Tocopherol
| α-Tocopherol[1] | |
|---|---|
 |
|
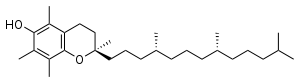
| IUPAC name | (2R)-2,5,7,8-Tetramethyl-2-[(4R,8R)-4,8,12 -trimethyltridecyl]-3,4-dihydro-2H-chromen-6-ol |
| Identifiers | |
| CAS number | 59-02-9 |
| EINECS number | |
| SMILES |
|
| InChI |
|
| Properties | |
| Molecular formula | C29H50O2 |
| Molar mass | 430.69 g/mol |
| Density | 0.950 g/cm³ |
| Melting point |
2.5-3.5 °C |
| Boiling point |
200-220 °C at 0.1 mmHg |
| Except where noted otherwise, data are given for materials in their standard state (at 25 °C, 100 kPa) Infobox references |
|
Tocopherol, a class of chemical compounds of which many have vitamin E activity, describes a series of organic compounds consisting of various methylated phenols. Because the vitamin activity was first identified in 1936 from a dietary fertility factor in rats, it was given the name "tocopherol" from the Greek words “τοκος” [birth], and “φορειν”, [to bear or carry] meaning in sum "to carry a pregnancy," with the ending "-ol" signifying its status as a chemical alcohol.
Tocotrienols, which are related compounds, may also have vitamin E activity. All of these various derivatives with vitamin activity may correctly be referred to as "vitamin E." Tocopherols and tocotrienols are fat-soluble antioxidants.
The compound α-tocopherol, a common form of tocopherol added to food products, is denoted by the E number E307.
Contents |
Forms
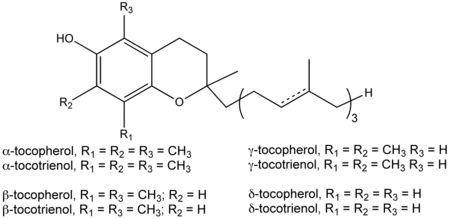
Vitamin E exists in eight different forms, four tocopherols and four tocotrienols. All feature a chromanol ring, with a hydroxyl group that can donate a hydrogen atom to reduce free radicals and a hydrophobic side chain which allows for penetration into biological membranes. Both the tocopherols and tocotrienols occur in alpha, beta, gamma and delta forms, determined by the number of methyl groups on the chromanol ring. Each form has slightly different biological activity.[2]
As a food additive, tocopherol is labeled with these E numbers: E307 (α-tocopherol), E308 (γ-tocopherol), and E309 (δ-tocopherol).
Alpha-tocopherol
Alpha-tocopherol is the form of vitamin E that is preferentially absorbed and accumulated in humans.[3] The measurement of "vitamin E" activity in international units (IU) was based on fertility enhancement by the prevention of spontaneous abortions in pregnant rats relative to alpha-tocopherol.
There are three stereocenters in alpha-tocopherol, so this is a chiral molecule.[4] The eight stereoisomers of alpha-tocopherol differ in the arrangement of groups around these stereocenters. In the image of RRR-alpha-tocopherol below, all three stereocenters are in the R form. However, if the middle of the three stereocenters were changed (so the hydrogen was now pointing down and the methyl group pointing up), this would become the structure of RSR-alpha-tocopherol. RSR-alpha-tocopherol and RRR-alpha-tocopherol are mirror-images of each other. These stereoisomers can also be named in an alternative older nomenclature, where the stereocenters are either in the d or l form.[5]

1 IU of tocopherol is defined as ⅔ milligrams of RRR-alpha-tocopherol (formerly named d-alpha-tocopherol or sometimes ddd-alpha-tocopherol). 1 IU is also defined as 1 milligram of an equal mix of the eight stereoisomers, which is a racemic mixture called all-rac-alpha-tocopheryl acetate. This mix of stereoisomers is often called dl-alpha-tocopheryl acetate, even though it is more precisely dl,dl,dl-alpha-tocopheryl acetate). However, 1 IU of this racemic mixture is not now considered equivalent to 1 IU of natural (RRR) α-tocopherol, and the Institute of Medicine and the USDA now convert IU's of the racemic mixture to milligrams of equivalent RRR using 1 IU racemic mixture = 0.45 "milligrams α-tocopherol".[6]
Other R, R, R tocopherol
The other R, R, R tocopherol vitamins are slowly being recognized as research begins to elucidate their additional roles in the human body. Many naturopathic and orthomolecular medicine advocates suggest that vitamin E supplements contain at least 20% by weight of the other natural vitamin E isomers.
Tocotrienols
Tocotrienols, with four d- isomers, also belong to the vitamin E family. The four tocotrienols have structures corresponding to the four tocopherols, except with an unsaturated bond in each of the three isoprene units that form the hydrocarbon tail. Tocopherols have a saturated phytyl tail.
