Kendall, F., McCreary, E., Provance, P., Rodgers, M., Romai, W. (2005). Muscles testing and function with posture and pain (5th ed.). PA, USA: Lippincott Williams & Wilkins.