Prostate cancer
| Prostate cancer Classification and external resources |
|
 |
|
|---|---|
| ICD-10 | C61. |
| ICD-9 | 185 |
| OMIM | 176807 |
| DiseasesDB | 10780 |
| MedlinePlus | 000380 |
| eMedicine | radio/574 |
| MeSH | D011471 |
Prostate cancer is a disease in which cancer develops in the prostate, a gland in the male reproductive system. It occurs when cells of the prostate mutate and begin to multiply out of control. These cells may spread (metastasize) from the prostate to other parts of the body, especially the bones and lymph nodes. Prostate cancer may cause pain, difficulty in urinating, problems during sexual intercourse, erectile dysfunction and other symptoms.
Rates of prostate cancer vary widely across the world. Although the rates vary widely between countries, it is least common in South and East Asia, more common in Europe, and most common in the United States.[1] Prostate cancer develops most frequently in men over fifty. This cancer can occur only in men, as the prostate is exclusively of the male reproductive tract. It is one of the most common types of cancer in men. However, many men who develop prostate cancer never have symptoms, undergo no therapy, and eventually die of other causes. That is because malignant neoplasms of the prostate are, in most cases, slow-growing, and because most of those affected are over 60. Hence they often die of causes unrelated to the prostate cancer, such as heart/circulatory disease, pneumonia, other unconnected cancers or old age. Many factors, including genetics and diet, have been implicated in the development of prostate cancer.
Prostate cancer is most often discovered by PSA (prostate specific antigen) screening and less commonly by physical examination or by symptoms. There is some current concern about the accuracy of the PSA test and its usefulness. Suspected prostate cancer is typically confirmed by taking a biopsy of the prostate and examining it under a microscope. Further tests, such as CT scans and bone scans, may be performed to determine whether prostate cancer has spread.
Treatment options for prostate cancer with intent to cure are primarily surgery and radiation therapy. Other treatments such as hormonal therapy, chemotherapy, proton therapy, cryosurgery, high intensity focused ultrasound (HIFU) also exist depending on the clinical scenario and desired outcome. Abiraterone Acetate is showing promise in reducing Tumor Size and PSA levels in Aggressive end-stage prostate cancers.[2] The age and underlying health of the man as well as the extent of spread, appearance under the microscope and response of the cancer to initial treatment are important in determining the outcome of the disease. The decision whether or not to treat localized prostate cancer (a tumor that is contained within the prostate) with curative intent is a patient trade-off between the expected beneficial and harmful effects in terms of patient survival and quality of life.
Contents |
Prostate
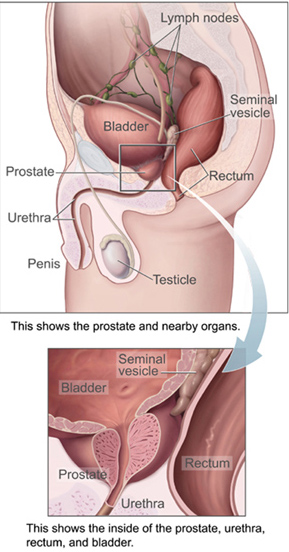
The prostate is a part of the male reproductive organ which helps make and store seminal fluid. In adult men a typical prostate is about three centimeters long and weighs about twenty grams.[3] It is located in the pelvis, under the urinary bladder and in front of the rectum. The prostate surrounds part of the urethra, the tube that carries urine from the bladder during urination and semen during ejaculation.[4] Because of its location, prostate diseases often affect urination, ejaculation, and rarely defecation. The prostate contains many small glands which make about twenty percent of the fluid constituting semen.[5] In prostate cancer the cells of these prostate glands mutate into cancer cells. The prostate glands require male hormones, known as androgens, to work properly. Androgens include testosterone, which is made in the testes; dehydroepiandrosterone, made in the adrenal glands; and dihydrotestosterone, which is converted from testosterone within the prostate itself. Androgens are also responsible for secondary sex characteristics such as facial hair and increased muscle mass.
Symptoms
Early prostate cancer usually causes no symptoms. Often it is diagnosed during the workup for an elevated PSA noticed during a routine checkup. Sometimes, however, prostate cancer does cause symptoms, often similar to those of diseases such as benign prostatic hypertrophy. These include frequent urination, increased urination at night, difficulty starting and maintaining a steady stream of urine, blood in the urine, and painful urination. Prostate cancer is associated with urinary dysfunction as the prostate gland surrounds the prostatic urethra. Changes within the gland therefore directly affect urinary function. Because the vas deferens deposits seminal fluid into the prostatic urethra, and secretions from the prostate gland itself are included in semen content, prostate cancer may also cause problems with sexual function and performance, such as difficulty achieving erection or painful ejaculation.[6].