History
During feeding experiments with rats Herbert McLean Evans concluded in 1922 that besides vitamins B and C, an unknown vitamin existed.[7] Although every other nutrition was present, the rats were not fertile. This condition could be changed by additional feeding with wheat germ. It took several years until 1936 when the substance was isolated from wheat germ and the formula C29H50O2 was determined. Evans also found that the compound reacted like an alcohol and concluded that one of the oxygen atoms was part of an OH (hydroxyl) group. As noted in the introduction, the vitamin was given its name by Evans from Greek words meaning "to bear young" with the addition of the -ol as an alcohol.[8] The structure was determined shortly thereafter in 1938.[9]
Recommended amounts
The U.S. Dietary Reference Intake (DRI) Recommended Daily Amount (RDA) for a 25-year old male for Vitamin E is 15 mg/day. The DRI for vitamin E is based on the alpha-tocopherol form because it is the most active form as originally tested. Results of two national surveys, the National Health and Nutrition Examination Survey (NHANES III 1988-91) and the Continuing Survey of Food Intakes of Individuals (1994 CSFII) indicated that the dietary intakes of most Americans do not provide the recommended amounts of vitamin E. However, a 2000 Institute of Medicine (IOM) report on vitamin E states that intake estimates of vitamin E may be low because energy and fat intake is often underreported in national surveys and because the kind and amount of fat added during cooking is often not known. The IOM states that most North American adults get enough vitamin E from their normal diets to meet current recommendations. However, they do caution individuals who consume low fat diets because vegetable oils are such a good dietary source of vitamin E. "Low-fat diets can substantially decrease vitamin E intakes if food choices are not carefully made to enhance alpha-tocopherol intakes". Vitamin E supplements are absorbed best when taken with meals.[10]
Because vitamin E can act as an anticoagulant and may increase the risk of bleeding problems, many agencies have set an upper tolerable intake level (UL) for vitamin E at 1,000 mg (1,500 IU) per day.[11]
Sources
In foods, the most abundant sources of vitamin E are vegetable oils such as palm oil, sunflower, corn, soybean, and olive oil. Nuts, sunflower seeds, seabuckthorn berries, kiwi fruit, and wheat germ are also good sources. Other sources of vitamin E are whole grains, fish, peanut butter, goats milk, and green leafy vegetables. Fortified breakfast cereals are also an important source of vitamin E in the United States. Although originally extracted from wheat germ oil, most natural vitamin E supplements are now derived from vegetable oils, usually soybean oil.
The content of Vitamin E for rich sources follows:[12]
- Wheat germ oil (215.4 mg/100 g)
- Sunflower oil (55.8 mg/100 g)
- Almond oil (39.2 mg/100 g)
- Hazelnut (26.0 mg/100 g)
- Walnut oil (20.0 mg/100 g)
- Peanut oil (17.2 mg/100 g)
- Olive oil (12.0 mg/100 g)
- Peanut (9.0 mg/100 g)
- Pollard (2.4 mg/100 g)
- Corn (2.0 mg/100 g)
- Asparagus (1.5 mg/100 g)
- Oats (1.5 mg/100 g)
- Chestnut (1.2 mg/100 g)
- Coconut (1.0 mg/100 g)
- Tomatoes (0.9 mg/100 g)
- Carrots (0.6 mg/100 g)
- Goat's milk (0.1 mg/100ml)
Deficiency
Vitamin E deficiency causes neurological problems due to poor nerve conduction. These include neuromuscular problems such as spinocerebellar ataxia and myopathies.[5] Deficiency can also cause anemia, due to oxidative damage to red blood cells.
Supplements
Commercial vitamin E supplements can be classified into several distinct categories:
- Fully synthetic vitamin E, "dl-alpha-tocopherol", the most inexpensive, most commonly sold supplement form usually as the acetate ester;
- Semi-synthetic "natural source" vitamin E esters, the "natural source" forms used in tablets and multiple vitamins. These are highly fractionated d-alpha tocopherol or its esters, often made by synthetic methylation of gamma and beta d,d,d tocopherol vitamers extracted from plant oils.
- Less fractionated "natural mixed tocopherols" and high d-gamma-tocopherol fraction supplements
Synthetic all-racemic
Synthetic vitamin E derived from petroleum products is manufactured as all-racemic alpha tocopheryl acetate with a mixture of eight stereoisomers. In this mixture, one alpha-tocopherol molecule in eight molecules are in the form of RRR-alpha-tocopherol (12.5% of the total).[13]
The 8-isomer all-rac vitamin E is always marked on labels simply as dl-tocopherol or dl-tocopheryl acetate, even though it is (if fully written out) actually dl,dl,dl-tocopherol. The present largest manufacturers of this type are DSM and BASF.
