Tetrahydrocannabinol
 |
|
|---|---|
 |
|
| Systematic (IUPAC) name | |
| (−)-(6aR,10aR)-6,6,9-trimethyl- 3-pentyl-6a,7,8,10a-tetrahydro- 6H-benzo[c]chromen-1-ol |
|
| Identifiers | |
| CAS number | 1972-08-3 |
| ATC code | A04AD10 |
| PubChem | CID 16078 |
| DrugBank | DB00470 |
| ChemSpider | 15266 |
| Chemical data | |
| Formula | C21H30O2 |
| Mol. mass | 314.45 |
| SMILES | eMolecules & PubChem |
| Synonyms | Dronabinol |
| Physical data | |
| Boiling point | 157 °C (315 °F) [2] |
| Solubility in water | 0.0028 [1] (23 °C) mg/mL (20 °C) |
| Spec. rot | -152° (ethanol) |
| Pharmacokinetic data | |
| Bioavailability | 10-35% (inhalation), 6-20% (oral)[3] |
| Protein binding | 95-99%[3] |
| Metabolism | mostly hepatic by CYP2C[3] |
| Half-life | 1.6-59 hours [3], 25-36 hours (orally administered Dronabinol) |
| Excretion | 65-80% (feces), 20-35% (urine) as acid metabolites[3] |
| Therapeutic considerations | |
| Pregnancy cat. | C |
| Legal status | Schedule I and III (US) |
| |
|


Tetrahydrocannabinol (pronounced /ˌtɛtrəˌhaɪdrɵkəˈnæbɨnɒl/ tet-rə-HYE-drə-kə-NAB-i-nol) (THC), also known as delta-9-tetrahydrocannabinol (Δ9-THC), Δ1-THC (using an older chemical nomenclature), or dronabinol, is the main psychoactive substance found in the cannabis plant.
It was first isolated by Yechiel Gaoni and Raphael Mechoulam from the Weizmann Institute of Science in Rehovot, Israel, in 1964.[4][5][6] In pure form, it is a glassy solid when cold and becomes viscous and sticky if warmed. An aromatic terpenoid, THC has a very low solubility in water, but good solubility in most organic solvents.
Like most pharmacologically-active secondary metabolites of plants, THC in cannabis is assumed to be involved in self-defense, perhaps against herbivores.[7] THC also possesses high UV-B (280-315 nm) absorption properties, which, it has been speculated, could protect the plant from harmful UV radiation exposure.[8][9][10]
Dronabinol is the International Nonproprietary Name (INN) for a pure isomer of THC, (-)-trans-Δ9-tetrahydrocannabinol, that is, the main isomer in cannabis.[11] It is sold as Marinol (a registered trademark of Solvay Pharmaceuticals). Dronabinol is also marketed, sold, and distributed by PAR Pharmaceutical Companies under the terms of a license and distribution agreement with SVC pharma LP, an affiliate of Rhodes Technologies.
Contents |
Pharmacology
The pharmacological actions of THC result from its binding to the cannabinoid receptor CB1, located mainly in the central nervous system, and the CB2 receptor, mainly present in cells of the immune system. It acts as a partial agonist on both receptors, i.e., it activates them but not to their full extent. The psychoactive effects of THC are mediated by its activation of the CB1 receptor, which is the most abundant G protein-coupled receptor in the brain.
The presence of these specialized receptors in the brain implied to researchers that endogenous cannabinoids are manufactured by the body, so the search began for a substance normally manufactured in the brain that binds to these receptors, the so-called natural ligand or agonist, leading to the eventual discovery of anandamide, 2-arachidonyl glyceride (2-AG), and other related compounds known as endocannabinoids. This is similar to the story of the discovery of endogenous opiates (endorphins, enkephalins, and dynorphin), after the realization that morphine and other opiates bind to specific receptors in the brain. In addition, it has been shown that cannabinoids, through an unknown mechanism, activate endogenous opioid pathways involving the μ1 opioid receptor, precipitating a dopamine release in the nucleus accumbens. The effects of the drug can be suppressed by the CB1 cannabinoid receptor antagonist rimonabant (SR141716A) as well as opioid receptor antagonists (opioid blockers) naloxone and naloxonazine.[12]
The mechanism of endocannabinoid synaptic transmission is thought to occur as follows: First, transmission of the excitatory neurotransmitter glutamate causes an influx of calcium ions into the post-synaptic neuron. Through a mechanism not yet fully understood, the presence of post-synaptic calcium induces the production of endocannabinoids in the post-synaptic neuron. These endocannabinoids (such as anandamide), then, are released into the synaptic cleft, where binding occurs at cannabinoid receptors present on pre-synaptic neurons, where they modulate neurotransmission. Thus, this form of neurotransmission is termed retrograde transmission, as the signal is carried in the opposite direction of orthodox propagation, which previously was thought to be exclusively one way.
