Simvastatin
 |
|
|---|---|
| Systematic (IUPAC) name | |
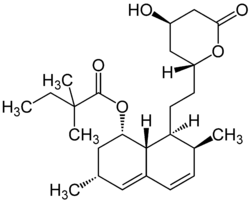
| (1S,3R,7S,8S,8aR)-8-{2-[(2R,4R)-4-hydroxy-6-oxooxan-2-yl]ethyl}-3,7-dimethyl-1,2,3,7,8,8a-hexahydronaphthalen-1-yl 2,2-dimethylbutanoate | |
| Identifiers | |
| CAS number | 79902-63-9 |
| ATC code | C10AA01 |
| PubChem | CID 54454 |
| DrugBank | APRD00104 |
| ChemSpider | 49179 |
| Chemical data | |
| Formula | C25H38O5 |
| Mol. mass | 418.566 g/mol |
| SMILES | eMolecules & PubChem |
| Pharmacokinetic data | |
| Bioavailability | 5% |
| Protein binding | 95% |
| Metabolism | Hepatic (CYP3A4) |
| Half-life | 3 hours |
| Excretion | Renal 13%, faecal 60% |
| Therapeutic considerations | |
| Pregnancy cat. | D(AU) X(US) |
| Legal status | Prescription Only (S4) (AU) P (UK) ℞-only (US) |
| Routes | Oral |
| |
|
Simvastatin (INN) (pronounced /ˈsɪmvəstætɨn/), (marketed under the trade names Zocor, Simlup, Simcard, Simvacor, and others, as well as generically) is a hypolipidemic drug belonging to the class of pharmaceuticals called "statins". It is used to control hypercholesterolemia (elevated cholesterol levels) and to prevent cardiovascular disease. Simvastatin is a synthetic derivate of a fermentation product of Aspergillus terreus.
Contents |
History
The development of simvastatin was closely linked with lovastatin. Biochemist Jesse Huff and his colleagues at Merck began researching the biosynthesis of cholesterol in the early 1950s. In 1956, mevalonic acid was isolated from a yeast extract by Karl Folkers, Carl Hoffman, and others at Merck; while Huff and his associates confirmed that mevalonic acid was an intermediate in cholesterol biosynthesis. In 1959, the HMG-CoA reductase enzyme (a major contributor of internal cholesterol production) was discovered by researchers at the Max Planck Institute. This discovery encouraged scientists worldwide to find an effective inhibitor of this enzyme.
By 1976, Akira Endo had isolated the first inhibitor (Compactin, ML-236B) from the fungus, Penicillium citrinium in Sankyo, Japan.[1] In 1979, Hoffman and colleagues isolated lovastatin from a strain of the fungus Aspergillus terreus. While developing and researching lovastatin, Merck scientists synthetically derived a more potent HMG-CoA reductase inhibitor from a fermentation product of Aspergillus terreus, which was designated MK-733 (later to be named simvastatin).[2]
Uses
Simvastatin is a powerful lipid-lowering drug that can decrease low density lipoprotein (LDL) levels by up to 50%. It is used in doses of 5 mg up to 80 mg. Higher doses (160 mg) have been found to be too toxic, while giving only minimal benefit in terms of lipid lowering. There is also evidence of raising high density lipoprotein (HDL) and lowering triglyceride (TG) levels.
From recent research it has become apparent that simvastatin and other statins inhibit the progression of atherosclerosis beyond their effects on LDL. Many explanations have been proposed, for example its inhibitory effect on macrophages in the atherosclerotic plaque lesions.
In one non-randomized study, simvastatin halved the risk of developing dementia or Parkinson's disease.[3]
Cost / benefit
Since its introduction, there has been a large debate surrounding the price for lipid-lowering treatment and its benefits on atherosclerosis. Although this has affected the other statins as well, simvastatin was the first statin drug to be used extensively in clinical practice.