Advanced prostate cancer can spread to other parts of the body and this may cause additional symptoms. The most common symptom is bone pain, often in the vertebrae (bones of the spine), pelvis or ribs. Spread of cancer into other bones such as the femur is usually to the proximal part of the bone. Prostate cancer in the spine can also compress the spinal cord, causing leg weakness and urinary and fecal incontinence.[7]
Pathophysiology

Prostate cancer is classified as an adenocarcinoma, or glandular cancer, that begins when normal semen-secreting prostate gland cells mutate into cancer cells. The region of prostate gland where the adenocarcinoma is most common is the peripheral zone. Initially, small clumps of cancer cells remain confined to otherwise normal prostate glands, a condition known as carcinoma in situ or prostatic intraepithelial neoplasia (PIN). Although there is no proof that PIN is a cancer precursor, it is closely associated with cancer. Over time these cancer cells begin to multiply and spread to the surrounding prostate tissue (the stroma) forming a tumor. Eventually, the tumor may grow large enough to invade nearby organs such as the seminal vesicles or the rectum, or the tumor cells may develop the ability to travel in the bloodstream and lymphatic system. Prostate cancer is considered a malignant tumor because it is a mass of cells which can invade other parts of the body. This invasion of other organs is called metastasis. Prostate cancer most commonly metastasizes to the bones, lymph nodes, rectum, and bladder.
Etiology
The specific causes of prostate cancer remain unknown.[8] A man's risk of developing prostate cancer is related to his age, genetics, race, diet, lifestyle, medications, and other factors. The primary risk factor is age. Prostate cancer is uncommon in men less than 45, but becomes more common with advancing age. The average age at the time of diagnosis is 70.[9] However, many men never know they have prostate cancer. Autopsy studies of Chinese, German, Israeli, Jamaican, Swedish, and Ugandan men who died of other causes have found prostate cancer in thirty percent of men in their 50s, and in eighty percent of men in their 70s.[10] In the year 2005 in the United States, there were an estimated 230,000 new cases of prostate cancer and 30,000 deaths due to prostate cancer.[11]
A man's genetic background contributes to his risk of developing prostate cancer. This is suggested by an increased incidence of prostate cancer found in certain racial groups, in identical twins of men with prostate cancer, and in men with certain genes. In the United States, prostate cancer more commonly affects black men than white or Hispanic men, and is also more deadly in black men.[12] Men who have a brother or father with prostate cancer have twice the usual risk of developing prostate cancer.[13] Studies of twins in Scandinavia suggest that forty percent of prostate cancer risk can be explained by inherited factors.[14] However, no single gene is responsible for prostate cancer; many different genes have been implicated. Two genes (BRCA1 and BRCA2) that are important risk factors for ovarian cancer and breast cancer in women have also been implicated in prostate cancer.[15]
Dietary amounts of certain foods, vitamins, and minerals can contribute to prostate cancer risk. Men with higher serum levels of the short-chain ω-6 fatty acid linoleic acid have higher rates of prostate cancer. However, the same series of studies showed that men with elevated levels of long-chain ω-3 (EPA and DHA) had lowered incidence.[16] A long-term study reports that "blood levels of trans fatty acids, in particular trans fats resulting from the hydrogenation of vegetable oils, are associated with an increased prostate cancer risk."[17] Other dietary factors that may increase prostate cancer risk include low intake of vitamin E (Vitamin E is found in green, leafy vegetables), omega-3 fatty acids (found in fatty fishes like salmon), and the mineral selenium. A study in 2007 cast doubt on the effectiveness of lycopene (found in tomatoes) in reducing the risk of prostate cancer.[18] Lower blood levels of vitamin D also may increase the risk of developing prostate cancer. This may be linked to lower exposure to ultraviolet (UV) light, since UV light exposure can increase vitamin D in the body.[19]
There are also some links between prostate cancer and medications, medical procedures, and medical conditions. Daily use of anti-inflammatory medicines such as aspirin, ibuprofen, or naproxen may decrease prostate cancer risk.[20] Use of the cholesterol-lowering drugs known as the statins may also decrease prostate cancer risk.[21] More frequent ejaculation also may decrease a man's risk of prostate cancer. One study showed that men who ejaculated five times a week in their 20s had a decreased rate of prostate cancer, though others have shown no benefit.[22][23] Infection or inflammation of the prostate (prostatitis) may increase the chance for prostate cancer. In particular, infection with the sexually transmitted infections chlamydia, gonorrhea, or syphilis seems to increase risk.[24] Finally, obesity[25] and elevated blood levels of testosterone[26] may increase the risk for prostate cancer.
