Lyme disease
| Lyme Disease | |
|---|---|
| Classification and external resources | |
 Nymphal and adult deer ticks can be carriers of Lyme disease. Nymphs are about the size of a poppy seed. |
|
| ICD-10 | A69.2 |
| ICD-9 | 088.81 |
| DiseasesDB | 1531 |
| MedlinePlus | 001319 |
| eMedicine | med/1346 ped/1331 neuro/521 emerg/588 |
| MeSH | D008193 |
Lyme disease, or lyme borreliosis,[1] is an emerging infectious disease caused by at least three species of bacteria belonging to the genus Borrelia.[2] Borrelia burgdorferi sensu lato[3] is the main cause of Lyme disease in the United States, whereas Borrelia afzelii and Borrelia garinii cause most European cases. The disease is named after the town of Lyme, Connecticut, USA, where a number of cases were identified in 1975. Although Allen Steere realized in 1978 that Lyme disease was a tick-borne disease, the cause of the disease remained a mystery until 1982, when B. burgdorferi was identified by Willy Burgdorfer.
Lyme disease is the most common tick-borne disease in the Northern Hemisphere. Borrelia is transmitted to humans by the bite of infected ticks belonging to a few species of the genus Ixodes ("hard ticks").[4] Early symptoms may include fever, headache, fatigue, depression, and a characteristic circular skin rash called erythema migrans. Left untreated, later symptoms may involve the joints, heart, and central nervous system. In most cases, the infection and its symptoms are eliminated by antibiotics, especially if the illness is treated early. Delayed or inadequate treatment can lead to the more serious symptoms, which can be disabling and difficult to treat.[5] Occasionally, symptoms persist after the infection has been treated with antibiotics, prompting suggestions that Borrelia causes autoimmunity.[6]
Contents |
Signs and symptoms
Lyme disease can affect multiple body systems and produce a range of symptoms. Not all patients with Lyme disease will have all symptoms, and many of the symptoms are not specific to Lyme disease but can occur with other diseases as well. The incubation period from infection to the onset of symptoms is usually one to two weeks, but can be much shorter (days), or much longer (months to years). Symptoms most often occur from May through September, because the nymphal stage of the tick is responsible for most cases.[7] Asymptomatic infection exists, but occurs in less than 7% of infected individuals in the United States.[8] Asymptomatic infection may be much more common among those infected in Europe.[9]
Stage 1: Early localized infection


The classic sign of early local infection with Lyme disease is a circular, outwardly expanding rash called erythema chronicum migrans (also erythema migrans or EM), which occurs at the site of the tick bite three to thirty days after the tick bite.[10][11] The rash is red, and may be warm, but is generally painless. Classically, the innermost portion remains dark red and becomes indurated; the outer edge remains red; and the portion in between clears, giving the appearance of a bullseye. However, partial clearing is uncommon, and the bullseye pattern more often involves central redness.[12]
Erythema migrans is thought to occur in about 80% of infected patients.[11] Patients can also experience flu-like symptoms such as headache, muscle soreness, fever, and malaise.[13] Lyme disease can progress to later stages even in patients who do not develop a rash.[14]
Stage 2: Early disseminated infection
Within days to weeks after the onset of local infection, the borrelia bacteria may begin to spread through the bloodstream. Erythema chronicum migrans may develop at sites across the body that bear no relation to the original tick bite.[15] Another skin condition, which is apparently absent in North American patients but occurs in Europe, is borrelial lymphocytoma, a purplish lump that develops on the ear lobe, nipple, or scrotum.[16] Other discrete symptoms include migrating pain in muscles, joint, and tendons, and heart palpitations and dizziness caused by changes in heartbeat.
Acute neurological problems, which appear in 15% of untreated patients, encompass a spectrum of disorders.[13] These include facial palsy, which is the loss of muscle tone on one or both sides of the face, as well as meningitis, which involves severe headaches, neck stiffness, and sensitivity to light. Radiculoneuritis causes shooting pains that may interfere with sleep as well as abnormal skin sensations. Mild encephalitis may lead to memory loss, sleep disturbances, or mood changes. In addition, some case reports have described altered mental status as the only symptom seen in a few cases of early neuroborreliosis.[17]
Stage 3: Late persistent infection
After several months, untreated or inadequately treated patients may go on to develop severe and chronic symptoms that affect many parts of the body, including the brain, nerves, eyes, joints and heart. Myriad disabling symptoms can occur, including permanent paraplegia in the most extreme cases.[18]
Chronic neurologic symptoms occur in up to 5% of untreated patients.[13] A polyneuropathy that involves shooting pains, numbness, and tingling in the hands or feet may develop. A neurologic syndrome called Lyme encephalopathy is associated with subtle cognitive problems, such as difficulties with concentration and short-term memory. These patients may also experience profound fatigue.[19] However, other problems such as depression and fibromyalgia are no more common in people who have been infected with Lyme than in the general population.[19][20] Chronic encephalomyelitis, which may be progressive, can involve cognitive impairment, weakness in the legs, awkward gait, facial palsy, bladder problems, vertigo, and back pain. In rare cases untreated Lyme disease may cause frank psychosis, which has been mis-diagnosed as schizophrenia or bipolar disorder. Panic attack and anxiety can occur, also delusional behavior, including somatoform delusions, sometimes accompanied by a depersonalization or derealization syndrome, where the person begins to feel detached from themselves or from reality.[21][22]
Lyme arthritis usually affects the knees.[23] In a minority of patients arthritis can occur in other joints, including the ankles, elbows, wrist, hips, and shoulders. Pain is often mild or moderate, usually with swelling at the involved joint. Baker's cysts may form and rupture. In some cases joint erosion occurs.
Acrodermatitis chronica atrophicans (ACA) is a chronic skin disorder observed primarily in Europe among the elderly.[16] ACA begins as a reddish-blue patch of discolored skin, often on the backs of the hands or feet. The lesion slowly atrophies over several weeks or months, with the skin becoming first thin and wrinkled and then, if untreated, completely dry and hairless.[24]
Cause


Lyme disease is caused by Gram-negative spirochetal bacteria from the genus Borrelia. At least 11 Borrelia species have been discovered, 3 of which are known to be Lyme-related.[25][26] The Borrelia species that cause Lyme disease are collectively known as Borrelia burgdorferi sensu lato, and show a great deal of genetic diversity.[27]
The group Borrelia burgdorferi sensu lato is made up of three closely related species that are probably responsible for the large majority of cases: B. burgdorferi sensu stricto (predominant in North America, but also present in Europe), B. afzelii, and B. garinii (both predominant in Eurasia).[25] Some studies have also proposed that B. bissettii and B. valaisiana may sometimes infect humans, but these species do not seem to be important causes of disease.[28][29]
Transmission
Lyme disease is classified as a zoonosis, as it is transmitted to humans from a natural reservoir among rodents by ticks that feed on both sets of hosts.[30] Hard-bodied ticks of the genus Ixodes are the main vectors of Lyme disease.[2] Most infections are caused by ticks in the nymphal stage, as they are very small and may feed for long periods of time undetected.[30] Larval ticks are very rarely infected.[31] Tick bites often go unnoticed because of the small size of the tick in its nymphal stage, as well as tick secretions that prevent the host from feeling any itch or pain from the bite. However, transmission is quite rare, with only about 1% of recognized tick bites resulting in Lyme disease; this may be due to the fact that an infected tick must be attached for at least a day for transmission to occur.[32]
In Europe the vector is Ixodes ricinus, which is also called the sheep tick or castor bean tick.[33] In China Ixodes persulcatus (the taiga tick) is probably the most important vector.[34] In North America, the black-legged tick or deer tick (Ixodes scapularis) is the main vector on the east coast.[31] The lone star tick (Amblyomma americanum), which is found throughout the Southeastern United States as far west as Texas, is unlikely to transmit the Lyme disease spirochete Borrelia burgdorferi,[35] though it may be implicated in a related syndrome called southern tick-associated rash illness, which resembles a mild form of Lyme disease.[36] On the West Coast of the United States, the main vector is the western black-legged tick (Ixodes pacificus).[37] The tendency of this tick species to feed predominantly on host species such as lizards that are resistant to Borrelia infection appears to diminish transmission of Lyme disease in the West.[38][39]
While Lyme spirochetes have been found in insects as well as ticks,[40] reports of actual infectious transmission appear to be rare.[41] Lyme spirochetes have been found in semen[42] and breast milk,[43] however transmission of the spirochete by these routes is not known to occur.[44] Congenital transmission of Lyme disease can occur from an infected mother to fetus through the placenta during pregnancy. The risk for fetal harm is much higher in the first three months of pregnancy than later. Prompt antibiotic treatment almost always prevents fetal harm. Pregnant Lyme-disease patients cannot be treated with the first-choice antibiotic, doxycycline (see below), as it is potentially harmful for the fetus. Instead, erythromycin is usually given; it is less effective against the disease but harmless for the fetus.[45]
Tick-borne co-infections
Ticks that transmit B. burgdorferi to humans can also carry and transmit several other parasites such as Theileria microti and Anaplasma phagocytophilum, which cause the diseases babesiosis and human granulocytic anaplasmosis (HGA), respectively.[46] Among early Lyme disease patients, depending on their location, 2–12% will also have HGA and 2–40% will have babesiosis.[47] Ticks in certain regions, including the landscapes along the Eastern Baltic Sea, also transmit tick-borne encephalitis.[48]
Co-infections complicate Lyme symptoms, especially diagnosis and treatment. It is possible for a tick to carry and transmit one of the co-infections and not Borrelia, making diagnosis difficult and often elusive. The Centers for Disease Control studied 100 ticks in rural New Jersey and found that 55% of the ticks were infected with at least one of the pathogens.[49]
Pathophysiology
Borrelia burgdorferi can spread throughout the body during the course of the disease and has been found in the skin, heart, joint, peripheral nervous system, and central nervous system.[50][51] Many of the signs and symptoms of Lyme disease are a consequence of the immune response to the spirochete in those tissues.[13]
B. burgdorferi is injected into the skin by the bite of an infected Ixodes tick. Tick saliva, which accompanies the spirochete into the skin during the feeding process, contains substances that disrupt the immune response at the site of the bite.[52] This provides a protective environment where the spirochete can establish infection. The spirochetes multiply and migrate outward within the dermis. The host inflammatory response to the bacteria in the skin causes the characteristic circular EM lesion.[50] However neutrophils, which are necessary to eliminate the spirochetes from the skin, fail to appear in the developing EM lesion. This allows the bacteria to survive and eventually spread throughout the body.[53]
Days to weeks following the tick bite, the spirochetes spread via the bloodstream to joints, heart, nervous system, and distant skin sites, where their presence gives rise to the variety of symptoms of disseminated disease. The spread of B. burgdorferi is aided by the attachment of the host protease plasmin to the surface of the spirochete.[54] If untreated, the bacteria may persist in the body for months or even years, despite the production of anti-B. burgdorferi antibodies by the immune system.[32] The spirochetes may avoid the immune response by decreasing expression of surface proteins that are targeted by antibodies, antigenic variation of the VlsE surface protein, inactivating key immune components such as complement, and hiding in the extracellular matrix, which may interfere with the function of immune factors.[55][56]
In the brain B. burgdorferi may induce astrocytes to undergo astrogliosis (proliferation followed by apoptosis), which may contribute to neurodysfunction.[57] The spirochetes may also induce host cells to secrete products toxic to nerve cells, including quinolinic acid and the cytokines IL-6 and TNF-alpha, which can produce fatigue and malaise.[58][59][60] Both microglia and astrocytes secrete IL-6 and TNF-alpha in the presence of the spirochete.[57][61] This cytokine response may contribute to cognitive impairment.[62]
A developing hypothesis is that the chronic secretion of stress hormones as a result of Borrelia infection may reduce the effect of neurotransmitters, or other receptors in the brain by cell-mediated pro-inflammatory pathways, thereby leading to the dysregulation of neurohormones, specifically glucocorticoids and catecholamines, the major stress hormones.[63][64] This process is mediated via the hypothalamic-pituitary-adrenal axis. Additionally tryptophan, a precursor to serotonin appears to be reduced within the central nervous system (CNS) in a number of infectious diseases that affect the brain, including Lyme.[65] Researchers are investigating if this neurohormone secretion is the cause of neuropsychiatric disorders developing in some patients with borreliosis.[66]
Immunological studies
It is possible that exposure to the Borrelia bacterium during Lyme disease causes a long-lived and damaging inflammatory response.[67] This would be a form of pathogen-induced autoimmune disease.[6] The production of this reaction might be due to a form of molecular mimicry, where Borrelia avoid being killed by the immune system by resembling normal parts of the body's tissues.[68][69] It is therefore possible that if some chronic symptoms come from an autoimmune reaction, this could explain why some symptoms persist even after the spirochetes have been eliminated from the body. This hypothesis may explain chronic arthritis that persists after antibiotic therapy, similar to rheumatic fever, but its wider application is controversial.[70][71]
Diagnosis
Lyme disease is diagnosed clinically based on symptoms, objective physical findings (such as erythema migrans, facial palsy, or arthritis), a history of possible exposure to infected ticks, as well as serological blood tests. When making a diagnosis of Lyme disease, health care providers should consider other diseases that may cause similar illness. Most but not all patients with Lyme disease will develop the characteristic bulls-eye rash, but many may not recall a tick bite.[72] Laboratory testing is not recommended for persons who do not have symptoms of Lyme disease.