A number of large epidemiological studies were conducted to discover which patients would benefit most from statin drugs; most studies involve simvastatin as the study drug. The most influential studies were the Scandinavian Simvastatin Survival Study (4S) and the Heart protection study (HPS).
It has now become apparent that patients with one or more risk factors for cardiovascular disease (such as diabetes mellitus, hypertension or a positive family history) can benefit from statins—even if they do not have substantially elevated cholesterol levels.
Simvastatin was introduced in the late 1980s, and in many countries it is now available as a generic preparation. This has led to a decrease of the price of most statin drugs, and a reappraisal of the health economics of preventive statin treatment. In the UK in 2008 the typical per patient cost to the NHS of simvastatin was approx £1.50 per month.
In the UK, simvastatin (in a dose of 10 mg) is available to purchase from pharmacies without prescription.
Pharmacology and dosage
All statins act by inhibiting 3-hydroxy-3-methylglutaryl coenzyme A HMG-CoA reductase, the rate-limiting enzyme of the HMG-CoA reductase pathway, the metabolic pathway responsible for the endogenous production of cholesterol. Statins are more effective than other lipid-regulating drugs at lowering LDL-cholesterol concentration but they are less effective than the fibrates in reducing triglyceride concentration. However, statins reduce cardiovascular disease events and total mortality irrespective of the initial cholesterol concentration.
The drug is in the form of an inactive lactone that is hydrolyzed after ingestion to produce the active agent. It is a white, nonhygroscopic, crystalline powder that is practically insoluble in water, and freely soluble in chloroform, methanol and ethanol.
Usually, patients are started at 20 mg, but the dispersion index can go from 5 mg to 80 mg a day. If adjustments are required, the adjustment must be performed at intervals no less than 4 weeks. The maximum dose must not be more than 80 mg/day.
Interactions
Grapefruit contains furanocoumarins, notably bergamottin and 6',7'-dihydroxybergamottin, which inhibit the intestinal cytochrome P450 3A4 isoform. This in turn slows metabolization of simvastatin and a large number of other drugs resulting in higher plasma levels of the drug. Due to the risk of toxicity patients taking simvastatin should avoid intake of grapefruit and grapefruit-containing products.[4]
On August 8, 2008 FDA issued a warning of the risk of rhabdomyolysis, which can lead to kidney failure or death, when simvastatin is used with amiodarone. This interaction is dose-dependent with simvastatin doses exceeding 20 mg. This drug combination especially with higher doses of simvastatin should be avoided.[5]
Side effects
Common side effects (>1% incidence) may include abdominal pain, diarrhea, indigestion, and a general feeling of weakness. Rare side effects include joint pain, memory loss, and muscle cramps.[6] A type of DNA variant known as a single nucleotide polymorphism (SNP) may help predict individuals prone to developing myopathy when taking simvastatin; a study ultimately including 32,000 patients concluded that carriers of one or two risk alleles of SNP rs4149056 were at 5x or 16x increased risk, respectively.[7]
Marketing
Reference: Drug Discovery Today editorial, 2005.[8]
Simvastatin was initially marketed by Merck & Co under the trade name Zocor, but is now also available generically in most countries following the patent expiry. A combination of simvastatin along with ezetimibe is currently sold under the brand name Vytorin and is jointly marketed by Merck and Schering-Plough.
Brand names include Zocor, Zocor Heart Pro, marketed by the pharmaceutical company Merck & Co. Simlup, Simvotin, Simcard [India], Denan (Germany), Liponorm, Sinvacor, Sivastin (Italy), Lipovas (Japan), Lodales (France), Zocord (Austria and Sweden), Zimstat, Simvahexal (Australia), Lipex (Australia and New Zealand), Simvastatin-Teva, Simvacor, Simvaxon, Simovil (Israel), and others.
The primary U.S. patent for Zocor expired on June 23, 2006. Ranbaxy Laboratories (at the 80-mg strength) and Teva Pharmaceutical Industries through its Ivax Pharmaceuticals unit (at all other strengths) were given approval by the FDA to manufacture and sell simvastatin as a generic drug with 180-day exclusivity. Dr. Reddy's Laboratories also has a license from Merck & Co. to sell simvastatin as an authorized generic drug.