Research released in May 2007, found that US war veterans who had been exposed to Agent Orange had a 48% increased risk of prostate cancer recurrence following surgery.[27]
Prostate cancer risk can be decreased by modifying known risk factors for prostate cancer, such as decreasing intake of animal fat.[28]
One research study, by the Cancer Council Victoria, has shown that men who report that they regularly ("more than five times per week") masturbate have up to one third fewer occurrences of prostate cancer.[29][22] The researchers hypothesize that this could be because regular ejaculation reduces the buildup of carcinogenic deposits such as 3-methylcholanthrene, produced from the breakdown of cholesterol, which could damage the cells lining the prostate. The researchers also speculated that frequent ejaculation may cause the prostate to mature fully, making it less susceptible to carcinogens. It is also possible that there is another factor (such as hormone levels) that is a common cause of both a reduced susceptibility to prostate cancer and a tendency toward frequent masturbation. There is also some evidence that frequent sexual intercourse is associated with reduced risk of prostate cancer, although contrarily the risks associated with STDs have been shown to increase the risk of prostate cancer.[29][22] Once the lining of the prostate is affected with cancer, the only known treatments are surgery and radiation therapy. Both may limit the ability to have erections afterward.
Prevention
Vitamins and medication
Evidence from epidemiological studies supports protective roles in reducing prostate cancer for dietary selenium, vitamin E, lycopene, and soy foods. High plasma levels of Vitamin D may also have a protective effect.[30] Estrogens from fermented soybeans and other plant sources (called phytoestrogens) may also help prevent prostate cancer.[31] The selective estrogen receptor modulator drug toremifene has shown promise in early trials.[32][33] Two medications which block the conversion of testosterone to dihydrotestosterone, finasteride[34] and dutasteride,[35] have also shown some promise. The use of these medications for primary prevention is still in the testing phase, and they are not widely used for this purpose. The initial problem with these medications is that they may preferentially block the development of lower-grade prostate tumors, leading to a relatively greater chance of higher grade cancers, and negating any overall survival improvement. More recent research found that finasteride did not increase the percentage of higher grade cancers. A 2008 study update found that finasteride reduces the incidence of prostate cancer by 30%. In the original study it turns that that the smaller prostate caused by finasteride means that a doctor is more likely to hit upon cancer nests and more likely to find aggressive-looking cells. Most of the men in the study who had cancer — aggressive or not — chose to be treated and many had their prostates removed. A pathologist then carefully examined every one of those 500 prostates and compared the kinds of cancers found at surgery to those initially diagnosed at biopsy. Finasteride did not increase the risk of High-Grade prostate cancer.[36][37]
Green tea may be protective (due to its polyphenol content),[38] although the most comprehensive clinical study indicates that it has no protective effect.[39] A 2006 study of green tea derivatives demonstrated promising prostate cancer prevention in patients at high risk for the disease.[40] Recent research published in the Journal of the National Cancer Institute suggests that taking multivitamins more than seven times a week can increase the risks of contracting the disease.[41][42] This research was unable to highlight the exact vitamins responsible for this increase (almost double), although they suggest that vitamin A, vitamin E and beta-carotene may lie at its heart. It is advised that those taking multivitamins never exceed the stated daily dose on the label. Scientists recommend a healthy, well balanced diet rich in fiber, and to reduce intake of meat. A 2007 study published in the Journal of the National Cancer Institute found that men eating cauliflower, broccoli, or one of the other cruciferous vegetables, more than once a week were 40% less likely to develop prostate cancer than men who rarely ate those vegetables.[43][44] The phytochemicals indole-3-carbinol and diindolylmethane, found in cruciferous vegetables, has antiandrogenic and immune modulating properties.[45][46]
Ejaculation frequency
In 2003, an Australian research team led by Graham Giles of The Cancer Council Australia concluded that frequent masturbation by males appears to help prevent the development of prostate cancer.[47][29] Australian research concluded that the more men ejaculate between the ages of 20 and 50, the less likely they are to develop prostate cancer. The protective effect is greatest while men are in their twenties: those who had ejaculated more than five times per week in their twenties, for instance, were one-third less likely to develop aggressive prostate cancer later in life. The results contradict those of previous studies, which have suggested that having had many sexual partners, or a high frequency of sexual activity, increases the risk of prostate cancer by up to 40 percent. The key difference is that these earlier studies defined sexual activity as sexual intercourse, whereas this study focused on the number of ejaculations, whether or not intercourse was involved.[48] Another study completed in 2004 reported that "Most categories of ejaculation frequency were unrelated to risk of prostate cancer. However, high ejaculation frequency was related to decreased risk of total prostate cancer." The report abstract concluded, "Our results suggest that ejaculation frequency is not related to increased risk of prostate cancer." [49]
Screening
Prostate cancer screening is an attempt to find unsuspected cancers. Screening tests may lead to more specific follow-up tests such as a biopsy, where small cores of the prostate are removed for closer study. Prostate cancer screening options include the digital rectal exam and the prostate specific antigen (PSA) blood test. Screening for prostate cancer is controversial because it is not clear if the benefits of screening outweigh the risks of follow-up diagnostic tests and cancer treatments.