Because of the difficulty in culturing Borrelia bacteria in the laboratory, diagnosis of Lyme disease is typically based on the clinical exam findings and a history of exposure to endemic Lyme areas.[2] The EM rash, which does not occur in all cases, is considered sufficient to establish a diagnosis of Lyme disease even when serologic blood tests are negative.[73][74] Serological testing can be used to support a clinically suspected case but is not diagnostic by itself.[2]
Diagnosis of late-stage Lyme disease is often difficult because of the multi-faceted appearance which can mimic symptoms of many other diseases. For this reason, a reviewer called Lyme the new "great imitator."[75] Lyme disease may be misdiagnosed as multiple sclerosis, rheumatoid arthritis, fibromyalgia, chronic fatigue syndrome (CFS), lupus, or other autoimmune and neurodegenerative diseases.
Laboratory testing
Several forms of laboratory testing for Lyme disease are available, some of which have not been adequately validated. The most widely used tests are serologies, which measure levels of specific antibodies in a patient's blood. These tests may be negative in early infection, before the body has produced significant quantites of antibody, but they are considered a reliable aid in the diagnosis of later stages of Lyme disease.[76]
The serological laboratory tests most widely available and employed are the Western blot and ELISA. A two-tiered protocol is recommended by the CDC: the sensitive ELISA test is performed first, and if it is positive or equivocal then the more specific Western blot is run.[77] The reliability of testing in diagnosis remains controversial,[2] however studies show the Western blot IgM has a specificity of 94–96% for patients with clinical symptoms of early Lyme disease.[78][79] The initial ELISA test has a sensitivity of about 70%, and in two tiered testing the overall sensitivity is only 64% although this rises to 100% in the subset of people with disseminated symptoms, such as arthritis.[80] However, ELISA testing is typically done against region specific epitopes and may report a false negative if the patient has been infected with Borrelia from another region than that in which they are tested.[81]
Erroneous test results have been widely reported in both early and late stages of the disease. These errors can be caused by several factors, including antibody cross-reactions from other infections including Epstein-Barr virus and cytomegalovirus,[82] as well as herpes simplex virus.[83] The overall rate of false positives is low, only about 1 to 3%, in comparison to a false negative rate of up to 36% using two tiered testing.[80]
Polymerase chain reaction (PCR) tests for Lyme disease have also been developed to detect the genetic material (DNA) of the Lyme disease spirochete. PCR tests are susceptible to false-positive results from poor laboratory technique.[84] Even when properly performed, PCR often shows false-negative results with blood and CSF specimens.[85] Hence PCR is not widely performed for diagnosis of Lyme disease. However PCR may have a role in diagnosis of Lyme arthritis because it is a highly sensitive way of detecting ospA DNA in synovial fluid.[86] With the exception of PCR, there is currently no practical means for detecting the presence of the organism, as serologic studies only test for antibodies of Borrelia. High titers of either immunoglobulin G (IgG) or immunoglobulin M (IgM) antibodies to Borrelia antigens indicate disease, but lower titers can be misleading. This is because the IgM antibodies may remain after the initial infection, and IgG antibodies may remain for years.[87]
Western blot, ELISA and PCR can be performed by either blood test via venipuncture or cerebrospinal fluid (CSF) via lumbar puncture. Though lumbar puncture is more definitive of diagnosis, antigen capture in the CSF is much more elusive; reportedly CSF yields positive results in only 10–30% of patients cultured. The diagnosis of neurologic infection by Borrelia should not be excluded solely on the basis of normal routine CSF or negative CSF antibody analyses.[88]
New techniques for clinical testing of Borrelia infection have been developed, such as LTT-MELISA,[89] which is capable of identifying the active form of Borrelia infection (Lyme disease). Others, such as focus floating microscopy, are under investigation.[90] New research indicates chemokine CXCL13 may also be a possible marker for neuroborreliosis.[91]
Some laboratories offer Lyme disease testing using assays whose accuracy and clinical usefulness have not been adequately established. These tests include urine antigen tests, PCR tests on urine, immunofluorescent staining for cell wall-deficient forms of Borrelia burgdorferi, and lymphocyte transformation tests. The CDC does not recommend these tests and a 2005 review by Aguero-Rosenfeld et al. in Clinical Microbiology Reviews stated that their use is "of great concern and is strongly discouraged".[85]
Imaging
Single photon emission computed tomography (SPECT) imaging has been used to look for cerebral hypoperfusion indicative of Lyme encephalitis in the patient.[92] Although SPECT is not a diagnostic tool itself, it may be a useful method of determining brain function.
In Lyme disease patients, cerebral hypoperfusion of frontal subcortical and cortical structures has been reported.[93] In about 70% of chronic Lyme disease patients with cognitive symptoms, brain SPECT scans typically reveal a pattern of global hypoperfusion in a heterogeneous distribution through the white matter.[94] This pattern is not specific for Lyme disease, since it can also be seen in other central nervous system (CNS) syndromes such as HIV encephalopathy, viral encephalopathy, chronic cocaine use, and vasculitides. However, most of these syndromes can be ruled out easily through standard serologic testing and careful patient history taking.
The presence of global cerebral hypoperfusion deficits on SPECT in the presence of characteristic neuropsychiatric features should dramatically raise suspicion for Lyme encephalopathy among patients who inhabit or have traveled to endemic areas, regardless of patient recall of tick bites. Late disease can occur many years after initial infection. The average time from symptom onset to diagnosis in these patients is about 4 years. Because seronegative disease can occur, and because CSF testing is often normal, Lyme encephalopathy often becomes a diagnosis of exclusion: once all other possibilities are ruled out, Lyme encephalopathy becomes ruled in. Although the aberrant SPECT patterns are caused by cerebral vasculitis, brain biopsy is not commonly performed for these cases as it may be for other types of cerebral vasculitis.
Abnormal magnetic resonance imaging (MRI) findings are often seen in both early and late Lyme disease. MRI scans of patients with neurologic Lyme disease may demonstrate punctuated white matter lesions on T2-weighted images, similar to those seen in demyelinating or inflammatory disorders such as multiple sclerosis, systemic lupus erythematosus (SLE), or cerebrovascular disease.[95] Cerebral atrophy and brainstem neoplasm has been indicated with Lyme infection as well.[96]
Diffuse white matter pathology can disrupt these ubiquitous gray matter connections and could account for deficits in attention, memory, visuospatial ability, complex cognition, and emotional status. White matter disease may have a greater potential for recovery than gray matter disease, perhaps because neuronal loss is less common. Spontaneous remission can occur in multiple sclerosis, and resolution of MRI white matter hyper-intensities, after antibiotic treatment, has been observed in Lyme disease.[97]
Prevention
Attached ticks should be removed promptly, as removal within 36 hours can reduce transmission rates to close to zero.[98] Protective clothing includes a hat and long-sleeved shirts and long trousers that are tucked into socks or boots. Light-colored clothing makes the tick more easily visible before it attaches itself. People should use special care in handling and allowing outdoor pets inside homes because they can bring ticks into the house.
A more effective, communitywide method of preventing Lyme disease is to reduce the numbers of primary hosts on which the deer tick depends, such as rodents, other small mammals, and deer. Reduction of the deer population may over time help break the reproductive cycle of the deer ticks and their ability to flourish in suburban and rural areas.[99]
An unusual, organic approach to control of ticks and prevention of Lyme disease involves the use of domesticated guineafowl. Guineafowl are voracious consumers of insects and arachnids and have a particular fondness for ticks. Localized use of domesticated guineafowl may reduce dependence on chemical pest-control methods.[100]
Management of host animals
Lyme and all other deer-tick-borne diseases can be prevented on a regional level by reducing the deer population that the ticks depend on for reproductive success. This has been demonstrated in the communities of Monhegan, Maine[101] and in Mumford Cove, Connecticut.[102] The black-legged or deer tick (Ixodes scapularis) depends on the white-tailed deer for successful reproduction.
For example, in the US, it is suggested that by reducing the deer population to levels of 8 to 10 per square mile (from the current levels of 60 or more deer per square mile in the areas of the country with the highest Lyme disease rates), the tick numbers can be brought down to levels too low to spread Lyme and other tick-borne diseases.[103] However, such a drastic reduction may be impractical in many areas.
Vaccination
A recombinant vaccine against Lyme disease, based on the outer surface protein A (OspA) of B. burgdorferi, was developed by GlaxoSmithKline. In clinical trials involving more than 10,000 people, the vaccine, called LYMErix, was found to confer protective immunity to Borrelia in 76% of adults and 100% of children with only mild or moderate and transient adverse effects.[104] LYMErix was approved on the basis of these trials by the U.S. Food and Drug Administration (FDA) on December 21, 1998.
Following approval of the vaccine, its entry in clinical practice was slow for a variety of reasons including its cost, which was often not reimbursed by insurance companies.[105] Subsequently, hundreds of vaccine recipients reported that they had developed autoimmune side effects. Supported by some patient advocacy groups, a number of class-action lawsuits were filed against GlaxoSmithKline alleging that the vaccine had caused these health problems. These claims were investigated by the FDA and the U.S. Centers for Disease Control (CDC), who found no connection between the vaccine and the autoimmune complaints.[106]
Despite the lack of evidence that the complaints were caused by the vaccine, sales plummeted and LYMErix was withdrawn from the U.S. market by GlaxoSmithKline in February 2002,[107] in the setting of negative media coverage and fears of vaccine side effects.[106][108] The fate of LYMErix was described in the medical literature as a "cautionary tale";[108] an editorial in Nature cited the withdrawal of LYMErix as an instance in which "unfounded public fears place pressures on vaccine developers that go beyond reasonable safety considerations."[109] The original developer of the OspA vaccine at the Max Planck Institute told Nature: "This just shows how irrational the world can be... There was no scientific justification for the first OspA vaccine [LYMErix] being pulled."[106]
New vaccines are being researched using outer surface protein C (OspC) and glycolipoprotein as methods of immunization.[110][111] Vaccines are available for dogs.[112]
Tick removal
Folk remedies for tick removal tend to be ineffective, offer no advantages in preventing the transfer of disease, and may increase the risks of transmission or infection. The best method is simply to pull the tick out with tweezers as close to the skin as possible, without twisting, and avoiding crushing the body of the tick or removing the head from the body.[113] The risk of infection increases with the time that a tick is attached and if a tick is attached for less than 24 hours infection is unlikely. However, since these ticks are very small, especially in the nymph stage, this makes such prompt detection quite difficult.[98]
Treatment
Antibiotics are the primary treatment for Lyme disease; the most appropriate antibiotic treatment depends upon the patient and the stage of the disease.[2] The antibiotics of choice are doxycycline (in adults), amoxicillin (in children), erythromycin (for pregnant women) and ceftriaxone, with treatment lasting 14 to 28 days.[114] Alternative choices are cefuroxime and cefotaxime.[2] Treatment of pregnant women is similar, but tetracycline should not be used.[114]
A double blind, randomized, placebo-controlled multicenter clinical study indicated that 3 weeks of treatment with intravenous ceftriaxone, followed by 100 days of treatment with oral amoxicillin did not improve symptoms any more than just 3 weeks of treatment with ceftriaxone. The researchers noted that the outcome should not be evaluated after the initial antibiotic treatment but rather 6–12 months afterwards. In patients with chronic post-treatment symptoms, persistent positive levels of antibodies did not seem to provide any useful information for further care of the patient.[115]
In later stages, the bacteria disseminate throughout the body and may cross the blood-brain barrier, making the infection more difficult to treat. Late diagnosed Lyme is treated with oral or IV antibiotics, frequently ceftriaxone for a minimum of four weeks. Minocycline is also indicated for neuroborreliosis for its ability to cross the blood-brain barrier.[116]
Post-Lyme disease symptoms and "chronic" Lyme disease
The term "chronic Lyme disease" is often applied to several different sets of patients. One usage refers to people suffering from the symptoms of untreated and disseminated late-stage Lyme disease: arthritis, peripheral neuropathy and/or encephalomyelitis. The term is also applied to people who have had the disease in the past and some symptoms remain after antibiotic treatment, which is also called post-Lyme disease syndrome. A third and controversial use of the term applies to patients with non-specific symptoms such as fatigue who show no objective evidence that they have been infected with Lyme disease in the past, since the standard diagnostic tests for infection are negative.[117][118]
Up to one third of Lyme disease patients who have completed a course of antibiotic treatment continue to have symptoms such as severe fatigue, sleep disturbance, and cognitive difficulties, with these symptoms being severe in about 2% of cases.[5][119] While it is undisputed that these patients can have severe symptoms, the cause of these symptoms and appropriate treatment is controversial. The symptoms may represent "for all intents and purposes" fibromyalgia/chronic fatigue syndrome.[120] A few doctors attribute these symptoms to persistent infection with Borrelia, or coinfections with other tick-borne infections such as Ehrlichia and Babesia.[121][122] Other doctors believe that the initial infection may cause an autoimmune reaction that continues to cause serious symptoms even after the bacteria have been eliminated by antibiotics.[67]
Four randomized controlled trials have been performed in patients who have persisting complaints and a history of Borrelia infection. Some of these patients had evidence of an ongoing Borrelia infection and almost all of them were previously treated with antibiotics. The authors of all four trials concluded that their results did not support long-term antibiotic therapy. Of these four studies,
- two studies showed no benefit from 30 days of IV ceftriaxone and 60 days of oral doxycycline, concluding that "treatment with intravenous and oral antibiotics for 90 days did not improve symptoms more than placebo".[123][124]
- one study showed an improvement only in fatigue after 28 days of IV antibiotics, an effect that was significant only in a group of patients that never had antibiotics previously.[125] The results may have been compromised by unblinding, and detected a large placebo effect.[126] This trials also saw several cases of life-threatening side effects, concluding that "repeated courses of antibiotic treatment are not indicated for persistent symptoms following Lyme disease including those related to fatigue and cognitive dysfunction, particularly in light of the frequency of serious adverse events."