THC has mild to moderate analgesic effects, and cannabis can be used to treat pain. The mechanism for analgesic effects caused directly by THC or other cannabinoid agonists is not fully understood. Other effects include relaxation; euphoria; altered space-time perception; alteration of visual, auditory, and olfactory senses; anxiety; disorientation; fatigue; and appetite stimulation (colloquially known as "the munchies"). The mechanism for appetite stimulation in subjects is believed to result from activity in the gastro-hypothalamic axis. CB1 activity in the hunger centers in the hypothalamus increases the palatability of food when levels of a hunger hormone ghrelin increase as food enters the stomach. After chyme is passed into the duodenum, signaling hormones such as cholecystokinin and leptin are released, causing reduction in gastric emptying and transmission of satiety signals to the hypothalamus. Cannabinoid activity is reduced through the satiety signals induced by leptin release. It also has anti-emetic properties, and also may reduce aggression in certain subjects.
THC has an active metabolite, 11-Hydroxy-THC, which may also play a role in the analgesic and recreational effects of cannabis.
The α7 nicotinic receptor antagonist methyllycaconitine can block self-administration of THC in rats comparable to the effects of varenicline on nicotine administration.[13][14]
Toxicity
There has never been a documented human fatality from overdosing on tetrahydrocannabinol or cannabis.[15] Information about THC's toxicity is derived from animal studies. The toxicity depends on the route of administration and the laboratory animal. Absorption is limited by serum lipids, which can become saturated with THC, mitigating toxicity.[16] According to the Merck Index, 12th edition, THC has a LD50 (dose killing half of the research subjects) value of 1270 mg/kg (male rats) and 730 mg/kg (female rats) administered orally dissolved in sesame oil.[17] The LD50 value for rats by inhalation of THC is 42 mg/kg of body weight.[17] One estimate of THC's LD50 for humans indicates that about 1500 pounds (680 kilograms) of cannabis would have to be smoked within 14 minutes.[18] This estimate is supported by studies which indicate that the effective dose of THC is at least 1000 times lower than the estimated lethal dose (a "therapeutic ratio" of 1000:1). This is much higher than alcohol (therapeutic ratio 10:1), cocaine (15:1), or heroin (6:1).[19]
| Animal | Administration | LD50 [mg/kg] |
|---|---|---|
| rat | oral | 666 [16] |
| rat (male) | oral | 1270 [17] |
| rat (female) | oral | 730 [17] |
| rat | inhalation | 42 [17] |
| rat | intraperitoneal | 373 [16] |
| rat | intravenous | 29 [16] |
| mouse | intravenous | 42 [16] |
| mouse | oral | 482 [16] |
| mouse | intraperitoneal | 168 [16] |
| monkey (LDLo) | intravenous | 128 [16] |
| dog | oral | 525 [16] |
Research
The discovery of THC was first described in "Isolation, structure and partial synthesis of an active constituent of hashish", published in the Journal of the American Chemical Society in 1964.[4] Research was also published in the academic journal Science, with "Marihuana chemistry" by Raphael Mechoulam in June 1970,[20] followed by "Chemical basis of hashish activity" in August 1970.[21] In the latter, the team of researchers from Hebrew University Pharmacy School and Tel Aviv University Medical School experimented on monkeys to isolate the active compounds in hashish. Their results provided evidence that, except for tetrahydrocannabinol, no other major active compounds were present in hashish.
Studies in humans
A number of studies show that THC provides medical benefits for cancer and AIDS patients by increasing appetite and decreasing nausea. It has also been shown to assist some glaucoma patients by reducing pressure within the eye, and is used in the form of cannabis by a number of multiple sclerosis patients, who use it to alleviate neuropathic pain and spasticity. The National Multiple Sclerosis Society is currently supporting further research into these uses.[22]
In August 2009 a phase IV clinical trial by the Hadassah Medical Center in Jerusalem, Israel was started to investigate the effects of THC on post-traumatic stress disorders.[23] THC and other cannabinoid agonist have been shown to be beneficial both in open label studies, as well as in laboratory experiments with animals to ameliorate post-traumatic stress disorders.
Preliminary research on synthetic THC has been conducted on patients with Tourette syndrome, with results suggesting that it may help in reducing nervous tics and urges by a significant degree. Research on twelve patients showed that Marinol reduced tics with no significant adverse effects. A six-week controlled study on 24 patients showed that the patients taking dronabinol had a significant reduction in tic severity without serious adverse effects. Seven patients dropped out or had to be excluded from the study, one due to adverse side-effects. More significant reduction in tic severity was reported with longer treatment. No detrimental effects on cognitive functioning and a trend towards improvement in cognitive functioning were reported during and after treatment. Dronabinol's usefulness as a treatment for TS cannot be determined until/unless longer controlled studies on larger samples are undertaken.[24][25][26]
Dronabinol (Marinol®) is now a Schedule III medication which allows doctors to prescribe it for off label uses. It is now being prescribed to a small population of patients for ADHD and depression.