Prostate cancer is usually a slow-growing cancer, very common among older men. In fact, most prostate cancers never grow to the point where they cause symptoms, and most men with prostate cancer die of other causes before prostate cancer has an impact on their lives. The PSA screening test may detect these small cancers that would never become life threatening. Doing the PSA test in these men may lead to overdiagnosis, including additional testing and treatment. Follow-up tests, such as prostate biopsy, may cause pain, bleeding and infection. Prostate cancer treatments may cause urinary incontinence and erectile dysfunction. Therefore, it is essential that the risks and benefits of diagnostic procedures and treatment be carefully considered before PSA screening.
Several medical societies have not found sufficient evidence to support routine screening for prostate cancer - but the American Urological Association supports annual screening and digital examination for men over 50 years old - and starting earlier for 'men at high risk (those with a family history of prostate cancer or African American men)'. [50]
- In 2002, the U.S. Preventive Services Task Force (USPSTF) concluded that the evidence was insufficient to recommend for or against routine screening for prostate cancer using PSA testing or digital rectal examination (DRE).[51] The previous 1995 USPSTF recommendation was against routine screening.
- In 1997, American Cancer Society (ACS) guidelines began recommending that beginning at age 50 (age 45 for African-American men and men with a family history of prostate cancer, and since 2001, age 40 for men with a very strong family history of prostate cancer), PSA testing and DRE be offered annually to men who have a life-expectancy of 10 or more years (average life expectancy is 10 years or more for U.S. men under age 76)[52] along with information on the risks and benefits of screening.[53] The previous ACS recommendations since 1980 had been for routine screening for prostate cancer with DRE annually beginning at age 40, and since 1992 had been for routine screening with DRE and PSA testing annually beginning at age 50.[54]
- The 2007 National Comprehensive Cancer Network (NCCN) guideline recommends offering a baseline PSA test and DRE at ages 40 and 45 and annual PSA testing and DRE beginning at age 50 (with annual PSA testing and DRE beginning at age 40 for African-American men, men with a family history of prostate cancer, and men with a PSA ≥ 0.6 ng/mL at age 40 or PSA > 0.6 ng/mL at age 45) through age 80, along with information on the risks and benefits of screening. Biopsy is recommended if DRE is positive or PSA ≥ 4 ng/mL, and biopsy considered if PSA > 2.5 ng/mL or PSA velocity ≥ 0.35 ng/mL/year when PSA ≤ 2.5 ng/mL.[55]
- Some U.S. radiation oncologists and medical oncologists who specialize in treating prostate cancer recommend obtaining a baseline PSA in all men at age 35[56] or beginning annual PSA testing in high risk men at age 35.[57]
- The American Urological Association Patient Guide to Prostate Cancer.[58]
Since there is no general agreement that the benefits of PSA screening outweigh the harms, the consensus is that clinicians use a process of shared decision-making that includes discussing with patients the risks of prostate cancer, the potential benefits and harms of screening, and involving the patients in the decision.[59]
However, because PSA screening is widespread in the United States, following the recommendations of major scientific and medical organizations to use shared decision-making is legally perilous in some U.S. states.[60] In 2003, a Virginia jury found a family practice residency program guilty of malpractice and liable for $1 million for following national guidelines and using shared decision-making, thereby allowing a patient (subsequently found to have a high PSA and incurable advanced prostate cancer) to decline a screening PSA test, instead of routinely ordering without discussion PSA tests in all men ≥ 50 years of age as four local physicians testified was their practice, and was accepted by the jury as the local standard of care.[61]
An estimated 20 million PSA tests are done per year in North America and possibly 20 million more outside of North America.[62]
- In 2000, 34.1% of all U.S. men age ≥ 50 had a screening PSA test within the past year and 56.8% reported ever having a PSA test.[59]
- In 2000, 33.6% of all U.S. men age 50–64 and 51.3% of men age ≥ 65 had a PSA test within the past year.[63]
- In 2005, 33.5% of all U.S. men age 50–64 had a PSA test in the past year.