- one study reported an improvement in fatigue in a subset of patients and a transient improvement in cognition after 10 weeks of IV antibiotics, but concluded that the treatment was "not an effective strategy for sustained cognitive improvement."[127][128] These patients had also been ill for many years and had taken many antibiotic courses. Also, this study performed ad hoc statistical analysis[129] and its results were questionably significant.[119]
A non-profit interest group called the International Lyme And Associated Diseases Society (ILADS)[130] argues that persistence of B. burgdorferi may be responsible for manifestations of late Lyme disease symptoms.[131] It has questioned the generalizability and reliability of some of the above trials and the reliability of the current diagnostic tests.[131][122][132] Major US medical authorities, including the Infectious Diseases Society of America, the American Academy of Neurology, and the National Institutes of Health, have stated that there is no convincing evidence that Borrelia is involved in the various symptoms classed as chronic Lyme disease, and advise against long-term antibiotic treatment as ineffective and possibly harmful.[117][133][134][135] There are significant side effects and risks of prolonged antibiotic therapy, and one death has been reported from complications of a 27-month course of intravenous antibiotics for an unsubstantiated diagnosis of "chronic Lyme disease".[136]
Antibiotic treatment is the central pillar in the management of Lyme disease. However, in the late stages of borreliosis, symptoms may persist despite extensive and repeated antibiotic treatment.[137] Although it is possible that these chronic symptoms are due to either autoimmunity or residual bacteria (see immunological studies below), no Borrelia DNA can usually be detected in the joints after antibiotic treatment, which suggests that the arthritis may continue even after the bacteria have been killed.[67] Lyme arthritis that persists after antibiotic treatment may be treated with hydroxychloroquine or methotrexate.[138] Corticosteroid injections into the affected joint are not recommended for any stage of Lyme arthritis.[139]
Patients with chronic neuropathic pain responded well to gabapentin monotherapy with residual pain after intravenous ceftriaxone treatment in a pilot study.[140] Some antibiotics may have a dual effect on Lyme disease, since minocycline and doxycycline have anti-inflammatory effects in addition to their antibiotic actions including anti-inflammatory effects specific to the inflammation caused by Lyme Disease.[141][142] Indeed, minocycline is used in other neurodegenerative and inflammatory disorders such as multiple sclerosis, Parkinson's disease, Huntington's disease, rheumatoid arthritis (RA) and ALS.[143]
Alternative therapies

A number of other alternative therapies have been suggested, though clinical trials have not been conducted, so the therapies are not known to be scientifically sound. For example, the use of hyperbaric oxygen therapy, as in many other diseases, [144] is claimed by CAM enthusiasts as an adjunct to antibiotics for Lyme has been discussed.[145] Though there are no published data from clinical trials to support its use, preliminary results using a mouse model suggest its effectiveness against B. burgdorferi both in vitro and in vivo.[146] Anecdotal clinical research has suggested that antifungal azole medications such as diflucan could be used in the treatment of Lyme, but the use of these drugs has yet to be tested in a controlled study.[147]
Alternative medicine approaches include bee venom because it contains the peptide melittin, which has been shown to exert inhibitory effects on Lyme bacteria in vitro;[148] however, no clinical trials of this treatment have been carried out.
Prognosis
For early cases, prompt treatment is usually curative.[149] However, the severity and treatment of Lyme disease may be complicated due to late diagnosis, failure of antibiotic treatment, and simultaneous infection with other tick-borne diseases (co-infections) including ehrlichiosis, babesiosis, and immune suppression in the patient.
A meta-analysis published in 2005 found that some patients with Lyme disease have fatigue, joint or muscle pain, and neurocognitive symptoms persisting for years despite antibiotic treatment.[5] Patients with late stage Lyme disease have been shown to experience a level of physical disability equivalent to that seen in congestive heart failure.[150] In rare cases, Lyme disease can be fatal.[151]
Epidemiology
Northern hemisphere temperate regions are most endemic for Lyme disease.[152][153]
Africa
In Northern Africa B. burgdorferi sensu lato has been identified in Morocco, Algeria, Egypt and Tunisia.[154][155][156]
Lyme disease in sub-Saharan is presently unknown, but evidence indicates that Lyme disease may occur in humans in this region. The abundance of hosts and tick vectors would favor the establishment of Lyme infection in Africa.[157] In East Africa, two cases of Lyme disease have been reported in Kenya.[158]
Asia
B. burgdorferi sensu lato infested ticks are being found more frequently in Japan, as well as in Northwest China and far eastern Russia.[159][160] Borrelia has been isolated in Mongolia as well.[161]
Australia
In Australia there is no definitive evidence for the existence of B. burgdorferi or for any other tick-borne spirochete that may be responsible for a local syndrome being reported as Lyme disease.[162] Cases of neuroborreliosis have been documented in Australia but are often ascribed to travel to other continents. The existence of Lyme disease in Australia is controversial.
Canada
Due to changing climate the range of ticks able to carry Lyme disease has expanded from a limited area of Ontario to include areas of southern Quebec, Manitoba, northern Ontario, the Maritimes and parts of the Prairie provinces, as well as British Columbia.[163][164][165][166][167]
Europe
In Europe, cases of B. burgdorferi sensu lato infected ticks are found predominantly in central Europe, particularly in Slovenia and Austria, but have been isolated in almost every country on the continent.[168][169] Incidence in Southern Europe, such as Italy and Portugal, is much lower.
South America
In South America tick-borne disease recognition and occurrence is rising. Ticks carrying B. burgdorferi sensu lato, as well as canine and human tick-borne disease, have been reported widely in Brazil, but the subspecies of Borrelia has not yet been defined.[170] The first reported case of Lyme disease in Brazil was made in 1993 in Sao Paulo.[171] B. burgdorferi sensu stricto antigens in patients have been identified in Colombia and Bolivia.
United States

Lyme disease is the most common tick-borne disease in North America and Europe and one of the fastest-growing infectious diseases in the United States. Of cases reported to the United States CDC, the ratio of Lyme disease infection is 7.9 cases for every 100,000 persons. In the ten states where Lyme disease is most common, the average was 31.6 cases for every 100,000 persons for the year 2005.[172]
Although Lyme disease has been reported in 49 of 50 states in the U.S, about 99% of all reported cases are confined to just five geographic areas (New England, Mid-Atlantic, East-North Central, South Atlantic, and West North-Central).[173] New 2008 CDC Lyme case definition guidelines are used to determine confirmed CDC surveillance cases.[174] Effective January 2008, the CDC gives equal weight to laboratory evidence from 1) a positive culture for B. burgdorferi; 2) two-tier testing (ELISA screening and Western Blot confirming); or 3) single-tier IgG (old infection) Western Blot. Previously, the CDC only included laboratory evidence based on (1) and (2) in their surveillance case definition. The case definition now includes the use of Western Blot without prior ELISA screen.
The number of reported cases of the disease have been increasing, as are endemic regions in North America. For example, it had previously been thought that B. burgdorferi sensu lato was hindered in its ability to be maintained in an enzootic cycle in California because it was assumed the large lizard population would dilute the prevalence of B. burgdorferi in local tick populations, but this has since been brought into question as some evidence has suggested that lizards can become infected.[175] Except for one study in Europe,[176] much of the data implicating lizards is based on DNA detection of the spirochete and has not demonstrated that lizards are able to infect ticks feeding upon them.[177][178][179][180] As some experiments suggest lizards are refractory to infection with Borrelia, it appears likely their involvement in the enzootic cycle is more complex and species-specific.[39]
While B. burgdorferi is most associated with ticks hosted by white-tailed deer and white-footed mice, Borrelia afzelii is most frequently detected in rodent-feeding vector ticks, Borrelia garinii and Borrelia valaisiana appear to be associated with birds. Both rodents and birds are competent reservoir hosts for B. burgdorferi sensu stricto. The resistance of a genospecies of Lyme disease spirochetes to the bacteriolytic activities of the alternative complement pathway of various host species may determine its reservoir host association.
History
The evolutionary history of Borrelia burgdorferi genetics has been the subject of recent studies. One study has found that prior to the reforestation that accompanied post colonial farm abandonment in New England and the wholesale migration into the mid-west that occurred during the early 1800s, Lyme disease was present for thousands of years in America and had spread along with its tick hosts from the Northeast to the Midwest.[181] This is confirmed by the writings of Peter Kalm, a Swedish botanist who was sent to America by Linnaeus, and who found the forests of New York "abound" with ticks when he visited in 1749. When Kalm's journey was retraced 100 years later the forests were gone and the Lyme bacterium had probably become isolated to a few pockets along the northeast coast, Wisconsin, and Minnesota.[182] Perhaps the first detailed description of what we now know of as Lyme disease appeared in the writings of Reverend Dr John Walker after a visit to the Island of Jura (Deer Island) off the west coast of Scotland in 1764.[183] He gives a good description both of the symptoms of Lyme disease (with "exquisite pain (in) the interior parts of the limbs") and of the tick vector itself which he describes as a "worm" with a body which is "of a reddish colour and of a compressed shape with a row of feet on each side" that "penetrates the skin". Many people from this area of Great Britain emigrated to North America between 1717 and the end of the eighteenth century. The examination of preserved museum specimens has found Borrelia DNA in an infected Ixodes ricinus tick from Germany that dates back to 1884 and from an infected mouse from Cape Cod that died in 1894.[184]
The early European studies of what is now known as Lyme disease described its skin manifestations. The first study dates to 1883 in Wrocław, Poland (then known as Breslau, Free State of Prussia) where physician Alfred Buchwald described a man who had suffered for 16 years with a degenerative skin disorder now known as acrodermatitis chronica atrophicans. At a 1909 research conference, Swedish dermatologist Arvid Afzelius presented a study about an expanding, ring-like lesion he had observed in an older woman following the bite of a sheep tick. He named the lesion erythema migrans.[185] The skin condition now known as borrelial lymphocytoma was first described in 1911.[186]
Neurological problems following tick bites were recognized starting in the 1920s. French physicians Garin and Bujadoux described a farmer with a painful sensory radiculitis accompanied by mild meningitis following a tick bite. A large ring-shaped rash was also noted, although the doctors did not relate it to the meningoradiculitis. In 1930, the Swedish dermatologist Sven Hellerström was the first to propose that EM and neurological symptoms following a tick bite were related.[187] In the 1940s, German neurologist Alfred Bannwarth described several cases of chronic lymphocytic meningitis and polyradiculoneuritis, some of which were accompanied by erythematous skin lesions.
Carl Lennhoff, who worked at the Karolinska Institute in Sweden, believed that many skin conditions were caused by spirochetes. In 1948, he used a special stain to microscopically observe what he believed were spirochetes in various types of skin lesions, including EM.[188] Although his conclusions were later shown to be erroneous, interest in the study of spirochetes was sparked. In 1949, Nils Thyresson, who also worked at the Karolinska Institute, was the first to treat ACA with penicillin.[189] In the 1950s, the relationship among tick bite, lymphocytoma, EM and Bannwarth's syndrome was recognized throughout Europe leading to the widespread use of penicillin for treatment in Europe.[190][191]
In 1970 a dermatologist in Wisconsin named Rudolph Scrimenti recognized an EM lesion in a patient after recalling a paper by Hellerström that had been reprinted in an American science journal in 1950. This was the first documented case of EM in the United States. Based on the European literature, he treated the patient with penicillin.[192]
The full syndrome now known as Lyme disease was not recognized until a cluster of cases originally thought to be juvenile rheumatoid arthritis was identified in three towns in southeastern Connecticut in 1975, including the towns Lyme and Old Lyme, which gave the disease its popular name.[193] This was investigated by physicians David Snydman and Allen Steere of the Epidemic Intelligence Service, and by others from Yale University. The recognition that the patients in the United States had EM led to the recognition that "Lyme arthritis" was one manifestation of the same tick-borne condition known in Europe.[194]
Before 1976, elements of B. burgdorferi sensu lato infection were called or known as tick-borne meningopolyneuritis, Garin-Bujadoux syndrome, Bannwarth syndrome, Afzelius' disease,[1] Montauk Knee or sheep tick fever. Since 1976 the disease is most often referred to as Lyme disease,[195][196] Lyme borreliosis or simply borreliosis.