Sales
Prior to losing U.S. patent protection, simvastatin was Merck & Co.'s largest selling drug and second largest selling cholesterol lowering drug in the world; it recorded $4.3 billion of sales in 2005.[8] Zocor had an original patent expiration date of January 2006 but was extended by the United States Patent Trademark Office (PTO) to expire on June 23, 2006. The PTO granted the patent extension after Merck submitted data from studies of the drug’s positive effect on children, a move typically used by drug companies to lengthen exclusivity.[8] In the UK the patent for simvastatin had expired by 2004.
Ordinarily, Merck would have expected a sharp decrease in sales after the generic versions of simvastatin entered the market. However, Merck has slashed the price of Zocor dramatically in an effort to claim sales that would have otherwise gone to the generic versions. At least two major U.S. health insurers, UnitedHealthcare and WellPoint, are now offering Zocor to their members at generic copays.[9]
In addition, since Merck itself manufactures at least some versions of Dr. Reddy's authorized generic simvastatin. Merck is also poised to profit from the Dr. Reddy's version. An 80 mg, 30-count bottle of Dr. Reddy's simvastatin obtained July 6, 2006, states it is made by Merck Sharp & Dohme (Merck & Co.'s name outside the U.S. to avoid conflicts with Merck KGaA) in the UK, just like 80 mg Zocor, and has a Merck & Co. logo on the bottom; except for omitting the "80" on one side, the tablets are visually identical to 80 mg Zocor, including "543" on the other side which is the key part of the National Drug Code for 80 mg Zocor.
See also
- List of drugs affected by grapefruit
References
- ↑ Liao and Laufs. Pleiotropic Effects of Statins.(2005) Annu. Rev. Pharmacol. Toxicol:45:89-118
- ↑ Olivia Williams, Anne-Marie Jacks, Jim Davis, Sabrina Martinez (1998). "Case 10: Merck(A): Mevacor*". In Allan Afuah. Innovation Management - Strategies, Implementation, and Profits. Oxford University Press. ISBN 0195113462. http://www-personal.umich.edu/~afuah/cases/case10.html. Retrieved 2006-07-19.
- ↑ Wolozin, B; Wang SW, Li NC, Lee A, Lee TA, Kazis LE (July 19, 2007). "Simvastatin is associated with a reduced incidence of dementia and Parkinson's disease". BMC Medicine 5: 20. doi:10.1186/1741-7015-5-20. PMID 17640385.
- ↑ National electronic library for medicines[1]
- ↑ "Information on Simvastatin/Amiodarone". http://www.fda.gov/cder/drug/infopage/simvastatin_amiodarone/default.htm. Retrieved 2008-09-21.
- ↑ "Gen-Simvastatin - Drug Factsheets - C-Health". http://chealth.canoe.ca/drug_info_details.asp?channel_id=0&relation_id=0&brand_name_id=3499&page_no=. Retrieved 2007-08-15.
- ↑ SEARCH Collaborative Group,, Group; Link E, Parish S, Armitage J, Bowman L, Heath S, Matsuda F, Gut I, Lathrop M, Collins R (2008). "SLCO1B1 variants and statin-induced myopathy--a genomewide study.". N Engl J Med. 359(8) (8): 789–99. doi:10.1056/NEJMoa0801936. PMID 18650507.
- ↑ 8.0 8.1 8.2 Maggon K (June 2005). "Best-selling human medicines 2002-2004". Drug Discov. Today 10 (11): 739–42. DOI 10.1016/S1359-6446(05)03468-9. PMID 15922927
- ↑ Brin, Dinah Wisenberg (2006-06-22). "Zocor Patent Expiring Means Bidding War". Associated Press. http://biz.yahoo.com/ap/060622/generic_drugs_zocor.html?.v=1. Retrieved 2006-07-09.
External links
|
||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||