Studies in animals and in vitro
New scientific evidence is showing that THC can prevent Alzheimer's Disease in an animal model by preventing the inflammation caused by microglia cells which are activated by binding of amyloid protein.[27]
In in-vitro experiments, THC at extremely high concentrations, which could not be reached with commonly-consumed doses, caused inhibition of plaque formation (which are associated with Alzheimer's disease) better than currently-approved drugs.[28]
THC may also be an effective anti-cancer treatment, with studies showing tumor size reduction in mice conducted in 1975[29] and 2007[30], as well as in a pilot study in humans with glioblastoma multiforme (a type of brain cancer).[31]
A two-year study in which rats and mice were force-fed tetrahydrocannabinol dissolved in corn oil showed reduced body mass, enhanced survival rates, and decreased tumor incidences in several sites, mainly organs under hormonal control. It also caused testicular atrophy and uterine and ovarian hypoplasia, as well as hyperactivity and convulsions immediately after administration, of which the onset and frequency were dose related.[32]
Research in rats indicates that THC prevents hydroperoxide-induced oxidative damage as well as or better than other antioxidants in a chemical (Fenton reaction) system and neuronal cultures.[33] In mice low doses of Δ9-THC reduces the progression of atherosclerosis.[34]
Research has also shown that past claims of brain damage from cannabis use fail to hold up to the scientific method.[35] Instead, recent studies with synthetic cannabinoids show that activation of CB1 receptors can facilitate neurogenesis,[36] as well as neuroprotection[37], and can even help prevent natural neural degradation from neurodegenerative diseases such as MS, Parkinson's, and Alzheimer's. This, along with research into the CB2 receptor (throughout the immune system), has given the case for medical marijuana more support.[38][39] THC is both a CB1 and CB2 agonist.[40]
Research indicating negative side-effects
Conceivable long-term ill effects of THC on humans are disputed, yet its status as an illegal drug in most countries makes research difficult.
Some studies claim a variety of negative effects associated with constant, long-term use, including short-term memory loss.[41][42] Other studies have refuted this by evidence of MRIs of long-term users, showing little or no difference to MRIs of the non-using control group. Using positron emission tomography (PET), one study reports altered memory-related brain function in chronic daily marijuana users.[43]
Some studies have suggested that marijuana users have a greater risk of developing psychosis than non-users. This risk is most pronounced in cases with an existing risk of psychotic disorder.[44] Other studies have made similar associations, especially in individuals predisposed to psychosis prior to cannabis use.[45] A 2005 paper from the Dunedin study suggested an increased risk in the development of psychosis linked to polymorphisms in the COMT gene.[46] A literature review on the subject concluded that "Cannabis use appears to be neither a sufficient nor a necessary cause for psychosis. It is a component cause, part of a complex constellation of factors leading to psychosis."[47] Contrastingly, a French review from 2009 came to a conclusion that cannabis use, particularly that before age 15, was a factor in the development of schizophrenic disorders.[48] A 2008 German review reported that cannabis was supposedly a causal factor in some cases of schizophrenia and stressed the need for better education among the public due to increasingly relaxed access to cannabis.[49] Interestingly, however, though cannabis use has increased dramatically in several countries over the past few decades, the rates of psychosis and schizophrenia have generally not increased, casting some doubt over whether the drug can cause cases that would not otherwise have occurred[50]
Research from 2007 reported a correlation between cannabis use and increased cognitive function in schizophrenic patients.[51]
A 2008 National Institutes of Health study of 18 chronic heavy marijuana users with cardiac and cerebral abnormalities (averaging 78 to 350 marijuana cigarettes per week, or 30 g to 270 g (1 to 9.5 ounces)) and 24 controls found elevated levels of apolipoprotein C-III (apoC-III) in the chronic smokers.[52][53] An increase in apoC-III levels induces the development of hypertriglyceridemia.
A 2008 study by the University of Melbourne of 15 heavy marijuana users (consuming at least 5 marijuana cigarettes daily for on average 20 years) and 16 controls found an average size difference for the smokers in the hippocampus (12 percent smaller) and the amygdala (7 percent smaller).[54] It has been suggested that such effects can be reversed with long term abstinence.[55] However, the study indicates that they are unsure that the problems were caused by marijuana alone. Furthermore, this correlation might suggest self-medication by individuals with these brain features.
A 2008 study at Karolinska Institute suggested that young rats treated with THC received an increased motivation for drug use, heroin in the study, under conditions of stress.[56][57]
A 2009 study found that there was a high prevalence of cannabis in the toxicologic analysis of homicide (22%) and suicide victims (11%) in Australia.[58] In a similar study from Sweden it was also found that suicide victims had a significant higher use of cannabis, but the authors found that "this was explained by markers of psychological and behavioural problems".[59]
Biosynthesis
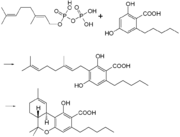
In the cannabis plant THC occurs mainly as tetrahydrocannabinol carboxylic acid (THC-COOH). The enzymatic condensation of geranyl pyrophosphate and olivetolic acid gives cannabigerolic acid[60], which is cyclized by the enzyme THC acid synthase to give THC-COOH. Heating decarboxylates the acid to THC.