In 1980 Steere, et al., began to test antibiotic regimens in adult patients with Lyme disease.[197] In the same year, New York State Health Dept. epidemiologist Jorge Benach provided Willy Burgdorfer, a researcher at the Rocky Mountain Biological Laboratory, with collections of I. dammini [scapularis] from Shelter Island, NY, a known Lyme-endemic area as part of an ongoing investigation of Rocky Mountain spotted fever. In examining the ticks for rickettsiae, Burgdorfer noticed “poorly stained, rather long, irregularly coiled spirochetes.” Further examination revealed spirochetes in 60% of the ticks. Burgdorfer credited his familiarity with the European literature for his realization that the spirochetes might be the “long-sought cause of ECM and Lyme disease.” Benach supplied him with more ticks from Shelter Island and sera from patients diagnosed with Lyme disease. University of Texas Health Science Center researcher Alan Barbour “offered his expertise to culture and immunochemically characterize the organism.” Burgdorfer subsequently confirmed his discovery by isolating from patients with Lyme disease spirochetes identical to those found in ticks.[198] In June 1982 he published his findings in Science, and the spirochete was named Borrelia burgdorferi in his honor.[199]
After the identification of B. burgdorferi as the causative agent of Lyme disease, antibiotics were selected for testing, guided by in vitro antibiotic sensitivities, including tetracycline antibiotics, amoxicillin, cefuroxime axetil, intravenous and intramuscular penicillin and intravenous ceftriaxone.[200][201] The mechanism of tick transmission was also the subject of much discussion. B. burgdorferi spirochetes were identified in tick saliva in 1987, confirming the hypothesis that transmission occurred via tick salivary glands.[202]
Society and culture
Ecology
Urbanization and other anthropogenic factors can be implicated in the spread of Lyme disease to humans. In many areas, expansion of suburban neighborhoods has led to gradual deforestation of surrounding wooded areas and increased border contact between humans and tick-dense areas. Human expansion has also resulted in reduction of predators that hunt deer as well as mice, chipmunks and other small rodents – the primary reservoirs for Lyme disease. As a consequence of increased human contact with host and vector, the likelihood of transmission of the disease has greatly increased.[203][204] Researchers are investigating possible links between global warming and the spread of vector-borne diseases, including Lyme disease.[205]
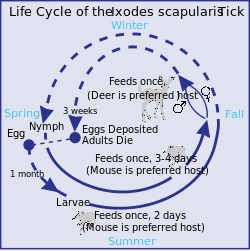
The deer tick (Ixodes scapularis, the primary vector in the northeastern U.S.) has a two-year life cycle, first progressing from larva to nymph, and then from nymph to adult. The tick feeds only once at each stage. In the fall, large acorn forests attract deer as well as mice, chipmunks and other small rodents infected with B. burgdorferi. During the following spring, the ticks lay their eggs. The rodent population then "booms". Tick eggs hatch into larvae, which feed on the rodents; thus the larvae acquire infection from the rodents. At this stage, tick infestation may be controlled using acaricides (miticides).
Adult ticks may also transmit disease to humans. After feeding, female adult ticks lay their eggs on the ground, and the cycle is complete. On the West Coast of the United States, Lyme disease is spread by the western black-legged tick (Ixodes pacificus), which has a different life cycle.
The risk of acquiring Lyme disease does not depend on the existence of a local deer population, as is commonly assumed. New research suggests that eliminating deer from smaller areas (less than 2.5 ha or 6 acres) may in fact lead to an increase in tick density and the rise of "tick-borne disease hotspots".[206]
Controversy and politics
While there is general agreement on the optimal treatment of early Lyme disease, there is considerable controversy over the existence, prevalence, diagnostic criteria, and treatment of "chronic Lyme disease."[130][207] The mainstream view is exemplified by a 2007 review in the New England Journal of Medicine, which noted that the diagnosis of "chronic Lyme disease" is used by a few physicians despite a lack of "reproducible or convincing scientific evidence," leading the authors to describe this diagnosis as "the latest in a series of syndromes that have been postulated in an attempt to attribute medically unexplained symptoms to particular infections."[117] Most medical authorities agree with this viewpoint: the Infectious Diseases Society of America (IDSA), the American Academy of Neurology, the U.S. Centers for Disease Control, and the National Institutes of Health advise against long-term antibiotic treatment for "chronic" Lyme disease, given the lack of supporting evidence and the potential toxicities.[133][134][135]
A minority view holds that chronic Lyme disease is responsible for a range of unexplained symptoms, sometimes in people without any evidence of past infection.[207] This viewpoint is promoted by many patient advocates, notably an advocacy organization[130] called the International Lyme And Associated Diseases Society.[131] Groups of patients, patient advocates, and the small number of physicians who support the concept of chronic Lyme disease have organized to lobby for recognition of this diagnosis, as well as to argue for insurance coverage of long-term antibiotic therapy, which most insurers deny as it is at odds with the guidelines of major medical organizations.[207][208]
In 2006, Richard Blumenthal, the Connecticut Attorney General, opened an antitrust investigation against the IDSA, accusing the IDSA Lyme disease panel of undisclosed conflicts of interest and of unduly dismissing alternative therapies and "chronic" Lyme disease. The investigation was closed on May 1, 2008 without charges when the IDSA agreed to submit to a review of its guidelines by a panel of independent scientists and physicians which would occur on July 30, 2009.[209] Views on the motivation and outcome of the investigation varied. Blumenthal's press release described the agreement as a vindication of his investigation and repeated his conflict-of-interest allegations.[210] The IDSA focused on the fact that the medical validity of the IDSA guidelines was not challenged,[211] and cited mounting legal costs and the difficulty of presenting scientific arguments in a legal setting as their rationale for accepting the settlement.[212] A journalist writing in Nature Medicine suggested that some IDSA members may not have disclosed potential conflicts of interest,[207] while a Forbes piece described Blumenthal's investigation as "intimidation" of scientists by an elected official with close ties to Lyme advocacy groups.[208] The Journal of the American Medical Association described the decision as an example of the "politicization of health policy" that went against the weight of scientific evidence and may have a chilling effect on future decisions by medical associations.[213]
The state of Connecticut went on to enact a law on June 18, 2009 "to allow a licensed physician to prescribe, administer or dispense long-term antibiotics for a therapeutic purpose to a patient clinically diagnosed with Lyme disease."[214] The adjacent state of Rhode Island has a similar law.[215] The expert panel's review was published in 2010, with the independent doctors and scientists in the panel unanimously endorsing the guidelines, stating that "No changes or revisions to the 2006 Lyme guidelines are necessary at this time," and concluding that long-term antibiotic treatments are unproven and potentially dangerous.[216] The ISDA welcomed the final report, stating that "Our number one concern is the patients we treat, and we’re glad patients and their physicians now have additional reassurance that the guidelines are medically sound."[217]
- Harassment of researchers
In 2001, the New York Times Magazine reported that Allen Steere, chief of immunology and rheumatology at Tufts Medical Center and a codiscoverer and leading expert on Lyme disease, had been harassed, stalked, and threatened by patients and patient advocacy groups angry at his refusal to substantiate their diagnoses of "chronic" Lyme disease and endorse long-term antibiotic therapy.[218] Because this intimidation included death threats, Steere was assigned security guards.[106] Paul G. Auwaerter, director of infectious disease at Johns Hopkins School of Medicine, cited the political controversy and high emotions as contributing to a "poisonous atmosphere" around Lyme disease, which he believes has led to doctors trying to avoid having Lyme patients in their practice.[209]
- Media and Internet material
A 2004 study in The Pediatric Infectious Disease Journal stated that 9 of 19 internet websites surveyed contained what were described as major inaccuracies. Websites described as providing inaccurate information included several with the word "lyme" in their domain name (e.g. lymenet.org), as well as the website of the International Lyme And Associated Diseases Society.[219] A 2008 article in the New England Journal of Medicine argued that media coverage of chronic Lyme disease ignored scientific evidence in favor of anecdotes and testimonials:
The media frequently disregard complex scientific data in favor of testimonials about patients suffering from purported chronic Lyme disease and may even question the competence of clinicians who are reluctant to diagnose chronic Lyme disease. All these factors have contributed to a great deal of public confusion with little appreciation of the serious harm caused to many patients who have received a misdiagnosis and have been inappropriately treated.[117]
The 2008 Oscar finalist documentary film Under Our Skin: The Untold Story of Lyme Disease opened June 19, 2009 in New York City. This documentary, made by a director whose sister contracted the disease, argues that chronic lyme disease conditions do exist.[220] Lyme Disease was also the focus of a major feature in The Times (London) in February 2010[221] which detailed the impact the disease had had on British author Alex Wade.
Notable sufferers
- Samantha Stosur - Australian tennis player; contracted in 2007 (affected at the French Open, did not play in 2007 after Wimbledon)
- Amy Tan - Author [222]
- Ben Petrick - Colorado Rockies catcher/outfielder (1999-2003) [223]
- George W. Bush - former United States President[224]
- Wyatt Sexton - Former Quarterback at Florida State University[225]
See also
- List of cutaneous conditions
- Tick-borne disease
- Deer tick
- Erythema migrans
- Rocky mountain spotted fever
Bibliography
- Jonathan A. Edlow MD, Bull's Eye: Unraveling the Medical Mystery of Lyme Disease, Yale University Press, 2003
- Pamela Weintraub, Cure Unknown: Inside the Lyme Disease Epidemic, May 2008. 400 p. St. Martin's Press, hardcover. ISBN 978-0-312-37812-7. MED
References
- ↑ 1.0 1.1 Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 1-4160-2999-0.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 Ryan KJ, Ray CG (editors) (2004). Sherris Medical Microbiology (4th ed.). McGraw Hill. pp. 434–437. ISBN 0838585299.
- ↑ Hu MD, Linden (2009). "Clinical Manifestations of Lyme Disease in Adults". UpToDate. UpToDate.
- ↑ Johnson RC (1996). "Borrelia". Baron's Medical Microbiology (Baron S et al., eds.) (4th ed.). Univ of Texas Medical Branch. ISBN 0-9631172-1-1. http://www.ncbi.nlm.nih.gov/books/bv.fcgi?&rid=mmed.section.1965.
- ↑ 5.0 5.1 5.2 Cairns V, Godwin J (2005). "Post-Lyme borreliosis syndrome: a meta-analysis of reported symptoms". Int J Epidemiol 34 (6): 1340–1345. doi:10.1093/ije/dyi129. PMID 16040645. http://ije.oxfordjournals.org/cgi/content/full/34/6/1340.
- ↑ 6.0 6.1 Singh SK, Girschick HJ (July 2004). "Lyme borreliosis: from infection to autoimmunity". Clin. Microbiol. Infect. 10 (7): 598–614. doi:10.1111/j.1469-0691.2004.00895.x. PMID 15214872.
- ↑ Edlow JA (2007-01-25). "Lyme disease". eMedicine. http://www.emedicine.com/derm/topic536.htm. Retrieved 2007-08-21.
- ↑ Steere AC, Sikand VK, Schoen RT, Nowakowski J (2003). "Asymptomatic infection with Borrelia burgdorferi". Clin. Infect. Dis. 37 (4): 528–532. doi:10.1086/376914. PMID 12905137. http://www.journals.uchicago.edu/doi/full/10.1086/376914.
- ↑ Fahrer H, Sauvain MJ, Zhioua E, Van Hoecke C, Gern LE (1998). "Longterm survey (7 years) in a population at risk for Lyme borreliosis: what happens to the seropositive individuals?". Eur. J. Epidemiol. 14 (2): 117–123. doi:10.1023/A:1007404620701. PMID 9556169.
- ↑ Lyme Disease: eMedicine Ophthalmology. Author: Gerald W Zaidman. http://emedicine.medscape.com/article/1202521-overview Accessed 18th August 2009
- ↑ 11.0 11.1 Fauci, Anthony S. (2008). Harrison's Principles of Internal Medicine: Editors, Anthony S. Fauci ... [Et Al.]. McGraw-Hill Medical Publishing. pp. Chapter 166. ISBN 0-07-159991-6.
- ↑ Smith RP, Schoen RT, Rahn DW, Sikand VK, Nowakowski J, Parenti DL, Holman MS, Persing DH, Steere AC (March 2002). "Clinical characteristics and treatment outcome of early Lyme disease in patients with microbiologically confirmed erythema migrans". Ann. Intern. Med. 136 (6): 421–428. PMID 11900494. http://www.annals.org/cgi/content/full/136/6/421.
- ↑ 13.0 13.1 13.2 13.3 Auwaerter PG, Aucott J, Dumler JS (January 2004). "Lyme borreliosis (Lyme disease): molecular and cellular pathobiology and prospects for prevention, diagnosis and treatment". Expert Rev Mol Med 6 (2): 1–22. doi:10.1017/S1462399404007276. PMID 14987414.
- ↑ Steere AC, Dhar A, Hernandez J, et al. (January 2003). "Systemic symptoms without erythema migrans as the presenting picture of early Lyme disease". Am. J. Med. 114 (1): 58–62. doi:10.1016/S0002-9343(02)01440-7. PMID 12543291. http://linkinghub.elsevier.com/retrieve/pii/S0002934302014407.
- ↑ Dandache P, Nadelman RB (June 2008). "Erythema migrans". Infect. Dis. Clin. North Am. 22 (2): 235–60, vi. doi:10.1016/j.idc.2007.12.012. PMID 18452799.
- ↑ 16.0 16.1 Stanek G, Strle F (June 2008). "Lyme disease: European perspective". Infect. Dis. Clin. North Am. 22 (2): 327–39, vii. doi:10.1016/j.idc.2008.01.001. PMID 18452805.
- ↑ Chabria SB, Lawrason J (2007). "Altered mental status, an unusual manifestation of early disseminated Lyme disease: A case report". Journal of Medical Case Reports 1 (1): 62. doi:10.1186/1752-1947-1-62. PMID 17688693.
- ↑ "Tick disease plea to moor users". BBC News. May 27, 2009. http://news.bbc.co.uk/1/hi/england/south_yorkshire/8070935.stm. Retrieved July 6, 2009.