- 37.5% of men with private health insurance, 20.8% of men with Medicaid insurance, 14.0% of currently uninsured men, and 11.5% of men uninsured for > 12 months.[64]
- In 2000–2001, 34.1% of all Canadian men age ≥ 50 had a screening PSA test within the past year and 47.5% reported ever having a screening PSA test.[65]
- Canadian men in Ontario were most likely to have had a PSA test within the past year and men in Alberta were least likely to have had a PSA test with the past year or ever.[66]
Digital rectal examination
Digital rectal examination (DRE) is a procedure where the examiner inserts a gloved, lubricated finger into the rectum to check the size, shape, and texture of the prostate. Areas which are irregular, hard or lumpy need further evaluation, since they may contain cancer. Although the DRE only evaluates the back of the prostate, 85% of prostate cancers arise in this part of the prostate. Prostate cancer which can be felt on DRE is generally more advanced.[67] The use of DRE has never been shown to prevent prostate cancer deaths when used as the only screening test.[68]
Prostate specific antigen
The PSA test measures the blood level of prostate-specific antigen, an enzyme produced by the prostate. Specifically, PSA is a serine protease similar to kallikrein. Its normal function is to liquify gelatinous semen after ejaculation, allowing spermatozoa to more easily navigate through the uterine cervix.
The risk of prostate cancer increases with increasing PSA levels.[69] 4 ng/mL was chosen arbitrarily as a decision level for biopsies in the clinical trial upon which the FDA in 1994 based adding prostate cancer detection in men age 50 and over as an approved indication for the first commercially available PSA test.[70] 4 ng/mL was used as the biopsy decision level in the PLCO trial, 3 ng/mL was used in the ERSPC and ProtecT trials, and 2.5 ng/mL is used in the 2007 NCCN guideline.
PSA levels can change for many reasons other than cancer. Two common causes of high PSA levels are enlargement of the prostate (benign prostatic hypertrophy (BPH)) and infection in the prostate (prostatitis). It can also be raised for 24 hours after ejaculation and several days after catheterization. PSA levels are lowered in men who use medications used to treat BPH or baldness. These medications, finasteride (marketed as Proscar or Propecia) and dutasteride (marketed as Avodart), may decrease the PSA levels by 50% or more.
Several other ways of evaluating the PSA have been developed to avoid the shortcomings of simple PSA screening. The use of age-specific reference ranges improves the sensitivity and specificity of the test. The rate of rise of the PSA over time, called the PSA velocity, has been used to evaluate men with PSA levels between 4 and 10 ng/ml, but it has not proven to be an effective screening test.[71] Comparing the PSA level with the size of the prostate, as measured by ultrasound or magnetic resonance imaging, has also been studied. This comparison, called PSA density, is both costly and has not proven to be an effective screening test.[72] PSA in the blood may either be free or bound to other proteins. Measuring the amount of PSA which is free or bound may provide additional screening information, but questions regarding the usefulness of these measurements limit their widespread use.[73][74]
Diagnosis

When a man has symptoms of prostate cancer, or a screening test indicates an increased risk for cancer, more invasive evaluation is offered.
The only test which can fully confirm the diagnosis of prostate cancer is a biopsy, the removal of small pieces of the prostate for microscopic examination. However, prior to a biopsy, several other tools may be used to gather more information about the prostate and the urinary tract. Cystoscopy shows the urinary tract from inside the bladder, using a thin, flexible camera tube inserted down the urethra. Transrectal ultrasonography creates a picture of the prostate using sound waves from a probe in the rectum.
Biopsy
If cancer is suspected, a biopsy is offered. During a biopsy a urologist or radiologist obtains tissue samples from the prostate via the rectum. A biopsy gun inserts and removes special hollow-core needles (usually three to six on each side of the prostate) in less than a second. Prostate biopsies are routinely done on an outpatient basis and rarely require hospitalization. Fifty-five percent of men report discomfort during prostate biopsy.[75]
Gleason score
The tissue samples are then examined under a microscope to determine whether cancer cells are present, and to evaluate the microscopic features (or Gleason score) of any cancer found.