Metabolism
THC is metabolized mainly to 11-OH-THC (11-hydroxy-THC) by the human body. This metabolite is still psychoactive and is further oxidized to 11-Nor-9-carboxy-THC (THC-COOH). In humans and animals, more than 100 metabolites could be identified, but 11-OH-THC and THC-COOH are the dominating metabolites. Metabolism occurs mainly in the liver by cytochrome P450 enzymes CYP2C9, CYP2C19, and CYP3A4. More than 55% of THC is excreted in the feces and ~20% in the urine. The main metabolite in urine is the ester of glucuronic acid and THC-COOH and free THC-COOH. In the feces, mainly 11-OH-THC was detected.[61]
Detection in body fluids
THC and THC-COOH can be quantitated in blood or urine using chromatographic techniques as part of a drug use testing program or in a forensic investigation of a traffic or other criminal offense or suspicious death. The concentrations obtained from such an analysis can often be helpful in distinguishing active from passive use or prescription from illicit use, elapsed time since use and extent or duration of use.[62]
Dronabinol
Synthetic THC is known as dronabinol. It is available as a prescription drug (under Marinol[63]) in several countries including the United States and Germany. In the United States, Marinol is a Schedule III drug, available by prescription, considered to be non-narcotic and to have a low risk of physical or mental dependence. Efforts to get cannabis rescheduled as analogous to Marinol have not succeeded thus far, though a 2002 petition has been accepted by the DEA. As a result of the rescheduling of Marinol from Schedule II to Schedule III, refills are now permitted for this substance. Marinol has been approved by the U.S. Food and Drug Administration (FDA) in the treatment of anorexia in AIDS patients, as well as for refractory nausea and vomiting of patients undergoing chemotherapy, which has raised much controversy as to why natural THC is still a schedule I drug.[64]
An analog of dronabinol, nabilone, is available commercially in Canada under the trade name Cesamet, manufactured by Valeant. Cesamet has also received FDA approval and began marketing in the U.S. in 2006; it is a Schedule II drug.
In April 2005, Canadian authorities approved the marketing of Sativex, a mouth spray for multiple sclerosis patients, who can use it to alleviate neuropathic pain and spasticity. Sativex contains tetrahydrocannabinol together with cannabidiol. It is marketed in Canada by GW Pharmaceuticals, being the first cannabis-based prescription drug in the world (in modern times). In addition, Sativex received European regulatory approval in 2010.
Comparisons to medical marijuana
Dronabinol is known to produce mild side effects similar to cannabis. Many scientists believe that dronabinol lacks the beneficial properties of cannabis, which contains more than 60 cannabinoids, including cannabidiol (CBD), thought to be the major anticonvulsant that helps multiple sclerosis patients;[65] and cannabichromene (CBC), an anti-inflammatory which may contribute to the pain-killing effect of cannabis.[66] Others have countered that the effects of all of cannabis's cannabinoids have not been completely studied and are not fully understood.
It takes over one hour for Marinol to reach full systemic effect,[67] compared to minutes for smoked or vaporized cannabis.[68] Some patients accustomed to inhaling just enough cannabis smoke to manage symptoms have complained of too-intense intoxication from Marinol's predetermined dosages. Many patients have said that Marinol produces a more acute psychedelic effect than cannabis, and it has been speculated that this disparity can be explained by the moderating effect of the many non-THC cannabinoids present in cannabis. Mark Kleiman, director of the Drug Policy Analysis Program at UCLA's School of Public Affairs said of Marinol, "It wasn't any fun and made the user feel bad, so it could be approved without any fear that it would penetrate the recreational market, and then used as a club with which to beat back the advocates of whole cannabis as a medicine."[69] United States federal law currently registers dronabinol as a Schedule III controlled substance, but all other cannabinoids remain Schedule I, except nabilone.
Regulatory history
Since at least 1986, the trend has been for THC in general, and especially the Marinol preparation, to be downgraded to less and less stringently-controlled schedules of controlled substances, in the U.S. and throughout the rest of the world.
On July 13, 1986, the Drug Enforcement Administration (DEA) issued a Final Rule and Statement of Policy authorizing the "Rescheduling of Synthetic Dronabinol in Sesame Oil and Encapsulated in Soft Gelatin Capsules From Schedule I to Schedule II" (DEA 51 FR 17476-78). This permitted medical use of Marinol, albeit with the severe restrictions associated with Schedule II status. For instance, refills of Marinol prescriptions were not permitted. At its 1045th meeting, on April 29, 1991, the Commission on Narcotic Drugs, in accordance with article 2, paragraphs 5 and 6, of the Convention on Psychotropic Substances, decided that Δ9-tetrahydrocannabinol (also referred to as Δ9-THC) and its stereochemical variants should be transferred from Schedule I to Schedule II of that Convention. This released Marinol from the restrictions imposed by Article 7 of the Convention [2].
An article published in the April-June 1998 issue of the Journal of Psychoactive Drugs found that "Healthcare professionals have detected no indication of scrip-chasing or doctor-shopping among the patients for whom they have prescribed dronabinol". The authors state that Marinol has a low potential for abuse[70].
In 1999, Marinol was rescheduled from Schedule II to III of the Controlled Substances Act, reflecting a finding that THC had a potential for abuse less than that of cocaine, and heroin. This rescheduling comprised part of the argument for a 2002 petition for removal of cannabis from Schedule I of the Controlled Substances Act, in which petitioner Jon Gettman noted, "Cannabis is a natural source of dronabinol (THC), the ingredient of Marinol, a Schedule III drug. There are no grounds to schedule cannabis in a more restrictive schedule than Marinol"[71].
At its 33rd meeting, the World Health Organization Expert Committee on Drug Dependence recommended transferring THC to Schedule IV of the Convention, citing its medical uses and low abuse potential. This would put THC in the Convention's least stringently-controlled Schedule.