- ↑ 19.0 19.1 Shadick NA, Phillips CB, Sangha O, et al. (December 1999). "Musculoskeletal and neurologic outcomes in patients with previously treated Lyme disease". Ann. Intern. Med. 131 (12): 919–26. PMID 10610642. http://www.annals.org/cgi/pmidlookup?view=long&pmid=10610642.
- ↑ Seltzer EG, Gerber MA, Cartter ML, Freudigman K, Shapiro ED (February 2000). "Long-term outcomes of persons with Lyme disease". JAMA 283 (5): 609–16. doi:10.1001/jama.283.5.609. PMID 10665700. http://jama.ama-assn.org/cgi/pmidlookup?view=long&pmid=10665700.
- ↑ Fallon BA, Nields JA (1994). "Lyme disease: a neuropsychiatric illness". The American journal of psychiatry 151 (11): 1571–1583. PMID 7943444.
- ↑ Hess A, Buchmann J, Zettl UK, et al. (1999). "Borrelia burgdorferi central nervous system infection presenting as an organic schizophrenia-like disorder". Biol. Psychiatry 45 (6): 795. doi:10.1016/S0006-3223(98)00277-7. PMID 10188012.)
- ↑ Puius YA, Kalish RA (June 2008). "Lyme arthritis: pathogenesis, clinical presentation, and management". Infect. Dis. Clin. North Am. 22 (2): 289–300, vi–vii. doi:10.1016/j.idc.2007.12.014. PMID 18452802.
- ↑ Mullegger RR (2004). "Dermatological manifestations of Lyme borreliosis". Eur J Dermatol 14 (5): 296–309. PMID 15358567. http://www.john-libbey-eurotext.fr/en/revues/medecine/ejd/e-docs/00/04/05/60/article.phtml.
- ↑ 25.0 25.1 Wang G, van Dam AP, Schwartz I, Dankert J (October 1999). "Molecular typing of Borrelia burgdorferi sensu lato: taxonomic, epidemiological, and clinical implications". Clin. Microbiol. Rev. 12 (4): 633–53. PMID 10515907. PMC 88929. http://cmr.asm.org/cgi/pmidlookup?view=long&pmid=10515907.
- ↑ Derdáková M, Lencáková D (2005). "Association of genetic variability within the Borrelia burgdorferi sensu lato with the ecology, epidemiology of Lyme borreliosis in Europe". Ann Agric Environ Med 12 (2): 165–72. PMID 16457468. http://www.aaem.pl/pdf/12165.htm.
- ↑ Bunikis J, Garpmo U, Tsao J, Berglund J, Fish D, Barbour AG (2004). "Sequence typing reveals extensive strain diversity of the Lyme borreliosis agents Borrelia burgdorferi in North America and Borrelia afzelii in Europe" (PDF). Microbiology 150 (Pt 6): 1741–1755. doi:10.1099/mic.0.26944-0. PMID 15184561. http://mic.sgmjournals.org/cgi/reprint/150/6/1741.pdf.
- ↑ Schneider BS, Schriefer ME, Dietrich G, Dolan MC, Morshed MG, Zeidner NS (October 2008). "Borrelia bissettii isolates induce pathology in a murine model of disease". Vector Borne Zoonotic Dis. 8 (5): 623–33. doi:10.1089/vbz.2007.0251. PMID 18454594.
- ↑ Rudenko N, Golovchenko M, Mokrácek A, et al. (October 2008). "Detection of Borrelia bissettii in cardiac valve tissue of a patient with endocarditis and aortic valve stenosis in the Czech Republic". J. Clin. Microbiol. 46 (10): 3540–3. doi:10.1128/JCM.01032-08. PMID 18650352.
- ↑ 30.0 30.1 Tilly K, Rosa PA, Stewart PE (June 2008). "Biology of infection with Borrelia burgdorferi". Infect. Dis. Clin. North Am. 22 (2): 217–34, v. doi:10.1016/j.idc.2007.12.013. PMID 18452798.
- ↑ 31.0 31.1 Lo Re V, Occi JL, MacGregor RR (April 2004). "Identifying the vector of Lyme disease". Am Fam Physician 69 (8): 1935–7. PMID 15117014.
- ↑ 32.0 32.1 Steere AC (July 2001). "Lyme disease". N. Engl. J. Med. 345 (2): 115–25. doi:10.1056/NEJM200107123450207. PMID 11450660.
- ↑ de Mik EL, van Pelt W, Docters-van Leeuwen BD, van der Veen A, Schellekens JF, Borgdorff MW (April 1997). "The geographical distribution of tick bites and erythema migrans in general practice in The Netherlands". Int J Epidemiol 26 (2): 451–7. doi:10.1093/ije/26.2.451. PMID 9169184.
- ↑ Sun Y, Xu R (2003). "Ability of Ixodes persulcatus, Haemaphysalis concinna and Dermacentor silvarum ticks to acquire and transstadially transmit Borrelia garinii". Exp. Appl. Acarol. 31 (1-2): 151–60. doi:10.1023/B:APPA.0000005119.30172.43. PMID 14756409.
- ↑ Ledin KE, et al. (2005). "Borreliacidal activity of saliva of the tick Amblyomma americanum". Med Vet Entomol 19 (1): 90–95. doi:10.1111/j.0269-283X.2005.00546.x. PMID 15752182.
- ↑ Masters EJ, Grigery CN, Masters RW (June 2008). "STARI, or Masters disease: Lone Star tick-vectored Lyme-like illness". Infect. Dis. Clin. North Am. 22 (2): 361–76, viii. doi:10.1016/j.idc.2007.12.010. PMID 18452807.
- ↑ Clark K (2004). "Borrelia species in host-seeking ticks and small mammals in northern Florida" (PDF). J Clin Microbiol 42 (11): 5076–5086. doi:10.1128/JCM.42.11.5076-5086.2004. PMID 15528699. PMC 525154. http://jcm.asm.org/cgi/reprint/42/11/5076.pdf.
- ↑ Eisen L, Eisen RJ, Lane RS (2004). "The roles of birds, lizards, and rodents as hosts for the western black-legged tick Ixodes pacificus". J. Vector Ecol. 29 (2): 295–308. PMID 15709249.
- ↑ 39.0 39.1 Lane RS, Mun J, Eisen L, Eisen RJ (2006). "Refractoriness of the western fence lizard (Sceloporus occidentalis) to the Lyme disease group spirochete Borrelia bissettii". J. Parasitol. 92 (4): 691–696. doi:10.1645/GE-738R1.1. PMID 16995383.
- ↑ Magnarelli L, Anderson J (1988). "Ticks and biting insects infected with the etiologic agent of Lyme disease, Borrelia burgdorferi" (PDF). J Clin Microbiol 26 (8): 1482–1486. PMID 3170711. PMC 266646. http://www.pubmedcentral.gov/picrender.fcgi?artid=266646&blobtype=pdf.
- ↑ Luger S (1990). "Lyme disease transmitted by a biting fly". N Engl J Med 322 (24): 1752. PMID 2342543. http://cassia.org/library/N_Engl_J_Med_1990_Jun_14,322(24),1752.htm.
- ↑ Bach G (2001). "Recovery of Lyme spirochetes by PCR in semen samples of previously diagnosed Lyme disease patients.". 14th International Scientific Conference on Lyme Disease. http://www.anapsid.org/lyme/bach.html.
- ↑ Schmidt B, Aberer E, Stockenhuber C, et al. (1995). "Detection of Borrelia burgdorferi DNA by polymerase chain reaction in the urine and breast milk of patients with Lyme borreliosis". Diagn Microbiol Infect Dis 21 (3): 121–128. doi:10.1016/0732-8893(95)00027-8. PMID 7648832.
- ↑ Steere AC (2003-02-01). "Lyme Disease: Questions and Answers" (PDF). Massachusetts General Hospital / Harvard Medical School. Archived from the original on 2008-03-07. http://web.archive.org/web/20080307191326/http://www.mgh.harvard.edu/medicine/rheu/Q&ALYME.pdf. Retrieved 2009-04-01.
- ↑ Walsh CA, Mayer EW, Baxi LV (2007). "Lyme disease in pregnancy: case report and review of the literature". Obstetrical & gynecological survey 62 (1): 41–50. doi:10.1097/01.ogx.0000251024.43400.9a. PMID 17176487.
- ↑ Swanson SJ, Neitzel D, Reed KD, Belongia EA (October 2006). "Coinfections acquired from ixodes ticks". Clin. Microbiol. Rev. 19 (4): 708–27. doi:10.1128/CMR.00011-06. PMID 17041141.
- ↑ Wormser GP (June 2006). "Clinical practice. Early Lyme disease". N. Engl. J. Med. 354 (26): 2794–801. doi:10.1056/NEJMcp061181. PMID 16807416.
- ↑ Tick-borne encephalitis in Sweden and climate change
- ↑ Varde S, Beckley J, Schwartz I (1998). "Prevalence of tick-borne pathogens in Ixodes scapularis in a rural New Jersey County". Emerging Infect. Dis. 4 (1): 97–9. doi:10.3201/eid0401.980113. PMID 9452402. PMC 2627663. http://www.cdc.gov/ncidod/eid/vol4no1/varde.htm.
- ↑ 50.0 50.1 Steere AC, Coburn J, Glickstein L (April 2004). "The emergence of Lyme disease". J. Clin. Invest. 113 (8): 1093–101. doi:10.1172/JCI21681. PMID 15085185.
- ↑ Pachner AR, Steiner I (June 2007). "Lyme neuroborreliosis: infection, immunity, and inflammation". Lancet Neurol 6 (6): 544–52. doi:10.1016/S1474-4422(07)70128-X. PMID 17509489.
- ↑ Fikrig E, Narasimhan S (April 2006). "Borrelia burgdorferi--traveling incognito?". Microbes Infect. 8 (5): 1390–9. doi:10.1016/j.micinf.2005.12.022. PMID 16698304.
- ↑ Xu Q, Seemanapalli SV, Reif KE, Brown CR, Liang FT (April 2007). "Increasing the recruitment of neutrophils to the site of infection dramatically attenuates Borrelia burgdorferi infectivity". J. Immunol. 178 (8): 5109–15. PMID 17404293. http://www.jimmunol.org/cgi/pmidlookup?view=long&pmid=17404293.
- ↑ Coleman JL, Gebbia JA, Piesman J, Degen JL, Bugge TH, Benach JL (June 1997). "Plasminogen is required for efficient dissemination of B. burgdorferi in ticks and for enhancement of spirochetemia in mice". Cell 89 (7): 1111–9. doi:10.1016/S0092-8674(00)80298-6. PMID 9215633. http://linkinghub.elsevier.com/retrieve/pii/S0092-8674(00)80298-6.
- ↑ Rupprecht TA, Koedel U, Fingerle V, Pfister HW (2008). "The pathogenesis of Lyme neuroborreliosis: from infection to inflammation". Mol. Med. 14 (3-4): 205–12. doi:10.2119/2007-00091.Rupprecht (inactive 2009-09-26). PMID 18097481.
- ↑ Cabello FC, Godfrey HP, Newman SA (August 2007). "Hidden in plain sight: Borrelia burgdorferi and the extracellular matrix". Trends Microbiol. 15 (8): 350–4. doi:10.1016/j.tim.2007.06.003. PMID 17600717.
- ↑ 57.0 57.1 Ramesh G, Alvarez AL, Roberts ED, et al. (September 2003). "Pathogenesis of Lyme neuroborreliosis: Borrelia burgdorferi lipoproteins induce both proliferation and apoptosis in rhesus monkey astrocytes". Eur. J. Immunol. 33 (9): 2539–50. doi:10.1002/eji.200323872. PMID 12938230.
- ↑ Halperin JJ, Heyes MP (January 1992). "Neuroactive kynurenines in Lyme borreliosis". Neurology 42 (1): 43–50. PMID 1531156.
- ↑ "Treatment of Lyme Disease". Columbia University. http://www.columbia-lyme.org/flatp/treatment.html. Retrieved 2007-08-23.
- ↑ Papanicolaou DA, Wilder RL, Manolagas SC, Chrousos GP (1998). "The pathophysiologic roles of interleukin-6 in human disease". Ann. Intern. Med. 128 (2): 127–137. PMID 9441573.
- ↑ Rasley A, Anguita J, Marriott I (2002). "Borrelia burgdorferi induces inflammatory mediator production by murine microglia". J. Neuroimmunol. 130 (1–2): 22–31. doi:10.1016/S0165-5728(02)00187-X. PMID 12225885.
- ↑ Wright CB, Sacco RL, Rundek TR, et al. (2006). "Interleukin-6 is associated with cognitive function: the Northern Manhattan Study". Journal of Stroke and Cerebrovascular Diseases 15 (1): 34–38. doi:10.1016/j.jstrokecerebrovasdis.2005.08.009. PMID 16501663.
- ↑ Elenkov IJ, Iezzoni DG, Daly A, Harris AG, Chrousos GP (2005). "Cytokine dysregulation, inflammation and well-being". Neuroimmunomodulation 12 (5): 255–269. doi:10.1159/000087104. PMID 16166805.
- ↑ Calcagni E, Elenkov I (2006). "Stress system activity, innate and T helper cytokines, and susceptibility to immune-related diseases". Ann. N. Y. Acad. Sci. 1069: 62–76. doi:10.1196/annals.1351.006. PMID 16855135.