Tumor markers
Tissue samples can be stained for the presence of PSA and other tumor markers in order to determine the origin of maligant cells that have metastasized.[76]
New tests being investigated
Currently, an active area of research involves non-invasive methods of prostate tumor detection. Adenoviruses modified to transfect tumor cells with harmless yet distinct genes (such as luciferase) have proven capable of early detection. So far, though, this area of research has only been tested in animal and LNCaP models.[77]
PCA3
Another potential non-invasive method of early prostate tumor detection is through a molecular test that detects the presence of cell-associated PCA3 mRNA in urine. PCA3 mRNA is expressed almost exclusively by prostate cells and has been shown to be highly over-expressed in prostate cancer cells. PCA3 is not a replacement for PSA but an additional tool to help decide if, in men suspected of having prostate cancer, a biopsy is really needed. The higher the expression of PCA3 in urine, the greater the likelihood of a positive biopsy, i.e. the presence of cancer cells in the prostate. Company Diagnocure has an exclusive worldwide license for all diagnostic and therapeutic applications related to PCA3
Early prostate cancer
It was reported in April 2007 that a new blood test for early prostate cancer antigen-2 (EPCA-2) is being researched that may alert men if they have prostate cancer and how aggressive it will be.[78][79]
Prostasomes
Epithelial cells of the prostate secrete prostasomes as well as PSA. Prostasomes are membrane –surrounded, prostate-derived organelles that appear extracellularly and one of their physiological functions is to protect the sperm from attacks by the female immune system. Cancerous prostate cells continue to synthesize and secrete prostasomes and may be shielded against immunological attacks by these prostasomes. Research of several aspects of prostasomal involvement in prostate cancer has been performed.[80]
Prostate mapping
Prostate Mapping is a new diagnostic process developed by urology and radiology consultants in the UK. This is a method of diagnosis which may be accurate in determining the precise location and aggressiveness of cancer. It uses a combination of multi-sequence MRI imaging techniques and a template guided biopsy system and involves taking multiple biopsies through the skin that lies in front of the back passage rather than through the back passage. The procedure is carried out under general anaesthetic.
Staging
An important part of evaluating prostate cancer is determining the stage, or how far the cancer has spread. Knowing the stage helps define prognosis and is useful when selecting therapies. The most common system is the four-stage TNM system (abbreviated from Tumor/Nodes/Metastases). Its components include the size of the tumor, the number of involved lymph nodes, and the presence of any other metastases.
The most important distinction made by any staging system is whether or not the cancer is still confined to the prostate. In the TNM system, clinical T1 and T2 cancers are found only in the prostate, while T3 and T4 cancers have spread elsewhere. Several tests can be used to look for evidence of spread. These include computed tomography to evaluate spread within the pelvis, bone scans to look for spread to the bones, and endorectal coil magnetic resonance imaging to closely evaluate the prostatic capsule and the seminal vesicles. Bone scans should reveal osteoblastic appearance due to increased bone density in the areas of bone metastasis - opposite to what is found in many other cancers that metastasize.
Computed tomography (CT) and magnetic resonance imaging (MRI) currently do not add any significant information in the assessment of possible lymph node metastases in patients with prostate cancer according to a meta-analysis.[81] The sensitivity of CT was 42% and specificity of CT was 82%. The sensitivity of MRI was 39% and the specificity of MRI was 82%. For patients at similar risk to those in this study (17% had positive pelvic lymph nodes in the CT studies and 30% had positive pelvic lymph nodes in the MRI studies), this leads to a positive predictive value (PPV) of 32.3% with CT, 48.1% with MRI, and negative predictive value (NPV) of 87.3% with CT, 75.8% with MRI.
After a prostate biopsy, a pathologist looks at the samples under a microscope. If cancer is present, the pathologist reports the grade of the tumor. The grade tells how much the tumor tissue differs from normal prostate tissue and suggests how fast the tumor is likely to grow. The Gleason system is used to grade prostate tumors from 2 to 10, where a Gleason score of 10 indicates the most abnormalities. The pathologist assigns a number from 1 to 5 for the most common pattern observed under the microscope, then does the same for the second most common pattern. The sum of these two numbers is the Gleason score. The Whitmore-Jewett stage is another method sometimes used. Proper grading of the tumor is critical, since the grade of the tumor is one of the major factors used to determine the treatment recommendation.
Risk assessment
Many prostate cancers are not destined to be lethal, and most men will ultimately die from causes other than of the disease. Decisions about treatment type and timing may therefore be informed by an estimation of the risk that the tumor will ultimately recur after treatment and/or progress to metastases and mortality. Several tools are available to help predict outcomes such as pathologic stage and recurrence after surgery or radiation therapy. Most combine stage, grade, and PSA level, and some also add the number or percent of biopsy cores positive, age, and/or other information.
The D’Amico classification stratifies men to low, intermediate, or high risk based on stage, grade, and PSA. It is used widely in clinical practice and research settings. The major downside to the 3-level system is that it does not account for multiple adverse parameters (e.g., high Gleason score and high PSA) in stratifying patients.
The Partin tables predict pathologic outcomes (margin status, extraprostatic extension, and seminal vesicle invasion) based on the same 3 variables, and are published as lookup tables.
The Kattan nomograms predict recurrence after surgery and/or radiation therapy, based on data available either at time of diagnosis or after surgery. The nomograms can be calculated using paper graphs, or using software available on a website or for handheld computers. The Kattan score represents the likelihood of remaining free of disease at a given time interval following treatment.