(An earlier semisynthetic vitamin E actually contained 50% d,d,d-alpha tocopherol moiety and 50% l,d,d-alpha-tocopherol moiety, as synthesized by an earlier process which started with a plant sterol intermediate with the correct chirality in the tail, and thus resulted in a racemic mixture at only one chiral center. This form, known as 2-ambo tocopherol, is no longer made.)
Natural alpha-tocopherol is the RRR-alpha (or ddd-alpha) form. The synthetic dl,dl,dl-alpha ("dl-alpha") form is not as active as the natural ddd-alpha ("d-alpha") tocopherol form. This is mainly due to reduced vitamin activity of the 4 possible stereoisomers which are represented by the l or S enantiomer at the first stereocenter (an S or l configuration between the chromanol ring and the tail, i.e., the SRR, SRS, SSR, and SSS stereoisomers).[4] Unnatural 2R stereoisomers with natural R configuration at this stereocenter, but S at the other centers in the tail (RSR, RRS), appear to retain substantial RRR vitamin activity because they are recognized by the alpha-tocopherol transport protein, and thus maintained in the plasma, where the other four stereoisomers are not. Thus, the synthetic all-rac-α-tocopherol probably has only about half the vitamin activity of RRR-alpha-tocopherol in humans, even though the ratio of activities of the 8 stereoisomer racemic mixture to the natural vitamin is 1 to 1.36 in the rat pregnancy model. [14]
Although it is clear that mixtures of stereoisomers are not as active as the natural RRR-alpha-tocopherol form, in the ratios discussed above, specific information on any side effects of the seven synthetic vitamin E stereoisomers is not readily available. Naturopathic and orthomolecular medicine advocates have held that none of the other stereoisomers of vitamin E have merit for cancer, circulatory and heart diseases, but hold this opinion without being able to point to definitive studies of the matter.
Esters
Manufacturers also commonly convert the phenol form of the vitamins (with a free hydroxyl group) to esters, using acetic or succinic acid. These tocopheryl esters are more stable and are easy to use in vitamin supplements. Alpha tocopheryl esters are de-esterified in the gut and then absorbed as the free tocopherol.[15][16]

An initial study in humans saw large variability between different people's absorption of all these forms of vitamin E, with no statistically-significant differences seen between tocopheryl esters and the free tocopherol.[17] Later studies saw no difference between the rate of absorption of these forms of vitamin E and found that tocopheryl esters and free tocopherol had the same bioavailability.[18][19] The esterase activity responsible for releasing the free tocopherol may be reduced in children with cystic fibrosis.[20]
Tocopheryl nicotinate and tocopheryl linolate esters are used in cosmetics and some pharmaceuticals.
Mixed tocopherols
"Mixed tocopherols" in the US contain at least 20% w/w other natural R, R,R- tocopherols, i.e. R, R,R-alpha-tocopherol content plus at least 25% R, R,R-beta-, R, R,R-gamma-, R, R,R-delta-tocopherols.
Some brands may contain 200% w/w or more of the other tocopherols and measurable tocotrienols. Some mixed tocopherols with higher gamma-tocopherol content are marketed as "High Gamma-Tocopherol". The label should report each component in milligrams, except R, R,R-alpha-tocopherol may still be reported in IU. Mixed tocopherols can also be found in other nutritional supplements.
Other uses
Conventional medical studies on vitamin E, as of 2006 and as below, use either a synthetic all-racemic ("d, l-") alpha tocopheryl ester (acetate or succinate) or a semi-synthetic d-alpha tocopheryl ester (acetate or succinate). Proponents of megavitamin, orthomolecular and naturally based therapies have advocated, for the last two thirds of a century, and have used the natural tocopherols, often mixed tocopherols with an additional 25% - 200% w/w d-beta-, d-gamma-,[21][22] and d-delta-tocopherol. Based on various clinical, experimental, patent, and individual data, natural health proponents have long held[23][24] that the other poorly studied tocopherols, especially the abundant d-gamma-tocopherol,[25] in combination with other antioxidants such as selenium, coQ10, vitamin C, vitamin K2, mixed carotenoids, and lipoic acid, provide unique biochemical benefits.[26] The methodology, interpretation and reporting of conventional vitamin E studies have even become contentious within conventional medicine circles.[27]
Controversy
"Megadoses" of Vitamin E are not recommended by many government agencies, due to a possible increased risk of bleeding. A 2005 meta-analysis by Miller found that high-dosage vitamin E supplements may increase all-cause mortality.[28] "High dose" vitamin E esters (>400 units/day) were also associated with an increased risk in all-cause mortality of 39 per 10,000 persons, and a statistically significant relation existed between dose and mortality, with increased risk at doses exceeding 150 units per day. These trials included synthetic beta-carotene and other confounders.