- ↑ Gasse T, Murr C, Meyersbach P, et al. (1994). "Neopterin production and tryptophan degradation in acute Lyme neuroborreliosis versus late Lyme encephalopathy". European journal of clinical chemistry and clinical biochemistry : journal of the Forum of European Clinical Chemistry Societies 32 (9): 685–689. PMID 7865624.
- ↑ Zajkowska J, Grygorczuk S, Kondrusik M, Pancewicz S, Hermanowska-Szpakowicz T (2006). "New aspects of pathogenesis of Lyme borreliosis" (in Polish). Przegla̧d epidemiologiczny 60 Suppl 1: 167–170. PMID 16909797.
- ↑ 67.0 67.1 67.2 Ercolini AM, Miller SD (January 2009). "The role of infections in autoimmune disease". Clin. Exp. Immunol. 155 (1): 1–15. doi:10.1111/j.1365-2249.2008.03834.x. PMID 19076824.
- ↑ Oldstone MB (October 1998). "Molecular mimicry and immune-mediated diseases". FASEB J. 12 (13): 1255–65. PMID 9761770. http://www.fasebj.org/cgi/content/full/12/13/1255.
- ↑ Raveche ES, Schutzer SE, Fernandes H, et al. (February 2005). "Evidence of Borrelia autoimmunity-induced component of Lyme carditis and arthritis". J. Clin. Microbiol. 43 (2): 850–6. doi:10.1128/JCM.43.2.850-856.2005. PMID 15695691.
- ↑ Weinstein A, Britchkov M (July 2002). "Lyme arthritis and post-Lyme disease syndrome". Curr Opin Rheumatol 14 (4): 383–7. doi:10.1097/00002281-200207000-00008. PMID 12118171.
- ↑ Bolz DD, Weis JJ (August 2004). "Molecular mimicry to Borrelia burgdorferi: pathway to autoimmunity?". Autoimmunity 37 (5): 387–92. doi:10.1080/08916930410001713098. PMID 15621562.
- ↑ Wormser G, Masters E, Nowakowski J, et al. (2005). "Prospective clinical evaluation of patients from missouri and New York with erythema migrans-like skin lesions". Clin Infect Dis 41 (7): 958–965. doi:10.1086/432935. PMID 16142659.
- ↑ Brown SL, Hansen SL, Langone JJ (1999). "Role of serology in the diagnosis of Lyme disease". JAMA 282 (1): 62–66. doi:10.1001/jama.282.1.62. PMID 10404913.
- ↑ Hofmann H (1996). "Lyme borreliosis—problems of serological diagnosis". Infection 24 (6): 470–472. doi:10.1007/BF01713052. PMID 9007597.
- ↑ Pachner AR (1989). "Neurologic manifestations of Lyme disease, the new "great imitator"". Rev. Infect. Dis. 11 Suppl 6: S1482–1486. PMID 2682960.
- ↑ "Lyme Disease Diagnosis". U.S. Centers for Disease Control. October 7, 2008. http://www.cdc.gov/ncidod/dvbid/lyme/ld_humandisease_diagnosis.htm. Retrieved July 6, 2009.
- ↑ Wilske B (2005). "Epidemiology and diagnosis of Lyme borreliosis". Ann. Med. 37 (8): 568–79. doi:10.1080/07853890500431934. PMID 16338759.
- ↑ Engstrom SM, Shoop E, Johnson RC (1995). "Immunoblot interpretation criteria for serodiagnosis of early Lyme disease" (PDF). J Clin Microbiol 33 (2): 419–427. PMID 7714202. PMC 227960. http://jcm.asm.org/cgi/reprint/33/2/419.pdf.
- ↑ Sivak SL, Aguero-Rosenfeld ME, Nowakowski J, Nadelman RB, Wormser GP (1996). "Accuracy of IgM immunoblotting to confirm the clinical diagnosis of early Lyme disease". Arch Intern Med 156 (18): 2105–2109. doi:10.1001/archinte.156.18.2105. PMID 8862103.
- ↑ 80.0 80.1 Steere AC, McHugh G, Damle N, Sikand VK. (2008). "Prospective study of serologic tests for lyme disease.". Clin Infect Dis. 47 (2): 188–195. doi:10.1086/589242. PMID 18532885. http://www.journals.uchicago.edu/doi/full/10.1086/589242.
- ↑ Wormser GP, Liveris D, Hanincová K, Brisson D, Ludin S, Stracuzzi VJ, Embers ME, Philipp MT, Levin A, Aguero-Rosenfeld M, Schwartz I. (2008). "Effect of Borrelia burgdorferi genotype on the sensitivity of C6 and 2-tier testing in North American patients with culture-confirmed Lyme disease.". Clin Infect Dis. 47 (7): 910–914. doi:10.1086/591529. PMID 18724824.
- ↑ Goossens HA, Nohlmans MK, van den Bogaard AE (1999). "Epstein-Barr virus and cytomegalovirus infections cause false-positive results in IgM two-test protocol for early Lyme borreliosis". Infection 27 (3): 231. doi:10.1007/BF02561539. PMID 10378140.
- ↑ Strasfeld L, Romanzi L, Seder RH, Berardi VP (2005). "False-positive serological test results for Lyme disease in a patient with acute herpes simplex virus type 2 infection". Clin Infect Dis 41 (12): 1826–1827. doi:10.1086/498319. PMID 16288417.
- ↑ Molloy PJ, Persing DH, Berardi VP (2001). "False-positive results of PCR testing for Lyme disease". Clin. Infect. Dis. 33 (3): 412–413. doi:10.1086/321911. PMID 11438915.
- ↑ 85.0 85.1 Aguero-Rosenfeld ME, Wang G, Schwartz I, Wormser GP (2005). "Diagnosis of Lyme borreliosis". Clin. Microbiol. Rev. 18 (3): 484–509. doi:10.1128/CMR.18.3.484-509.2005. PMID 16020686.
- ↑ Nocton JJ, Dressler F, Rutledge BJ, Rys PN, Persing DH, Steere AC (1994). "Detection of Borrelia burgdorferi DNA by polymerase chain reaction in synovial fluid from patients with Lyme arthritis". N. Engl. J. Med. 330 (4): 229–234. doi:10.1056/NEJM199401273300401. PMID 8272083.
- ↑ Burdash N, Fernandes J (1 June 1991). "Lyme borreliosis: detecting the great imitator". The Journal of the American Osteopathic Association 91 (6): 573–574, 577–578. PMID 1874654. http://www.jaoa.org/cgi/content/abstract/91/6/573.
- ↑ Coyle PK, Schutzer SE, Deng Z, et al. (1995). "Detection of Borrelia burgdorferi-specific antigen in antibody-negative cerebrospinal fluid in neurologic Lyme disease". Neurology 45 (11): 2010–2015. PMID 7501150.
- ↑ Valentine-Thon E, Ilsemann K, Sandkamp M (2007). "A novel lymphocyte transformation test (LTT-MELISA) for Lyme borreliosis". Diagn. Microbiol. Infect. Dis. 57 (1): 27–34. doi:10.1016/j.diagmicrobio.2006.06.008. PMID 16876371.
- ↑ Eisendle K, Grabner T, Zelger B (2007). "Focus floating microscopy: "gold standard" for cutaneous borreliosis?". Am. J. Clin. Pathol. 127 (2): 213–222. doi:10.1309/3369XXFPEQUNEP5C. PMID 17210530.
- ↑ Cadavid D (2006). "The mammalian host response to borrelia infection". Wien. Klin. Wochenschr. 118 (21–22): 653–658. doi:10.1007/s00508-006-0692-0. PMID 17160603.
- ↑ Sumiya H, Kobayashi K, Mizukoshi C, et al. (1997). "Brain perfusion SPECT in Lyme neuroborreliosis". J. Nucl. Med. 38 (7): 1120–1122. PMID 9225802.
- ↑ Logigian EL, Johnson KA, Kijewski MF, et al. (1997). "Reversible cerebral hypoperfusion in Lyme encephalopathy". Neurology 49 (6): 1661–1670. PMID 9409364.
- ↑ Fallon BA, Das S, Plutchok JJ, Tager F, Liegner K, Van Heertum R (1997). "Functional brain imaging and neuropsychological testing in Lyme disease". Clin. Infect. Dis. 25 Suppl 1: S57–63. doi:10.1086/516175. PMID 9233666.
- ↑ Fallon, BA (2000). "Review of Lyme Neuroborreliosis". 3rd International Scientific Conference on Lyme Disease and other Tick-borne Disorders. http://www.medscape.com/viewarticle/412987.
- ↑ Kalina P, Decker A, Kornel E, Halperin JJ (2005). "Lyme disease of the brainstem". Neuroradiology 47 (12): 903–907. doi:10.1007/s00234-005-1440-2. PMID 16158278.
- ↑ Fallon BA, Keilp J, Prohovnik I, Heertum RV, Mann JJ (2003). "Regional cerebral blood flow and cognitive deficits in chronic Lyme disease". The Journal of neuropsychiatry and clinical neurosciences 15 (3): 326–332. PMID 12928508.
- ↑ 98.0 98.1 Piesman J, Dolan MC (2002). "Protection against Lyme disease spirochete transmission provided by prompt removal of nymphal Ixodes scapularis (Acari: Ixodidae)". J Med Entomol 39 (3): 509–512. doi:10.1603/0022-2585-39.3.509. PMID 12061448.
- ↑ http://www.ct.gov/caes/lib/caes/documents/publications/bulletins/b1010.pdf
- ↑ Duffy, DC; Downer R, Brinkley C (June 1992). "The effectiveness of Helmeted Guineafowl in the control of the deer tick, the vector of Lyme disease" (PDF). The Wilson Bulletin 104 (2): 342–45. http://www.guineafowl.com/fritsfarm/guineas/ticks/tickstudy.pdf.
- ↑ Rand PW, Lubelczyk C, Holman MS, Lacombe EH, Smith RP (2004). "Abundance of Ixodes scapularis (Acari: Ixodidae) after the complete removal of deer from an isolated offshore island, endemic for Lyme Disease". J. Med. Entomol. 41 (4): 779–784. doi:10.1603/0022-2585-41.4.779. PMID 15311475.
- ↑ "Managing Urban Deer in Connecticut, Figure 2, p.4." (PDF). 2nd edition. Connecticut Department of Environmental Protection - Wildlife Division. June 2007. http://www.ct.gov/dep/lib/dep/wildlife/pdf_files/game/urbandeer07.pdf. Retrieved 2008-05-02.
- ↑ Stafford KC (2004). "Tick Management Handbook" (PDF). Connecticut Agricultural Experiment Station and Connecticut Department of Public Health. pp. 46. http://www.ct.gov/caes/lib/caes/documents/special_features/TickHandbook.pdf. Retrieved 2007-08-21.
- ↑ Poland GA, Jacobson RM (March 2001). "The prevention of Lyme disease with vaccine". Vaccine 19 (17-19): 2303–8. doi:10.1016/S0264-410X(00)00520-X. PMID 11257352. http://linkinghub.elsevier.com/retrieve/pii/S0264410X0000520X.
- ↑ "Lukewarm Response To New Lyme Vaccine". New York Times. June 13, 1999. http://query.nytimes.com/gst/fullpage.html?res=9C05E4D71238F930A25755C0A96F958260. Retrieved July 11, 2008.
- ↑ 106.0 106.1 106.2 106.3 Abbott A (February 2006). "Lyme disease: uphill struggle". Nature 439 (7076): 524–5. doi:10.1038/439524a. PMID 16452949.
- ↑ "Sole Lyme Vaccine Is Pulled Off Market". New York Times. February 28, 2002. http://query.nytimes.com/gst/fullpage.html?res=9C00E5D71531F93BA15751C0A9649C8B63. Retrieved July 11, 2008.
- ↑ 108.0 108.1 Nigrovic LE, Thompson KM (January 2007). "The Lyme vaccine: a cautionary tale". Epidemiol. Infect. 135 (1): 1–8. doi:10.1017/S0950268806007096. PMID 16893489.
- ↑ "When a vaccine is safe". Nature 439 (7076): 509. February 2006. doi:10.1038/439509a. PMID 16452935.
- ↑ Earnhart CG, Marconi RT (2007). "An octavalent Lyme disease vaccine induces antibodies that recognize all incorporated OspC type-specific sequences". Hum Vaccin 3 (6): 281–9. PMID 17921702. http://www.landesbioscience.com/journals/hv/abstract.php?id=4661.
- ↑ Pozsgay V, Kubler-Kielb J (2007). "Synthesis of an experimental glycolipoprotein vaccine against Lyme disease". Carbohydr. Res. 342 (3–4): 621–626. doi:10.1016/j.carres.2006.11.014. PMID 17182019.
- ↑ Aldf.com
- ↑ Zeller JL, Burke AE, Glass RM (2007). "JAMA patient page. Lyme disease". JAMA 297 (23): 2664. doi:10.1001/jama.297.23.2664. PMID 17579234. http://jama.ama-assn.org/cgi/content/full/297/23/2664.
- ↑ 114.0 114.1 Bratton RL, Whiteside JW, Hovan MJ, Engle RL, Edwards FD (May 2008). "Diagnosis and treatment of Lyme disease". Mayo Clin. Proc. 83 (5): 566–71. doi:10.4065/83.5.566. PMID 18452688. http://www.mayoclinicproceedings.com/content/83/5/566.long.