See also
- Cannabis (drug)
- Psychoactive drug
- Cannabinoids
- Anandamide, 2-Arachidonoylglycerol, endogenous cannabinoid agonists
- Cannabidiol (CBD), an isomer of THC
- Cannabinol (CBN), a metabolite of THC
- HU-210, WIN 55,212-2, JWH-133, synthetic cannabinoid agonists
- Medical cannabis
- War on Drugs
- Cannabis rescheduling in the United States
- Health issues and the effects of cannabis
References
- ↑ "ChemIDplus Lite". chem.sis.nlm.nih.gov. http://chem.sis.nlm.nih.gov/chemidplus/ProxyServlet?objectHandle=Search&actionHandle=getAll3DMViewFiles&nextPage=jsp%2Fcommon%2FChemFull.jsp%3FcalledFrom%3Dlite&chemid=001972083&formatType=_3D. Retrieved 2008-08-08.
- ↑ "Cannabis and Cannabis Extracts: Greater Than the Sum of Their Parts?". www.haworthpress.com. http://www.omma1998.org/McPartland-Russo-JCANT%201(3-4)-2001.pdf. Retrieved 2009-10-22.
- ↑ 3.0 3.1 3.2 3.3 3.4 Grotenhermen F (2003). "Pharmacokinetics and pharmacodynamics of cannabinoids". Clin Pharmacokinet 42 (4): 327–60. doi:10.2165/00003088-200342040-00003. PMID 12648025.
- ↑ 4.0 4.1 Gaoni, Yechiel; Raphael Mechoulam (1964). "Isolation, structure and partial synthesis of an active constituent of hashish" (PDF). Journal of the American Chemical Society 86 (8): 1646–1647. doi:10.1021/ja01062a046. http://pubs.acs.org/cgi-bin/searchRedirect.cgi/jacsat/1964/86/i08/pdf/ja01062a046.pdf. Retrieved 2008-05-31.
- ↑ Interview with the winner of the first ECNP Lifetime Achievement Award: Raphael Mechoulam, Israel February 2007
- ↑ Geller, Tom. (2007)."Cannabinoids: A Secret History", Chemical Heritage Newsmagazine, 25 (2)
- ↑ Pate, D.W. (1994). "Chemical ecology of Cannabis". J. Int. Hemp Assoc 1 (29): 32–37. http://www.kew.org/kbd/detailedresult.do?id=91816.
- ↑ Pate, D.W. (1983). "Possible role of ultraviolet radiation in evolution of Cannabis chemotypes". Economic Botany 37: 396–405. doi:10.1007/BF02904200 (inactive 2009-12-04).
- ↑ Lydon, J; A.H. Teramura (1987). "Photochemical decomposition of cannabidiol in its resin base". Phytochemistry 26: 1216. doi:10.1016/S0031-9422(00)82388-2.
- ↑ Lydon, J; A.H. Teramura, C.B. Coffman (1987). "UV-B radiation effects on photosynthesis, growth and cannabinoid production of two Cannabis sativa chemotypes". Photochem. Photobiol. A 46: 201. doi:10.1111/j.1751-1097.1987.tb04757.x.
- ↑ http://www.incb.org/pdf/e/list/green.pdf
- ↑ Lupica CR, Riegel AC, Hoffman AF (September 2004). "Marijuana and cannabinoid regulation of brain reward circuits". Br. J. Pharmacol. 143 (2): 227–34. doi:10.1038/sj.bjp.0705931. PMID 15313883.
- ↑ "Plant extract may block cannabis addiction" http://www.newscientist.com/article/dn11904-plant-extract-may-block-cannabis-addiction-.html
- ↑ Solinas M, Scherma M, Fattore L, et al. (May 2007). "Nicotinic alpha 7 receptors as a new target for treatment of cannabis abuse". J. Neurosci. 27 (21): 5615–20. doi:10.1523/JNEUROSCI.0027-07.2007. PMID 17522306.
- ↑ Walker JM, Huang SM (August 2002). "Cannabinoid analgesia". Pharmacol. Ther. 95 (2): 127–35. doi:10.1016/S0163-7258(02)00252-8. PMID 12182960. "...to date, there are no deaths known to have resulted from overdose of cannabis. (p. 128)".
- ↑ 16.0 16.1 16.2 16.3 16.4 16.5 16.6 16.7 16.8 Erowid Cannabis Vault : THC Material Safety Data Sheet
- ↑ 17.0 17.1 17.2 17.3 17.4 Erowid. "Cannabis Chemistry". http://www.erowid.org/plants/cannabis/cannabis_chemistry.shtml. Retrieved 2006-03-20.
- ↑ Annas GJ (August 1997). "Reefer madness--the federal response to California's medical-marijuana law". N. Engl. J. Med. 337 (6): 435–9. doi:10.1056/NEJM199708073370621. PMID 9241134.
- ↑ Gable, R.S. (2004). "Comparison of acute lethal toxicity of commonly abused psychoactive substances" (PDF). Addiction 99 (6): 686–696. doi:10.1111/j.1360-0443.2004.00744.x. PMID 15139867. http://web.cgu.edu/faculty/gabler/toxicity%20Addiction%20offprint.pdf.