The Miller study was criticised in the Journal of the American Nutraceutical Association.[26] Acute toxicity seems to be low with one author concluding that "toxicity symptoms have not been reported even at intakes of 800 IU per kilogram of body weight daily for 5 months" according to the Food and Nutrition Board (Rosenberg, et al), an amount that corresponds to 60,000 IU per day for a 75 kg adult.
A review of a number of randomized controlled trials in the scientific literature by the Cochrane Collaboration published in JAMA in 2007 also found an increase in mortality, of 4% (Relative Risk 1.04, 95% confidence interval 1.01-1.07), or 400 per 10,000 persons.[29]
Topical use
Vitamin E is widely used in industry as an inexpensive antioxidant (namely for cosmetics and foods). Vitamin E containing products are commonly used in the belief that vitamin E is good for the skin; many cosmetics include it, often labeled as tocopherol acetate, tocopheryl linoleate or tocopheryl nicotinate. Individuals can still experience allergic reactions to some tocopheryl esters or develop a rash and hives that may spread over the entire body from the use of topical products with alpha tocopheryl esters.[30]
Reduce scarring
Topical use of Vitamin E is often claimed by manufacturers of skin creams and lotions to play a role in encouraging skin healing and reducing scarring after injuries such as burns on the basis of limited research,[31] but the weak evidence of a benefit of silicon gel sheeting with or without added Vitamin E is limited by the poor quality of the research.[32] Indeed one study found that it did not improve or worsen the cosmetic appearance in 90% of patients, with a third developing contact dermatitis.[33]
During pregnancy
Recent studies into the use of both vitamin C and the single isomer vitamin E esters as possible help in preventing oxidative stress leading to pre-eclampsia has failed to show significant benefits,[34] but did increase the rate of babies born with a low birthweight in one study.[35]
Heart disease
Preliminary research has led to a widely held belief that vitamin E may help prevent or delay coronary heart disease, but larger controlled studies have not shown any benefit. Many researchers advance the belief that oxidative modification of LDL-cholesterol (sometimes called "bad" cholesterol) promotes blockages in coronary arteries that may lead to atherosclerosis and heart attacks. Vitamin E may help prevent or delay coronary heart disease by limiting the oxidation of LDL-cholesterol. Vitamin E also may help prevent the formation of blood clots, which could lead to a heart attack. Observational studies have associated lower rates of heart disease with higher vitamin E intake. A study of approximately 90,000 nurses suggested that the incidence of heart disease was 30% to 40% lower among nurses with the highest intake of vitamin E from diet and supplements. The range of intakes from both diet and supplements in this group was 21.6 to 1,000 IU (32 to 1,500 mg), with the median intake being 208 IU (139 mg). A 1994 review of 5,133 Finnish men and women aged 30 - 69 years suggested that increased dietary intake of vitamin E was associated with decreased mortality (death) from heart disease.
But even though these observations are promising, randomized clinical trials have consistently shown lack of benefit to the role of vitamin E supplements in heart disease. The Heart Outcomes Prevention Evaluation (HOPE) Study followed almost 10,000 patients for 4.5 years who were at high risk for heart attack or stroke. In this intervention study the subjects who received 265 mg (400) IU of vitamin E daily did not experience significantly fewer cardiovascular events or hospitalizations for heart failure or chest pain when compared to those who received a sugar pill. The researchers suggested that it is unlikely that the vitamin E supplement provided any protection against cardiovascular disease in the HOPE study. This study is continuing, to determine whether a longer duration of intervention with vitamin E supplements will provide any protection against cardiovascular disease.
Furthermore, meta analysis of several trials of antioxidants, including vitamin E, have not shown any benefit to vitamin E supplementation for preventing coronary heart disease.[36] One study suggested that Vitamin E (as alpha-tocopherol only) supplementation may increase the risk for heart failure.[37] Supplementing alpha-tocopherol without gamma-tocopherol is known to lead to reduced serum gamma- and delta-tocopherol concentrations.[38]
On September 10, 2007, the American Heart Association (in its journal Circulation) stated that women taking regular doses of vitamin E or Tocopherol were 21% less likely to suffer a blood clot. Dr. Robert Glynn of Harvard Medical School said (it was an interesting finding but not yet proven and) further research must confirm the link in the prevention of venous thromboembolism, and patients must not stop taking prescribed blood thinners.[39]
Cancer
Antioxidants such as vitamin E help protect against the damaging effects of free radicals, which may contribute to the development of chronic diseases such as cancer. Vitamin E also may block the formation of nitrosamines, which are carcinogens formed in the stomach from nitrites consumed in the diet. It also may protect against the development of cancers by enhancing immune function. To date, human trials and surveys that have tried to associate vitamin E with incidence of cancer remain generally inconclusive.