- ↑ Oksi J, Nikoskelainen J, Hiekkanen H, et al. (2007). "Duration of antibiotic treatment in disseminated Lyme borreliosis: a double-blind, randomized, placebo-controlled, multicenter clinical study". Eur. J. Clin. Microbiol. Infect. Dis. 26 (8): 571–581. doi:10.1007/s10096-007-0340-2. PMID 17587070.
- ↑ Elewa HF, Hilali H, Hess DC, Machado LS, Fagan SC (April 2006). "Minocycline for short-term neuroprotection". Pharmacotherapy 26 (4): 515–21. doi:10.1592/phco.26.4.515. PMID 16553511.
- ↑ 117.0 117.1 117.2 117.3 Feder HM, Johnson BJ, O'Connell S, et al. (October 2007). "A critical appraisal of "chronic Lyme disease"". N. Engl. J. Med. 357 (14): 1422–30. doi:10.1056/NEJMra072023. PMID 17914043. http://content.nejm.org/cgi/content/full/357/14/1422.
- ↑ "Frequently Asked Questions about Lyme Disease". Infectious Diseases Society of America. October 2006. http://www.idsociety.org/lymediseasefacts.htm. Retrieved June 24, 2008.
- ↑ 119.0 119.1 Halperin, JJ (2008). "Prolonged Lyme disease treatment: Enough is enough". Neurology 70 (13): 986–7. doi:10.1212/01.WNL.0000291407.40667.69. PMID 17928578.
- ↑ Wolfe F (April 2009). "Fibromyalgia wars". J Rheumatol. 36 (4): 679–83. doi:10.3899/jrheum.081180. PMID 19342721.
- ↑ Cameron D, Gaito A, Harris N, et al. (2004 url="http://www.guideline.gov/summary/summary.aspx?doc_id=4836&nbr=3481&string=lyme"). "Evidence-based guidelines for the management of Lyme disease". Expert Rev Anti Infect Ther 2 (1 Suppl): S1–13. doi:10.1586/14789072.2.1.S1. PMID 15581390.
- ↑ 122.0 122.1 Infectious Diseases Society of America: Lyme Disease Review Panel Hearing - Steven Phillips, MD
- ↑ Klempner MS, Hu LT, Evans J, et al. (July 2001). "Two controlled trials of antibiotic treatment in patients with persistent symptoms and a history of Lyme disease". N. Engl. J. Med. 345 (2): 85–92. doi:10.1056/NEJM200107123450202. PMID 11450676. http://content.nejm.org/cgi/pmidlookup?view=short&pmid=11450676&promo=ONFLNS19.
- ↑ Kaplan RF, Trevino RP, Johnson GM, et al. (June 2003). "Cognitive function in post-treatment Lyme disease: do additional antibiotics help?". Neurology 60 (12): 1916–22. PMID 12821733. http://www.neurology.org/cgi/pmidlookup?view=long&pmid=12821733.
- ↑ Krupp LB, Hyman LG, Grimson R, et al. (24 June 2003). "Study and treatment of post Lyme disease (STOP-LD): a randomized double masked clinical trial". Neurology 60 (12): 1923–30. PMID 12821734. http://www.neurology.org/cgi/content/abstract/60/12/1923.
- ↑ Baker, PJ (2008). "Perspectives on “Chronic Lyme Disease”". American Journal of Medicine 121 (7): 562–4. doi:10.1016/j.amjmed.2008.02.013. PMID 18589049.
- ↑ Fallon BA, Keilp JG, Corbera KM, Petkova E, Britton CB, Dwyer E, Slavov I, Cheng J, Dobkin J, Nelson DR, Sackeim HA (March 2008). "A randomized, placebo-controlled trial of repeated IV antibiotic therapy for Lyme encephalopathy". Neurology 70 (13): 992–1003. doi:10.1212/01.WNL.0000284604.61160.2d. PMID 17928580. http://neurology.org/cgi/content/abstract/70/13/992.
- ↑ http://www.medpagetoday.com/InfectiousDisease/GeneralInfectiousDisease/6946
- ↑ Marques A et al. Neurology, 2008.
- ↑ 130.0 130.1 130.2 Tonks A (November 2007). "Lyme wars". BMJ 335 (7626): 910–2. doi:10.1136/bmj.39363.530961.AD. PMID 17974685. PMC 2048873. http://medical.wesrch.com/pdf_file/LYY_1206297464/lyme_wars.pdf.
- ↑ 131.0 131.1 131.2 Stricker RB (July 2007). "Counterpoint: long-term antibiotic therapy improves persistent symptoms associated with Lyme disease". Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 45 (2): 149–57. doi:10.1086/518853. PMID 17578772.
- ↑ Epi-perspectives.com
- ↑ 133.0 133.1 Wormser GP, Dattwyler RJ, Shapiro ED, et al. (November 2006). "The clinical assessment, treatment, and prevention of lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America". Clin. Infect. Dis. 43 (9): 1089–134. doi:10.1086/508667. PMID 17029130. http://www.journals.uchicago.edu/doi/full/10.1086/508667.
- ↑ 134.0 134.1 Halperin JJ, Shapiro ED, Logigian E, Belman AL, Dotevall L, Wormser GP, Krupp L, Gronseth G, Bever CT (2007). "Practice parameter: treatment of nervous system Lyme disease (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology". Neurology 69 (1): 91–102. doi:10.1212/01.wnl.0000265517.66976.28. PMID 17522387. http://www.neurology.org/cgi/content/abstract/01.wnl.0000265517.66976.28v1.
- ↑ 135.0 135.1 ""Chronic Lyme Disease" Fact Sheet". National Institute of Allergy and Infectious Diseases. April 17, 2009. http://www3.niaid.nih.gov/topics/lymeDisease/understanding/chronic.htm.
- ↑ Patel R, Grogg KL, Edwards WD, Wright AJ, Schwenk NM (October 2000). "Death from inappropriate therapy for Lyme disease". Clin. Infect. Dis. 31 (4): 1107–9. doi:10.1086/318138. PMID 11049799. http://www.journals.uchicago.edu/cgi-bin/resolve?CID994157.
- ↑ Oksi J, Marjamäki M, Nikoskelainen J, Viljanen MK (1999). "Borrelia burgdorferi detected by culture and PCR in clinical relapse of disseminated Lyme borreliosis". Ann. Med. 31 (3): 225–232. doi:10.3109/07853899909115982. PMID 10442678.
- ↑ Massarotti EM (2002). "Lyme arthritis". Med. Clin. North Am. 86 (2): 297–309. doi:10.1016/S0025-7125(03)00088-9. PMID 11982303.
- ↑ Steere AC, Angelis SM (October 2006). "Therapy for Lyme arthritis: strategies for the treatment of antibiotic-refractory arthritis". Arthritis Rheum. 54 (10): 3079–86. doi:10.1002/art.22131. PMID 17009226.
- ↑ Weissenbacher S, Ring J, Hofmann H (2005). "Gabapentin for the symptomatic treatment of chronic neuropathic pain in patients with late-stage lyme borreliosis: a pilot study". Dermatology (Basel) 211 (2): 123–127. doi:10.1159/000086441. PMID 16088158.
- ↑ Bernardino AL, Kaushal D, Philipp MT. (2009). "The antibiotics doxycycline and minocycline inhibit the inflammatory responses to the Lyme disease spirochete Borrelia burgdorferi.". J. Infect. Dis. 199 (9): 1379–88.Click here to read. doi:10.1086/597807. PMID 19301981.
- ↑ Webster G, Del Rosso JQ (April 2007). "Anti-inflammatory activity of tetracyclines". Dermatol Clin 25 (2): 133–5, v. doi:10.1016/j.det.2007.01.012. PMID 17430750.
- ↑ Blum D, Chtarto A, Tenenbaum L, Brotchi J, Levivier M (2004). "Clinical potential of minocycline for neurodegenerative disorders". Neurobiol. Dis. 17 (3): 359–366. doi:10.1016/j.nbd.2004.07.012. PMID 15571972.
- ↑ http://www.alternative-two.com/hyperbaric.html
- ↑ Taylor R, Simpson I (2005). "Review of treatment options for Lyme borreliosis". J Chemother 17 Suppl 2: 3–16. PMID 16315580.
- ↑ Pavia C (2003). "Current and novel therapies for Lyme disease". Expert Opin Investig Drugs 12 (6): 1003–1016. doi:10.1517/13543784.12.6.1003. PMID 12783604.
- ↑ Schardt FW (2004). "Clinical effects of fluconazole in patients with neuroborreliosis". Eur. J. Med. Res. 9 (7): 334–336. PMID 15337633.
- ↑ Lubke LL, Garon CF (1997). "The antimicrobial agent melittin exhibits powerful in vitro inhibitory effects on the Lyme disease spirochete". Clin. Infect. Dis. 25 Suppl 1: S48–51. doi:10.1086/516165. PMID 9233664.
- ↑ Krause PJ, Foley DT, Burke GS, Christianson D, Closter L, Spielman A (2006). "Reinfection and relapse in early Lyme disease". Am. J. Trop. Med. Hyg. 75 (6): 1090–1094. PMID 17172372.
- ↑ Klempner MS, Hu LT, Evans J, et al. (2001). "Two controlled trials of antibiotic treatment in patients with persistent symptoms and a history of Lyme disease". N Engl J Med 345 (2): 85–92. doi:10.1056/NEJM200107123450202. PMID 11450676.
- ↑ Fatal cases of Lyme disease reported in the medical literature include:
- Kirsch M, Ruben FL, Steere AC, Duray PH, Norden CW, Winkelstein A (1988). "Fatal adult respiratory distress syndrome in a patient with Lyme disease". JAMA 259 (18): 2737–2739. doi:10.1001/jama.259.18.2737. PMID 3357244.
- Oksi J, Kalimo H, Marttila RJ, et al. (1996). "Inflammatory brain changes in Lyme borreliosis. A report on three patients and review of literature". Brain 119 (Pt 6): 2143–2154. doi:10.1093/brain/119.6.2143. PMID 9010017.
- Waniek C, Prohovnik I, Kaufman MA, Dwork AJ (1995). "Rapidly progressive frontal-type dementia associated with Lyme disease". J Neuropsychiatry Clin Neurosci 7 (3): 345–347. PMID 7580195.
- Cary NR, Fox B, Wright DJ, Cutler SJ, Shapiro LM, Grace AA (1990). "Fatal Lyme carditis and endodermal heterotopia of the atrioventricular node". Postgrad Med J 66 (772): 134–136. doi:10.1136/pgmj.66.772.134. PMID 2349186.
- ↑ Grubhoffer L, Golovchenko M, Vancová M, Zacharovová-Slavícková K, Rudenko N, Oliver JH (2005). "Lyme borreliosis: insights into tick-/host-borrelia relations". Folia Parasitol. 52 (4): 279–294. PMID 16405291.
- ↑ Higgins R (2004). "Emerging or re-emerging bacterial zoonotic diseases: bartonellosis, leptospirosis, Lyme borreliosis, plague". Rev. - Off. Int. Epizoot. 23 (2): 569–581. PMID 15702720.
- ↑ Bouattour A, Ghorbel A, Chabchoub A, Postic D (2004). "Lyme borreliosis situation in North Africa" (in French). Archives de l'Institut Pasteur de Tunis 81 (1–4): 13–20. PMID 16929760.
- ↑ Dsouli N, Younsi-Kabachii H, Postic D, et al. (2006). "Reservoir role of lizard Psammodromus algirus in transmission cycle of Borrelia burgdorferi sensu lato (Spirochaetaceae) in Tunisia". J. Med. Entomol. 43 (4): 737–742. doi:10.1603/0022-2585(2006)43[737:RROLPA]2.0.CO;2. PMID 16892633.
- ↑ Helmy N (2000). "Seasonal abundance of Ornithodoros (O.) savignyi and prevalence of infection with Borrelia spirochetes in Egypt". Journal of the Egyptian Society of Parasitology 30 (2): 607–619. PMID 10946521.
- ↑ Fivaz BH, Petney TN (1989). "Lyme disease—a new disease in southern Africa?". Journal of the South African Veterinary Association 60 (3): 155–158. PMID 2699499.
- ↑ Jowi JO, Gathua SN (2005). "Lyme disease: report of two cases". East African medical journal 82 (5): 267–269. PMID 16119758.
- ↑ Li M, Masuzawa T, Takada N, et al. (1 July 1998). "Lyme disease Borrelia species in northeastern China resemble those isolated from far eastern Russia and Japan". Appl. Environ. Microbiol. 64 (7): 2705–2709. PMID 9647853. PMC 106449. http://aem.asm.org/cgi/content/full/64/7/2705?view=long&pmid=9647853.
- ↑ Masuzawa T (2004). "Terrestrial distribution of the Lyme borreliosis agent Borrelia burgdorferi sensu lato in East Asia". Jpn. J. Infect. Dis. 57 (6): 229–235. PMID 15623946. http://www.nih.go.jp/JJID/57/229.html.
- ↑ Walder G, Lkhamsuren E, Shagdar A, et al. (2006). "Serological evidence for tick-borne encephalitis, borreliosis, and human granulocytic anaplasmosis in Mongolia". Int. J. Med. Microbiol. 296 Suppl 40: 69–75. doi:10.1016/j.ijmm.2006.01.031. PMID 16524782.
- ↑ Piesman J, Stone BF (1991). "Vector competence of the Australian paralysis tick, Ixodes holocyclus, for the Lyme disease spirochete Borrelia burgdorferi". Int. J. Parasitol. 21 (1): 109–111. doi:10.1016/0020-7519(91)90127-S. PMID 2040556.