- ↑ Mechoulam, Raphael (5 June 1970). "Marijuana Chemistry". Science 168 (3936): 1159–1165. doi:10.1126/science.168.3936.1159. PMID 4910003. http://www.sciencemag.org/cgi/content/citation/168/3936/1159. Retrieved 2008-05-31.
- ↑ Mechoulam, Raphael; Arnon Shani, Habib Edery, and Yona Grunfeld (7 August 1970). "Chemical Basis of Hashish Activity". Science 169 (3945): 611–612. doi:10.1126/science.169.3945.611. PMID 4987683. http://www.sciencemag.org/cgi/content/abstract/169/3945/611. Retrieved 2008-05-31.
- ↑ "Marijuana (Cannabis)". National Multiple Sclerosis Society. http://www.nationalmssociety.org/about-multiple-sclerosis/treatments/complementary--alternative-medicine/marijuana/index.aspx. Retrieved 2009-09-05.
- ↑ "Add on Study on Δ9-THC Treatment for Posttraumatic Stress Disorders (PTSD) - Full Text View - ClinicalTrials.gov". http://clinicaltrials.gov/ct2/show/NCT00965809.
- ↑ Müller-Vahl,K.R. Schneider,U. Koblenz,A. Jöbges,M. Kolbe,H. Daldrup,T. Emrich,H.M. (2002). "Treatment of Tourette's Syndrome with Δ9-Tetrahydrocannabinol (THC): A Randomized Crossover Trial". Pharmacopsychiatry 35 (2): 57–61. doi:10.1055/s-2002-25028. PMID 11951146.
- ↑ Müller-Vahl KR, Schneider U, Prevedel H, Theloe K, Kolbe H, Daldrup T, Emrich HM. (April 2003). "Delta 9-tetrahydrocannabinol (THC) is effective in the treatment of tics in Tourette syndrome: a 6-week randomized trial". J Clin Psychiatry 64 (4): 459–65. doi:10.4088/JCP.v64n0417. PMID 12716250.
- ↑ Muller-Vahl KR, Prevedel H, Theloe K, Kolbe H, Emrich HM, Schneider U. (February 2003). "Treatment of Tourette syndrome with delta-9-tetrahydrocannabinol (delta 9-THC): no influence on neuropsychological performance". Neuropsychopharmacology 28 (2): 384–388. doi:10.1038/sj.npp.1300047. PMID 12589392.
- ↑ Ramírez BG, Blázquez C, Gómez del Pulgar T, Guzmán M, de Ceballos ML (2005). "Prevention of Alzheimer's disease pathology by cannabinoids: neuroprotection mediated by blockade of microglial activation". J. Neurosci. 25 (8): 1904–13. doi:10.1523/JNEUROSCI.4540-04.2005. PMID 15728830.
- ↑ Eubanks LM, Rogers CJ, Beuscher AE, et al. (2006). "A molecular link between the active component of marijuana and Alzheimer's disease pathology". Mol. Pharm. 3 (6): 773–7. doi:10.1021/mp060066m. PMID 17140265.
- ↑ Munson AE, Harris LS, Friedman MA, Dewey WL, Carchman RA. "Anticancer activity of cannabinoids." Journal of the National Cancer Institute. September 1975;55(3):597-602. Accessed 2007-10-27.
- ↑ Preet A, Ganju RK, Groopman JE (January 2008). "Delta9-Tetrahydrocannabinol inhibits epithelial growth factor-induced lung cancer cell migration in vitro as well as its growth and metastasis in vivo". Oncogene 27 (3): 339–46. doi:10.1038/sj.onc.1210641. PMID 17621270.
- ↑ Guzmán M, Duarte MJ, Blázquez C, et al. (July 2006). "A pilot clinical study of Delta9-tetrahydrocannabinol in patients with recurrent glioblastoma multiforme". Br. J. Cancer 95 (2): 197–203. doi:10.1038/sj.bjc.6603236. PMID 16804518.
- ↑ Chan PC, Sills RC, Braun AG, Haseman JK, Bucher JR (1996). "Toxicity and carcinogenicity of delta 9-tetrahydrocannabinol in Fischer rats and B6C3F1 mice". Fundamental and applied toxicology : official journal of the Society of Toxicology 30 (1): 109–17. doi:10.1006/faat.1996.0048. PMID 8812248.
- ↑ Hampson AJ, Grimaldi M, Axelrod J, Wink D (July 1998). "Cannabidiol and (-)Delta9-tetrahydrocannabinol are neuroprotective antioxidants". Proceedings of the National Academy of Sciences of the United States of America 95 (14): 8268–73. doi:10.1073/pnas.95.14.8268. PMID 9653176. PMC 20965. http://www.pnas.org/cgi/pmidlookup?view=long&pmid=9653176.
- ↑ Steffens S, Veillard NR, Arnaud C, et al. (2005). "Low dose oral cannabinoid therapy reduces progression of atherosclerosis in mice". Nature 434 (7034): 782–6. doi:10.1038/nature03389. PMID 15815632.
- ↑ Sid Kirchheimer (July 1, 2003). "Heavy Marijuana Use Doesn't Damage Brain". WebMD Medical News. http://www.webmd.com/mental-health/news/20030701/heavy-marijuana-use-doesnt-damage-brain.