Some evidence associates higher intake of vitamin E with a decreased incidence of prostate cancer (see ATBC study) and breast cancer. Some studies correlate additional cofactors, such as specific vitamin E isomers, e.g. gamma-tocopherol, and other nutrients, e.g. selenium, with dramatic risk reductions in prostate cancer.[40] However, an examination of the effect of dietary factors, including vitamin E, on incidence of postmenopausal breast cancer in over 18,000 women from New York State did not associate a greater vitamin E intake with a reduced risk of developing breast cancer. A study of the effect on lung cancer in smokers also showed no benefit.[41]
A study of women in Iowa provided evidence that an increased dietary intake of vitamin E may decrease the risk of colon cancer, especially in women under 65 years of age. On the other hand, vitamin E intake was not statistically associated with risk of colon cancer in almost 2,000 adults with cancer who were compared to controls without cancer. At this time there is limited evidence to recommend vitamin E supplements for the prevention of cancer.
Recent studies have found that increased intake of vitamin E, especially among smokers may be responsible for an increase in the incidence of lung cancer, with one study finding an increase in the incidence of lung cancer by 7% for each 100IU of vitamin E taken daily.[42][43][44]A contradictional newer study found that alpha-tocopherol taken more than 7.73 mg per day were associated with a 53% reduction in lung cancer risk where other forms of the vitamin did not have any effects on their own. [45]
Cataracts
A cataract is a condition of clouding of the tissue of the lens of the eye. They increase the risk of disability and blindness in aging adults. Antioxidants are being studied to determine whether they can help prevent or delay cataract growth. Observational studies have found that lens clarity, which is used to diagnose cataracts, was better in regular users of vitamin E supplements and in persons with higher blood levels of vitamin E. A controlled trial of high doses of vitamins C and E and beta carotene found no effect on the risk of developing cataracts.[46] Similarly, a trial using vitamin E alone found that vitamin E supplementation produced no change in the risk of developing cataracts or the rate of progression of existing cataracts.[47]
Age-related macular degeneration (AMD) is the leading cause of visual impairment and blindness in the United States and the developed world among people 65 years and older. It has been shown that vitamin E alone does not attenuate the development or progression of AMD.[48]
However, studies focusing on efficacy of Vitamin E combined with other antioxidants, like zinc and vitamin C, indicate a protective effect against the onset and progression of AMD[49][50][51]
Glaucoma
A 2007 study published in the European Journal of Ophthalmology found that, along with other treatments for glaucoma, adding alpha-tocopherol appeared to help protect the retina from glaucomatous damage. Groups receiving 300 mg and 600 mg per day of alpha-tocopherol, delivered orally, showed statistically significant decreases in the resistivity index in the posterior ciliary arteries and in the pulsatility index in the ophthalmic arteries, after six and twelve months of therapy. Alpha-tocopherol-treated patients also had significantly lower differences in mean visual field deviations."[52]
Alzheimer's disease
Alzheimer's disease is a wasting disease of the brain. As oxidative stress may be involved in the pathogenesis of Alzheimer's, tocopherols have been tested as both a means of preventing and treating this disease. The results of these studies have been mixed, with some research suggesting that high levels of vitamin E in the diet may reduce the risk of Alzheimer's, while other studies found no such link.[53] Similarly, studies on if tocopherols could slow the progression of Alzheimer's have also been contradictory, with the Alzheimer’s Disease Cooperative Study suggesting that vitamin E supplementation might be beneficial, but a later trial finding no clinical benefit.[54] Due to this contradictory and confusing evidence, vitamin E or tocopherol supplements are not currently recommended for treating or preventing Alzheimer's disease.[55]
Parkinson's disease
In May 2005, The Lancet Neurology published a study suggesting that vitamin E may help protect against Parkinson's disease.[56] Individuals with moderate to high intakes of dietary vitamin E were found to have a lower risk of Parkinson's. No conclusion could be made from this trial about whether supplemental vitamin E has the same effect, however.[57] Other trials have tested if giving vitamin E supplements reduce the risk of Parkinson's disease, or if they can slow the progression of the disease. In a 1998 study, vitamin E supplements had no effect on the rate of progression of this disease[58]
See also
- Alkylresorcinols
References
- ↑ Merck Index, 11th Edition, 9931.
- ↑ Burton, G. W. and Ingold, K. U., "Autoxidation of biological molecules. 1. Antioxidant activity of vitamin E and related chain-breaking phenolic antioxidants in vitro", J. Am. Chem. Soc., 1981, 103, 6472 - 6477.
- ↑ Rigotti A (2007). "Absorption, transport, and tissue delivery of vitamin E". Mol. Aspects Med. 28 (5-6): 423–36. doi:. PMID 17320165.