- ↑ CBC.ca
- ↑ CBC.ca
- ↑ Gov.bc.ca
- ↑ GC.ca
- ↑ "The emergence of Lyme disease in Canada -- Ogden et al. 180 (12): 1221 -- Canadian Medical Association Journal". http://www.cmaj.ca/cgi/content/full/180/12/1221.
- ↑ Eurosurveillance.org
- ↑ Cababstractsplus.org
- ↑ Mantovani E, Costa IP, Gauditano G, Bonoldi VL, Higuchi ML, Yoshinari NH (2007). "Description of Lyme disease-like syndrome in Brazil. Is it a new tick borne disease or Lyme disease variation?". Braz. J. Med. Biol. Res. 40 (4): 443–456. PMID 17401487.
- ↑ Yoshinari NH, Oyafuso LK, Monteiro FG, et al. (1993). "Lyme disease. Report of a case observed in Brazil" (in Portuguese). Revista do Hospital das Clínicas 48 (4): 170–174. PMID 8284588.
- ↑ CDC (2006-10-02). "Reported Cases of Lyme Disease by Year, United States, 1991–2005". http://www.cdc.gov/ncidod/dvbid/lyme/ld_UpClimbLymeDis.htm. Retrieved 2007-08-20.
- ↑ CDC.gov
- ↑ CDC.gov
- ↑ Swanson KI, Norris DE (2007). "Detection of Borrelia burgdorferi DNA in lizards from Southern Maryland". Vector Borne Zoonotic Dis. 7 (1): 42–49. doi:10.1089/vbz.2006.0548. PMID 17417956.
- ↑ Richter D, Matuschka FR (July 2006). "Perpetuation of the Lyme disease spirochete Borrelia lusitaniae by lizards". Appl. Environ. Microbiol. 72 (7): 4627–4632. doi:10.1128/AEM.00285-06. PMID 16820453.
- ↑ Giery ST, Ostfeld RS (June 2007). "The role of lizards in the ecology of Lyme disease in two endemic zones of the northeastern United States". J. Parasitol. 93 (3): 511–517. doi:10.1645/GE-1053R1.1. PMID 17626342.
- ↑ Amore G, Tomassone L, Grego E, et al. (March 2007). "Borrelia lusitaniae in immature Ixodes ricinus (Acari: Ixodidae) feeding on common wall lizards in Tuscany, central Italy". J. Med. Entomol. 44 (2): 303–307. doi:10.1603/0022-2585(2007)44[303:BLIIIR]2.0.CO;2. PMID 17427701.
- ↑ Swanson KI, Norris DE (2007). "Detection of Borrelia burgdorferi DNA in lizards from Southern Maryland". Vector Borne Zoonotic Dis. 7 (1): 42–49. doi:10.1089/vbz.2006.0548. PMID 17417956.
- ↑ Majláthová V, Majláth I, Derdáková M, Víchová B, Pet'ko B (December 2006). "Borrelia lusitaniae and green lizards (Lacerta viridis), Karst Region, Slovakia". Emerging Infect. Dis. 12 (12): 1895–1901. PMID 17326941. http://www.cdc.gov/ncidod/eid/vol12no12/06-0784.htm.
- ↑ Yale University Press release (August 10, 2009)"Lyme bacterium, Once nearly eradicated in U.S.,Rebounded with Forests"
- ↑ Drymon, M.M. (2008)"Disguised as the Devil:How Lyme disease Created Witches and Changed History":51.
- ↑ Summerton N (1995)"Lyme Disease In The Eighteeth Century" British Medical Journal 311 (7018): 1478.
- ↑ Drymon, M.M. (2008)"Disguised as the Devil:How Lyme disease Created Witches and Changed History":52.
- ↑ Afzelius A (1910). "Verhandlungen der Dermatologischen Gesellshaft zu Stockholm" (in German). Archives of Dermatology and Syphilis 101: 100–102.
- ↑ Burckhardt JL (1911). "Zur Frage der Follikel- und Keimzentrenbildung in der Haut" (in German). Frankfurter Zeitschrift fur Pathologie 6: 352–359.
- ↑ Hellerström S (1930). "Erythema chronicum migrans Afzelii" (in German). Archiv Dermatologie and Venereologie (Stockholm) 11: 315–321.
- ↑ Lenhoff C (1948). "Spirochetes in aetiologically obscure diseases". Acta Dermato-Venreol 28: 295–324.
- ↑ Thyresson N (1949). "The penicillin treatment of acrodermatitis atrophicans chronica (Herxheimer)". Acta Derm. Venereol. 29 (6): 572–621. PMID 18140373.
- ↑ Bianchi GE (1950). "Penicillin therapy of lymphocytoma". Dermatologica 100 (4–6): 270–273. PMID 15421023.
- ↑ Paschoud JM (1954). "Lymphocytoma after tick bite" (in German). Dermatologica 108 (4–6): 435–437. PMID 13190934.
- ↑ Scrimenti RJ (1970). "Erythema chronicum migrans". Archives of dermatology 102 (1): 104–105. doi:10.1001/archderm.102.1.104. PMID 5497158.
- ↑ Steere AC (2006). "Lyme borreliosis in 2005, 30 years after initial observations in Lyme, Connecticut". Wien. Klin. Wochenschr. 118 (21–22): 625–633. doi:10.1007/s00508-006-0687-x. PMID 17160599.
- ↑ Sternbach G, Dibble C (1996). "Willy Burgdorfer: Lyme disease". J Emerg Med 14 (5): 631–634. doi:10.1016/S0736-4679(96)00143-6. PMID 8933327.
- ↑ Mast WE, Burrows WM (1976). "Erythema chronicum migrans and "Lyme arthritis"". JAMA 236 (21): 2392. doi:10.1001/jama.236.21.2392d. PMID 989847.
- ↑ Steere AC, Malawista SE, Snydman DR, et al. (1977). "Lyme arthritis: an epidemic of oligoarticular arthritis in children and adults in three connecticut communities". Arthritis Rheum. 20 (1): 7–17. doi:10.1002/art.1780200102. PMID 836338.
- ↑ Steere AC, Hutchinson GJ, Rahn DW, et al. (1983). "Treatment of the early manifestations of Lyme disease". Ann. Intern. Med. 99 (1): 22–26. PMID 6407378.
- ↑ Burgdorfer, W. Discovery of the Lyme Disease Spirochete and Its Relation to Tick Vectors. Yale J Biol Med 57;1984;515-520.
- ↑ PMID 7043737 (PubMed)
Citation will be completed automatically in a few minutes. Jump the queue or expand by hand - ↑ Luft BJ, Volkman DJ, Halperin JJ, Dattwyler RJ (1988). "New chemotherapeutic approaches in the treatment of Lyme borreliosis". Ann. N. Y. Acad. Sci. 539: 352–361. doi:10.1111/j.1749-6632.1988.tb31869.x. PMID 3056203.
- ↑ Dattwyler RJ, Volkman DJ, Conaty SM, Platkin SP, Luft BJ (1990). "Amoxycillin plus probenecid versus doxycycline for treatment of erythema migrans borreliosis". Lancet 336 (8728): 1404–1406. doi:10.1016/0140-6736(90)93103-V. PMID 1978873.
- ↑ Ribeiro JM, Mather TN, Piesman J, Spielman A (1987). "Dissemination and salivary delivery of Lyme disease spirochetes in vector ticks (Acari: Ixodidae)". J. Med. Entomol. 24 (2): 201–205. PMID 3585913.
- ↑ LoGiudice K, Ostfeld R, Schmidt K, Keesing F (2003). "The ecology of infectious disease: effects of host diversity and community composition on Lyme disease risk". Proc Natl Acad Sci USA 100 (2): 567–571. doi:10.1073/pnas.0233733100. PMID 12525705.
- ↑ Patz J, Daszak P, Tabor G, et al. (2004). "Unhealthy landscapes: Policy recommendations on land use change and infectious disease emergence". Environ Health Perspect 112 (10): 1092–1098. PMID 15238283.
- ↑ Khasnis AA, Nettleman MD (2005). "Global warming and infectious disease". Arch. Med. Res. 36 (6): 689–696. doi:10.1016/j.arcmed.2005.03.041. PMID 16216650.
- ↑ Perkins SE, Cattadori IM, Tagliapietra V, Rizzoli AP, Hudson PJ (2006). "Localized deer absence leads to tick amplification". Ecology 87 (8): 1981–1986. doi:10.1890/0012-9658(2006)87[1981:LDALTT]2.0.CO;2. PMID 16937637.
- ↑ 207.0 207.1 207.2 207.3 Ballantyne C (November 2008). "The chronic debate over Lyme disease". Nat. Med. 14 (11): 1135–9. doi:10.1038/nm1108-1135. PMID 18989271.
- ↑ 208.0 208.1 Whelan, David (2007-03-12). "Lyme Inc". Forbes. http://www.forbes.com/business/healthcare/forbes/2007/0312/096.html. Retrieved 2008-06-24.
- ↑ 209.0 209.1 Landers, Susan J (2008-06-09). "Lyme treatment accord ends antitrust probe". American Medical News. http://www.ama-assn.org/amednews/2008/06/09/hlsa0609.htm. Retrieved 2008-06-24.
- ↑ State of Connecticut Attorney General's Office (2008-05-01). "Attorney General's Investigation Reveals Flawed Lyme Disease Guideline Process, IDSA Agrees To Reassess Guidelines, Install Independent Arbiter". Press release. http://www.ct.gov/ag/cwp/view.asp?a=2795&q=414284. Retrieved 2008-06-24.
- ↑ Infectious Diseases Society of America (2008-05-01). "Agreement Ends Lyme Disease Investigation By Connecticut Attorney General: Medical Validity of IDSA Guidelines Not Challenged". Press release. http://www.idsociety.org/Content.aspx?id=11182. Retrieved 2008-06-24.
- ↑ Klein JO (November 2008). "Danger ahead: politics intrude in Infectious Diseases Society of America guideline for Lyme disease". Clin. Infect. Dis. 47 (9): 1197–9. doi:10.1086/592247. PMID 18821849.
- ↑ Kraemer JD, Gostin LO (February 2009). "Science, politics, and values: the politicization of professional practice guidelines". JAMA 301 (6): 665–7. doi:10.1001/jama.301.6.665. PMID 19211474.
- ↑ "An Act Concerning the Use of Long-Term Antibiotics for the Treatment of Lyme Disease.". 2009-06-18. http://www.cga.ct.gov/asp/cgabillstatus/cgabillstatus.asp?selBillType=Bill&bill_num=6200&which_year=2009&SUBMIT1.x=0&SUBMIT1.y=0&SUBMIT1=Normal. Retrieved 2009-07-05.
- ↑ "Lyme Disease and the Law". 2009. http://www.health.state.ri.us/disease/communicable/lyme/law.php. Retrieved 2009-07-05.
- ↑ Stephen Singer (4/22/2010). "No changes to Lyme disease treatment". Associated Press. http://www.msnbc.msn.com/id/36721207/ns/health-infectious_diseases/deck/news.mobile.msn.com/ent.mobile.msn.com/en-us/mny.mobile.msn.com/en-us/.
- ↑ Special Review Panel Unanimously Upholds Lyme Disease Treatment Guidelines: Short-term Antibiotics Proven to be Best Treatment for Patients Infectious Diseases Society of America April 22, 2010
- ↑ Grann, David (2001-06-17). "Stalking Dr. Steere Over Lyme Disease". New York Times Magazine. http://www.nytimes.com/2001/06/17/magazine/17LYMEDISEASE.html. Retrieved 2008-06-25.
- ↑ Cooper JD, Feder HM (December 2004). "Inaccurate information about lyme disease on the internet". Pediatr. Infect. Dis. J. 23 (12): 1105–8. PMID 15626946. http://www.cdc.gov/ncidod/dvbid/lyme/resources/LD_Internet.pdf. Retrieved 2009-07-05.
- ↑ Film Focuses on Lyme Patients, from the Washington Post. Published 17 June 2008; accessed 12 September 2008.
- ↑ Lyme disease: ‘I knew whatever was troubling me wasn’t a sports injury’, from The Times, accessed 23 February 2010
- ↑ http://www.canlyme.com/amy.html
- ↑ http://webcache.googleusercontent.com/search?q=cache:q0OmloepDPYJ:www.georgialymedisease.org/lyme_disease+colorado+rockies+ly+me+disease&cd=3&hl=en&ct=clnk&gl=us
- ↑ Brown, David (2007-08-09). "Bush Apparently Had Lyme Disease". The Washington Post. http://www.washingtonpost.com/wp-dyn/content/article/2007/08/08/AR2007080802268.html.
- ↑ http://sports.espn.go.com/ncf/news/story?id=2104326, ESPN.com, Retrieved August 12, 2010
|
|||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||
External links
- General
- Lyme Disease Map Project
- Lyme disease organizations at the Open Directory Project
- Lyme Disease Institute for Good Medicine at the Pennsylvania Medical Society
- Lyme Disease: from the U.S. Centers for Disease Control
- Lyme Disease Information: from the National Institute of Allergy and Infectious Diseases
- Lyme Disease The Merck Manual
- US Army Factsheet on Lyme Disease (CHPPM's Entomological Sciences Program)
- CTV (Canada) W5 Documentary on Lyme Disease in Canada
- International Lyme and Associated Diseases Society