The UCSF Cancer of the Prostate Risk Assessment (CAPRA) score predicts both pathologic status and recurrence after surgery. It offers comparable accuracy as the Kattan preoperative nomogram, and can be calculated without paper tables or a calculator. Points are assigned based on PSA, Grade, stage, age, and percent of cores positive; the sum yields a 0–10 score, with every 2 points representing roughly a doubling of risk of recurrence. The CAPRA score was derived from community-based data in the CaPSURE database. It has been validated among over 10,000 prostatectomy patients, including patients from CaPSURE; the SEARCH registry, representing data from several Veterans Administration and active military medical centers; a multi-institutional cohort in Germany; and the prostatectomy cohort at Johns Hopkins University.
Treatment
Treatment for prostate cancer may involve watchful waiting, surgery, radiation therapy including brachytherapy (prostate brachytherapy) and external beam radiation, High Intensity Focused Ultrasound (HIFU), chemotherapy, cryosurgery, hormonal therapy, or some combination. Which option is best depends on the stage of the disease, the Gleason score, and the PSA level. Other important factors are the man's age, his general health, and his feelings about potential treatments and their possible side effects. Because all treatments can have significant side effects, such as erectile dysfunction and urinary incontinence, treatment discussions often focus on balancing the goals of therapy with the risks of lifestyle alterations.
The selection of treatment options may be a complex decision involving many factors. For example, radical prostatectomy after primary radiation failure is a very technically challenging surgery and may not be an option.[82] This may enter into the treatment decision.
If the cancer has spread beyond the prostate, treatment options significantly change, so most doctors who treat prostate cancer use a variety of nomograms to predict the probability of spread. Treatment by watchful waiting, HIFU, radiation therapy, cryosurgery, and surgery are generally offered to men whose cancer remains within the prostate. Hormonal therapy and chemotherapy are often reserved for disease which has spread beyond the prostate. However, there are exceptions: radiation therapy may be used for some advanced tumors, and hormonal therapy is used for some early stage tumors. Cryotherapy, hormonal therapy, and chemotherapy may also be offered if initial treatment fails and the cancer progresses.
Active Surveillance
Active Surveillance refers to observation and regular monitoring without invasive treatment. Active surveillance is often used when an early stage, slow-growing prostate cancer is found in an older man. Conversely watchful waiting may also be suggested when the risks of surgery, radiation therapy, or hormonal therapy outweigh the possible benefits. Other treatments can be started if symptoms develop, or if there are signs that the cancer growth is accelerating (e.g., rapidly rising PSA, increase in Gleason score on repeat biopsy, etc.). Most men who choose active surveillance for early stage tumors eventually have signs of tumor progression, and they may need to begin treatment within three years.[83] Although men who choose active surveillance avoid the risks of surgery and radiation, the risk of metastasis (spread of the cancer) may be increased.
For younger men, a trial of active surveillance may not mean avoiding treatment altogether, but may reasonably allow a delay of a few years or more, during which time the quality of life impact of active treatment can be avoided. Published data to date suggest that carefully selected men will not miss a window for cure with this approach. Additional health problems that develop with advancing age during the observation period can also make it harder to undergo surgery and radiation therapy.
Natural Therapy
As an alternative to active surveillance or invasive treatments, which does nothing to change the course of disease, a growing number of clinicians and researchers are looking at non-invasive ways to help men with apparently localized prostate cancer. Perhaps most convincing among this group are Dean Ornish, MD and colleagues, previously made famous for showing that aggressive lifestyle changes can reverse atherosclerosis, and now showing that PSA can be lowered in men with apparent localized prostate cancer using a vegan diet (fish allowed), regular exercise, and stress reduction.[84] These results have so far proven durable after two-years' treatment.[85]
Many other single agents have been shown to reduce PSA, slow PSA doubling times, or have similar effects on secondary markers in men with localized cancer in short term trials, such as the Wonderful variety of pomegranate juice 8 oz daily or genistein, an isoflavone found in various legumes, 60 mg per day.[86][87] The potential of using multiple such agents in concert, let alone combining them with lifestyle changes, has not yet been studied but the potential is great. This is particularly true because most of these natural approaches have very low adverse effect rates, and in fact tend to help other risk factors and disease conditions such as atherosclerosis, diabetes, and risk for other cancers at the same time they are helping slow down prostate cancer. A more thorough review of natural approaches to prostate cancer has been published.[88]
Surgery
Surgical removal of the prostate, or prostatectomy, is a common treatment either for early stage prostate cancer, or for cancer which has failed to respond to radiation therapy. The most common type is radical retropubic prostatectomy, when the surgeon removes the prostate through an abdominal incision. Another type is radical perineal prostatectomy, when the surgeon removes the prostate through an incision in the perineum, the skin between the scrotum and anus. Radical prostatectomy can also be performed laparoscopically, through a series of small (1cm) incisions in the abdomen, with or without the assistance of a surgical robot.