- ↑ 4.0 4.1 Jensen SK, Lauridsen C (2007). "Alpha-tocopherol stereoisomers". Vitam. Horm. 76: 281–308. doi:. PMID 17628178.
- ↑ 5.0 5.1 Brigelius-Flohé R, Traber MG (July 1999). "Vitamin E: function and metabolism". FASEB J. 13 (10): 1145–55. PMID 10385606. http://www.fasebj.org/cgi/pmidlookup?view=long&pmid=10385606.
- ↑ Composition of Foods Raw, Processed, Prepared USDA National Nutrient Database for Standard Reference, Release 20 USDA, Feb. 2008
- ↑ Evans H. M., Bishop K. S. (1922). "On the existence of a hitherto unrecognized dietary factor essential for reproduction". Science 56 (1458): 650–651. doi:. http://links.jstor.org/sici?sici=0036-8075%2819221208%293%3A56%3A1458%3C650%3AOTEOAH%3E2.0.CO%3B2-Q.
- ↑ Evans H. M., Emerson O. H., Emerson G. A. (1936). "The isolation from wheat germ oil of an alcohol, a-tocopherol, having the properties of vitamin E". Journal of Biological Chemistry 113 (1): 319–332. http://www.jbc.org/cgi/reprint/113/1/319.
- ↑ Fernholz E. (1938). "On the Constitution of α-Tocopherol". Journal of the American Chemical Society 60 (1): 700–705. doi:.
- ↑ L. Iuliano; F. Micheletta; M. Maranghi; G. Frati; U. Diczfalusy; F. Violi (2001). "Bioavailability of Vitamin E as Function of Food Intake in Healthy Subjects". Arteriosclerosis, Thrombosis, and Vascular Biology 21: e34–e37. doi:. PMID 11597949. http://atvb.ahajournals.org/cgi/content/full/atvbaha;21/10/e34.
- ↑ Vitamin E Fact sheet
- ↑ J. Bauernfeind in: L. J. Machlin (ed.): Vitamin E – A Comprehensive Treatise, Marcel Dekker, New York 1980, p. 99
- ↑ Weiser H, Riss G, Kormann AW (October 1996). "Biodiscrimination of the eight alpha-tocopherol stereoisomers results in preferential accumulation of the four 2R forms in tissues and plasma of rats". J. Nutr. 126 (10): 2539–49. PMID 8857515. http://jn.nutrition.org/cgi/pmidlookup?view=long&pmid=8857515.
- ↑ "Taken together, these data indicate that of the eight stereoisomers (RRR, RSR, RRS, RSS, SRR, SSR, SRS, SSS) in all-rac-α-tocopherol, only the four 2R-forms (RRR, RSR, RSS, RRS) are recognized by α-TTP and maintained in the plasma. Indeed, the Food and Nutrition Board (Food and Nutrition Board and Institute of Medicine, 2000) has defined that only α-tocopherol, specifically the 2R-forms of α-tocopherol, can fulfill the human requirement for vitamin E. Thus, all-rac-α-tocopherol has only half the activity of RRR-α-tocopherol." Taken from the discussion in [1]: Relative bioactivity of dietary RRR- and all-rac-alpha-tocopheryl acetates in swine assessed with deuterium-labeled vitamin E1. J Anim Sci 80:702-707, 2002.
- ↑ Mathias PM, Harries JT, Peters TJ, Muller DP (July 1981). "Studies on the in vivo absorption of micellar solutions of tocopherol and tocopheryl acetate in the rat: demonstration and partial characterization of a mucosal esterase localized to the endoplasmic reticulum of the enterocyte". J. Lipid Res. 22 (5): 829–37. PMID 7288289.
- ↑ Ajandouz el H, Castan S, Jakob S, Puigserver A (2006). "A fast, sensitive HPLC method for the determination of esterase activity on alpha-tocopheryl acetate". J Chromatogr Sci 44 (10): 631–3. PMID 17254374.
- ↑ Horwitt M, Elliott W, Kanjananggulpan P, Fitch C (1984). "Serum concentrations of alpha-tocopherol after ingestion of various vitamin E preparations". Am J Clin Nutr 40 (2): 240–5. PMID 6465056. link
- ↑ Cheeseman KH, Holley AE, Kelly FJ, Wasil M, Hughes L, Burton G (November 1995). "Biokinetics in humans of RRR-alpha-tocopherol: the free phenol, acetate ester, and succinate ester forms of vitamin E". Free Radic. Biol. Med. 19 (5): 591–8. doi:. PMID 8529918.
- ↑ Burton GW, Ingold KU, Foster DO, et al (September 1988). "Comparison of free alpha-tocopherol and alpha-tocopheryl acetate as sources of vitamin E in rats and humans". Lipids 23 (9): 834–40. doi:. PMID 3185118.