- ↑ Jiang, W.; Zhang, Y.; Xiao, L.; Van Cleemput, J.; Ji, S.P.; Bai, G.; Zhang, X. (2005). "Cannabinoids promote embryonic and adult hippocampus neurogenesis and produce anxiolytic-and …". Journal of Clinical Investigation (American Society for Clinical Investigation) 115 (11): 3104. doi:10.1172/JCI25509. PMID 16224541. PMC 1253627. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1253627.
- ↑ Sarne, Y.; Mechoulam, R. (2005). "Cannabinoids: Between Neuroprotection and Neurotoxicity". Current Drug Targets-Cns and Neurological Disorders- 4 (6): 677. doi:10.2174/156800705774933005. PMID 16375685. http://www.ingentaconnect.com/content/ben/cdtcnsnd/2005/00000004/00000006/art00008.
- ↑ Correa, F.; Mestre, L.; Molina-holgado, E.; Arevalo-martin, A.; Docagne, F.; Romero, E.; Molina-holgado, F.; Borrell, J.; Guaza, C. (2005). "The Role of Cannabinoid System on Immune Modulation: Therapeutic Implications on CNS Inflammation". Mini Rev Med Chem 5 (7): 671–5. doi:10.2174/1389557054368790. PMID 16026313. http://www.ingentaconnect.com/content/ben/mrmc/2005/00000005/00000007/art00008.
- ↑ Fernández-ruiz, J.; Romero, J.; Velasco, G.; Tolón, R.M.; Ramos, J.A.; Guzmán, M. (2007). "Cannabinoid CB2 receptor: A new target for controlling neural cell survival?". Trends in Pharmacological Sciences 28 (1): 39–45. doi:10.1016/j.tips.2006.11.001. PMID 17141334. http://linkinghub.elsevier.com/retrieve/pii/S0165614706002677.
- ↑ http://www.tocris.com/pdfs/cannabinoid_receptor_review/page_003.html
- ↑ Bartholomew J, Holroyd S, Heffernan TM (October 2009). "Does cannabis use affect prospective memory in young adults?". J. Psychopharmacol. (Oxford) 24 (2): 241–6. doi:10.1177/0269881109106909. PMID 19825904.
- ↑ Indlekofer F, Piechatzek M, Daamen M, et al. (July 2009). "Reduced memory and attention performance in a population-based sample of young adults with a moderate lifetime use of cannabis, ecstasy and alcohol". J. Psychopharmacol. (Oxford) 23 (5): 495–509. doi:10.1177/0269881108091076. PMID 18635709.
- ↑ Block RI, O'Leary DS, Hichwa RD, et al. (May 2002). "Effects of frequent marijuana use on memory-related regional cerebral blood flow". Pharmacol. Biochem. Behav. 72 (1-2): 237–50. doi:10.1016/S0091-3057(01)00771-7. PMID 11900794.
- ↑ Moore TH, Zammit S, Lingford-Hughes A, et al. (July 2007). "Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review". Lancet 370 (9584): 319–28. doi:10.1016/S0140-6736(07)61162-3. PMID 17662880.
- ↑ Henquet C, Krabbendam L, Spauwen J, et al. (January 2005). "Prospective cohort study of cannabis use, predisposition for psychosis, and psychotic symptoms in young people". BMJ 330 (7481): 11. doi:10.1136/bmj.38267.664086.63. PMID 15574485.
- ↑ Caspi A, Moffitt TE, Cannon M, et al. (May 2005). "Moderation of the effect of adolescent-onset cannabis use on adult psychosis by a functional polymorphism in the catechol-O-methyltransferase gene: longitudinal evidence of a gene X environment interaction". Biol. Psychiatry 57 (10): 1117–27. doi:10.1016/j.biopsych.2005.01.026. PMID 15866551.
- ↑ Arseneault, Louise; Cannon, Mary; Witton, John; Murray, Robin M. (2004). "Causal association between cannabis and psychosis: examination of the evidence". The British Journal of Psychiatry 184 (2): 110–117. doi:10.1192/bjp.184.2.110. PMID 14754822. http://bjp.rcpsych.org/cgi/content/full/184/2/110.
- ↑ Laqueille, X. (September 2009). "Is cannabis a vulnerability factor in schizophrenic disorders" (in French). Arch Pediatr. (Elsevier) 16 (9): 1302–5. doi:10.1016/j.arcped.2009.03.016. PMID 19640690.
- ↑ Kawohl W, Rössler W. (2008). "[Cannabis and Schizophrenia: new findings in an old debate]" (in German). Neuropsychiatr 22 (4): 223–9. PMID 19080993.
- ↑ Degenhardt L, Hall W, Lynskey M (2001) (PDF). Comorbidity between cannabis use and psychosis: Modelling some possible relationships.. Technical Report No. 121.. Sydney: National Drug and Alcohol Research Centre.. http://ndarc.med.unsw.edu.au/NDARCWeb.nsf/resources/TR_18/$file/TR.121.PDF. Retrieved 2006-08-19.
- ↑ Coulston CM, Perdices M, Tennant CC (November 2007). "The neuropsychological correlates of cannabis use in schizophrenia: lifetime abuse/dependence, frequency of use, and recency of use". Schizophr. Res. 96 (1-3): 169–84. doi:10.1016/j.schres.2007.08.006. PMID 17826035.