- ↑ Mathias PM, Harries JT, Muller DP (January 1981). "Optimization and validation of assays to estimate pancreatic esterase activity using well-characterized micellar solutions of cholesteryl oleate and tocopheryl acetate". J. Lipid Res. 22 (1): 177–84. PMID 7217783. http://www.jlr.org/cgi/pmidlookup?view=long&pmid=7217783.
- ↑ Jiang Q et al."Gamma tocopherol, the major form of vitamin E in the US diet, deserves more attention" Am J Clin Nutr 2001; 74: 714-22.
- ↑ JM Gaziano, Vitamin E and Cardiovascular Disease: Observational Studies, Ann. N.Y. Acad. Sci. 1031: 280–291 (2004) "
- ↑ Bailey H (1964) Vitamin E: Your Key to a Healthy Heart, Chilton Books, ASIN B000GS9VPQ Bailey describes mixed tocopherols use for CVD back to the 1940s
- ↑ Walker M, "New/Old Findings on Unique Vitamin E", Townsend Letter for Doctors and Patients, No. 111, 1992, p. 826
- ↑ MacWilliam L,"What Makes Gamma Tocopherol Superior to Alpha Tocopherol", LE Magazine, Report, April 2006
- ↑ 26.0 26.1 M. Houston, “Meta-Analysis, Metaphysics and Mythology” JANA Vol. 8 No. 1, 2005 original
- ↑ Carter, T. "Responses and Comments: High-Dosage Vitamin E Supplementation and All-Cause Mortality", Ann Intern Med. 2005 July 19;143(2):155; responses 150-160
- ↑ Miller E, Pastor-Barriuso R, Dalal D, Riemersma R, Appel L, Guallar E (2005). "Meta-analysis: high-dosage vitamin E supplementation may increase all-cause mortality.". Ann Intern Med 142 (1): 37–46. doi:10.1016/j.freeradbiomed.2007.06.019. (inactive 2008-06-25). PMID 15537682.
- ↑ Bjelakovic et al., "Mortality in randomized trials of antioxidant supplements for primary and secondary prevention: Systematic review and meta-analysis", JAMA, 297:842; February 28, 2007 [2]
- ↑ Topical Vitamin E Formulations: Not Always Benign, Skin Therapy Letter Vol. 1, No. 3, January 1996
- ↑ Palmieri B, Gozzi G, Palmieri G (1995). "Vitamin E added silicone gel sheets for treatment of hypertrophic scars and keloids". Int. J. Dermatol. 34 (7): 506–9. doi:. PMID 7591421.
- ↑ O'Brien L, Pandit A (2006). "Silicon gel sheeting for preventing and treating hypertrophic and keloid scars". Cochrane Database Syst Rev (1): CD003826. doi:. PMID 16437463.
- ↑ Baumann LS, Spencer J (1999). "The effects of topical vitamin E on the cosmetic appearance of scars". Dermatol Surg 25 (4): 311–5. doi:. PMID 10417589. Lay summary – Vitamin E - Paula Begoun at CosmeticsCop (2008-01-01).
- ↑ Rumbold A, Crowther C, Haslam R, Dekker G, Robinson J (2006). "Vitamins C and E and the risks of pre-eclampsia and perinatal complications.". N Engl J Med 354 (17): 1796–806. doi:. PMID 16641396.
- ↑ Poston L, Briley A, Seed P, Kelly F, Shennan A (2006). "Vitamin C and vitamin E in pregnant women at risk for pre-eclampsia (VIP trial): randomised placebo-controlled trial.". Lancet 367 (9517): 1145–54. doi:. PMID 16616557.
- ↑ Vivekananthan D, Penn M, Sapp S, Hsu A, Topol E (2003). "Use of antioxidant vitamins for the prevention of cardiovascular disease: meta-analysis of randomised trials.". Lancet 361 (9374): 2017–23. doi:. PMID 12814711.
- ↑ Lonn E, Bosch J, Yusuf S, Sheridan P, Pogue J, Arnold J, Ross C, Arnold A, Sleight P, Probstfield J, Dagenais G (2005). "Effects of long-term vitamin E supplementation on cardiovascular events and cancer: a randomized controlled trial.". JAMA 293 (11): 1338–47. doi:. PMID 15769967.
- ↑ Huang HY, Appel LJ (2003). "Supplementation of diets with alpha-tocopherol reduces serum concentrations of gamma- and delta-tocopherol in humans". J. Nutr. 133 (10): 3137–40. PMID 14519797.
- ↑ Yahoo.com, Vitamin E may reduce blood clots in women: study
- ↑ Helzlsouer K, Huang H, Alberg A, Hoffman S, Burke A, Norkus E, Morris J, Comstock G (2000). "Association between alpha-tocopherol, gamma-tocopherol, selenium, and subsequent prostate cancer". J Natl Cancer Inst 92 (24): 2018–23. doi:. PMID 11121464.
- ↑ Beta Carotene Cancer Prevention Study Group The Alpha-Tocopherol, (1994). "The effect of vitamin E and beta carotene on the incidence of lung cancer and other cancers in male smokers. The Alpha-Tocopherol, Beta Carotene Cancer Prevention Study Group". N Engl J Med 330 (15): 1029–35. doi:. PMID 8127329.
- ↑ Cancer Research UK : Jury still out over vitamin E supplements and increased lung cancer risk
- ↑ Nursing in Practice - Vitamin E "linked to cancer"
- ↑ eCanadaNow.com - Vitamin E Linked To Increased Risk of Lung Cancer
- ↑ S. Mahabir, K. Schendel, Y.Q. Dong, S.L. Barrera, M.R. Spitz, M.R. Forman (2008). "Dietary alpha-, beta-, gamma- and delta-tocopherols in lung cancer risk". International Journal of Cancer 123: 1173–1180. doi:. PMID 8127329.
- ↑ "A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E and beta carotene for age-related cataract and vision loss: AREDS report no. 9". Arch. Ophthalmol. 119 (10): 1439–52. October 2001. PMID 11594943. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pubmed&pubmedid=11594943.
- ↑ McNeil JJ, Robman L, Tikellis G, Sinclair MI, McCarty CA, Taylor HR (January 2004). "Vitamin E supplementation and cataract: randomized controlled trial". Ophthalmology 111 (1): 75–84. doi:. PMID 14711717.
- ↑ Taylor H, Tikellis G, Robman L, McCarty C, McNeil J (2002). "Vitamin E supplementation and macular degeneration: randomised controlled trial". BMJ 325 (7354): 11. doi:. PMID 12098721.
- ↑ "A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8". Arch Ophthalmol 119 (10): 1417–36. 2001. PMID 11594942.
- ↑ van Leeuwen R, Boekhoorn S, Vingerling J, Witteman J, Klaver C, Hofman A, de Jong P (2005). "Dietary intake of antioxidants and risk of age-related macular degeneration". JAMA 294 (24): 3101–7. doi:. PMID 16380590.
- ↑ Moriarty-Craige S, Adkison J, Lynn M, Gensler G, Bressler S, Jones D, Sternberg P (2005). "Antioxidant supplements prevent oxidation of cysteine/cystine redox in patients with age-related macular degeneration". Am J Ophthalmol 140 (6): 1020–6. doi:. PMID 16376645.
- ↑ Engin KN, Engin G, Kucuksahin H, Oncu M, Engin G, Guvener B (2007). "Clinical evaluation of the neuroprotective effect of alpha-tocopherol against glaucomatous damage". European journal of ophthalmology 17 (4): 528–33. PMID 17671926.
- ↑ Frank B, Gupta S (2005). "A review of antioxidants and Alzheimer's disease". Ann Clin Psychiatry 17 (4): 269–86. doi:. PMID 16402761.
- ↑ Ricciarelli R, Argellati F, Pronzato MA, Domenicotti C (2007). "Vitamin E and neurodegenerative diseases". Mol. Aspects Med. 28 (5-6): 591–606. doi:. PMID 17306357.
- ↑ Boothby LA, Doering PL (December 2005). "Vitamin C and vitamin E for Alzheimer's disease". Ann Pharmacother 39 (12): 2073–80. doi:. PMID 16227450.
- ↑ Etminan M, Gill SS, Samii A (2005). "Intake of vitamin E, vitamin C, and carotenoids and the risk of Parkinson's disease: a meta-analysis". Lancet Neurol 4 (6): 362–5. doi:. PMID 15907740.
- ↑ "Vitamin E cuts Parkinson's risk", BBC News (19 May 2005). Retrieved on 2008-01-01.
- ↑ Shoulson I (September 1998). "DATATOP: a decade of neuroprotective inquiry. Parkinson Study Group. Deprenyl And Tocopherol Antioxidative Therapy Of Parkinsonism". Ann. Neurol. 44 (3 Suppl 1): S160–6. PMID 9749589.
External links
- Vitamin E - Its Role and Mechanism of Action
- Jane Higdon, "Vitamin E", Micronutrient Information Center, Linus Pauling Institute
- US Office of Dietary Supplements article on Vitamin E
- Vitamin E (Tocopherols and Tocotrienols)
- Vitamin E risk assessment, Expert Group on Vitamins and Minerals, UK Food Standards Agency, 2003
- High dose vitamin E leads to longer more active lives in mice
- Do vitamins C and E affect respiratory infections? (Dissertation 2006)
|
|||||||||||||||||||||||||||