- ↑ Jayanthi S, Buie S, Moore S, et al. (May 2008). "Heavy marijuana users show increased serum apolipoprotein C-III levels: evidence from proteomic analyses". Mol. Psychiatry 15 (1): 101–12. doi:10.1038/mp.2008.50. PMID 18475272.
- ↑ Dunham, Will (May 13, 2008). "Marijuana may up heart attack, stroke risk: study". Reuters. http://www.reuters.com/article/healthNews/idUSN1231013620080513. Retrieved 2009-09-05.
- ↑ Yücel M; et al. (2008). "Regional brain abnormalities associated with long-term heavy cannabis use". Arch Gen Psychiatry 65 (6): 694–701. doi:10.1001/archpsyc.65.6.694. PMID 18519827.
- ↑ Chang, L.; Yakupov, R.; Cloak, C.; Ernst, T. (2006). "Marijuana use is associated with a reorganized visual-attention network and cerebellar hypoactivation.". Brain 129 (5): 1096. doi:10.1093/brain/awl064. PMID 16585053. http://brain.oxfordjournals.org/cgi/content/full/129/5/1096.
- ↑ Ellgren, Maria (9 Feb 2007) (in English and Swedish). Neurobiological effects of early life cannabis exposure in relation to the gateway hypothesis. Stockholm. ISBN 978-91-7357-064-0. http://diss.kib.ki.se/2007/978-91-7357-064-0/.
- ↑ Ellgren M, Spano SM, Hurd YL (2007). "Adolescent cannabis exposure alters opiate intake and opioid limbic neuronal populations in adult rats". Neuropsychopharmacology 32 (3): 607–15. doi:10.1038/sj.npp.1301127. PMID 16823391.
- ↑ Darke S, Duflou J, Torok M (2009). "Drugs and violent death: comparative toxicology of homicide and non-substance toxicity suicide victims.". Addiction 104 (6): 1000–5. doi:10.1111/j.1360-0443.2009.02565.x. PMID 19466923.
- ↑ Price C, Hemmingsson T, Lewis G, Zammit S, Allebeck P (December 2009). "Cannabis and suicide: longitudinal study". Br J Psychiatry 195 (6): 492–7. doi:10.1192/bjp.bp.109.065227. PMID 19949196.
- ↑ Fellermeier M, Zenk MH (May 1998). "Prenylation of olivetolate by a hemp transferase yields cannabigerolic acid, the precursor of tetrahydrocannabinol". FEBS Lett. 427 (2): 283–5. doi:10.1016/S0014-5793(98)00450-5. PMID 9607329.
- ↑ Huestis MA (2005). "Pharmacokinetics and metabolism of the plant cannabinoids, Δ9-tetrahydrocannabinol, cannabidiol and cannabinol". Handb Exp Pharmacol 168 (168): 657–90. doi:10.1007/3-540-26573-2_23. PMID 16596792.
- ↑ R. Baselt, Disposition of Toxic Drugs and Chemicals in Man, 8th edition, Biomedical Publications, Foster City, CA, 2008, pp 1513-1518.
- ↑ http://www.usdoj.gov/dea/ongoing/marinol.html
- ↑ http://arthritis.about.com/cs/medmarijuana/a/marijuanadebate.htm
- ↑ Pickens JT (1981). "Sedative activity of cannabis in relation to its delta'-trans-tetrahydrocannabinol and cannabidiol content". Br. J. Pharmacol. 72 (4): 649–56. PMID 6269680.
- ↑ Burns, Tammy L.; Ineck, Joseph R. (2006). "Cannabinoid Analgesia as a Potential New Therapeutic Option in the Treatment of Chronic Pain". The Annals of Pharmacotherapy 40 (2): 251–260. doi:10.1345/aph.1G217. PMID 16449552. http://www.theannals.com/cgi/content/abstract/40/2/251.
- ↑ http://www.druglibrary.org/schaffer/hemp/medical/marinol1.htm
- ↑ McKim, William A (2002). Drugs and Behavior: An Introduction to Behavioral Pharmacology (5th Edition). Prentice Hall. pp. 400. ISBN 0-13-048118-1.
- ↑ Greenberg, Gary (2005-11-01). "Respectable Reefer". Mother Jones. http://motherjones.com/politics/2005/11/respectable-reefer?page=3. Retrieved 8 April 2010.
- ↑ Calhoun SR, Galloway GP, Smith DE (1998). "Abuse potential of dronabinol (Marinol)". Journal of psychoactive drugs 30 (2): 187–96. PMID 9692381.
- ↑ [1]
Further reading
- Calhoun SR, Galloway GP, Smith DE (1998). "Abuse potential of dronabinol (Marinol)". J Psychoactive Drugs 30 (2): 187–96. PMID 9692381.
- DEA Moves Marinol To Schedule Three, But Leaves Marijuana in Schedule One. The Magic of Sesame Oil, Richard Cowan, MarijuanaNews.Com.
- Petition to Reschedule Cannabis (Marijuana) per 21 CFR §1308.44(b), Filed October 9, 2002 with the DEA by the Coalition for Rescheduling Cannabis.
External links
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||
|
|||||||||||