Radical prostatectomy is effective for tumors which have not spread beyond the prostate;[89] cure rates depend on risk factors such as PSA level and Gleason grade. However, it may cause nerve damage that significantly alters the quality of life of the prostate cancer survivor.
Radical prostatectomy has traditionally been used alone when the cancer is small. In the event of positive margins or locally advanced disease found on pathology, adjuvant radiation therapy may offer improved survival. Surgery may also be offered when a cancer is not responding to radiation therapy. However, because radiation therapy causes tissue changes, prostatectomy after radiation has a higher risk of complications.
Laparoscopic radical prostatectomy, LRP, is a new way to approach the prostate surgically with intent to cure. Contrasted with the open surgical form of prostate cancer surgery, laparoscopic radical prostatectomy does not require a large incision. Relying on modern technology, such as miniaturization, fiber optics, and the like, laparoscopic radical prostatectomy is a minimally invasive prostate cancer treatment.
In the hands of an experienced surgeon, robotic assisted laparoscopic prostatectomy (RALP) may reduce positive surgical margins when compared to radical retropubic prostatectomy (RRP) among patients with prostate cancer according to a retrospective study.[81] The relative risk reduction was 57.7%. For patients at similar risk to those in this study (35.5% of patients had positive surgical margins following RRP), this leads to an absolute risk reduction of 20.5%. 4.9 patients must be treated for one to benefit (number needed to treat = 4.9). The relative merits of RALP and benefits over open radical prostatectomy are an area of intense research currently in urology and no definitive data, that has been widely accepted by the broader urological community, exists to say it is superior to a open radical retropubic prostatectomy.
Transurethral resection of the prostate, commonly called a "TURP," is a surgical procedure performed when the tube from the bladder to the penis (urethra) is blocked by prostate enlargement. TURP is generally for benign disease and is not meant as definitive treatment for prostate cancer. During a TURP, a small instrument (cystoscope) is placed into the penis and the blocking prostate is cut away.
In metastatic disease, where cancer has spread beyond the prostate, removal of the testicles (called orchiectomy) may be done to decrease testosterone levels and control cancer growth. (See hormonal therapy, below).
The most common serious complications of surgery are loss of urinary control and impotence. Reported rates of both complications vary widely depending on how they are assessed, by whom, and how long after surgery, as well as the setting (e.g., academic series vs. community-based or population-based data). Although penile sensation and the ability to achieve orgasm usually remain intact, erection and ejaculation are often impaired. Medications such as sildenafil (Viagra), tadalafil (Cialis), or vardenafil (Levitra) may restore some degree of potency. For most men with organ-confined disease, a more limited "nerve-sparing" technique may help reduce urinary incontinence and impotence.[90]
Radiation therapy

Radiation therapy, also known as radiotherapy, is often used to treat all stages of prostate cancer, or when surgery fails. Radiotherapy uses ionizing radiation to kill prostate cancer cells. When absorbed in tissue, Ionizing radiation such as Gamma and x-rays damage the DNA in cells, which increases the probability of apoptosis (cell death). Two different kinds of radiation therapy are used in prostate cancer treatment: external beam radiation therapy and brachytherapy (specifically prostate brachytherapy).
External beam radiation therapy uses a linear accelerator to produce high-energy x-rays which are directed in a beam towards the prostate. A technique called Intensity Modulated Radiation Therapy (IMRT) may be used to adjust the radiation beam to conform with the shape of the tumor, allowing higher doses to be given to the prostate and seminal vesicles with less damage to the bladder and rectum. External beam radiation therapy is generally given over several weeks, with daily visits to a radiation therapy center. New types of radiation therapy may have fewer side effects than traditional treatment. One of these is Tomotherapy.

Permanent implant brachytherapy is a popular treatment choice for patients with low to intermediate risk features, can be performed on an outpatient basis, and is associated with good 10-year outcomes with relatively low morbidity[91] It involves the placement of about 100 small "seeds" containing radioactive material (such as iodine-125 or palladium-103) with a needle through the skin of the perineum directly into the tumor while under spinal or general anesthetic. These seeds emit lower-energy X-rays which are only able to travel a short distance. Although the seeds eventually become inert, they remain in the prostate permanently. The risk of exposure to others from men with implanted seeds is generally accepted to be insignificant.[92]
Radiation therapy is commonly used in prostate cancer treatment. It may be used instead of surgery or after surgery in early stage prostate cancer. In advanced stages of prostate cancer radiation is used to treat painful bone metastases. Radiation treatments also can be combined with hormonal therapy for intermediate risk disease, when radiation therapy alone is less likely to cure the cancer. Some radiation oncologists combine external beam radiation and brachytherapy for intermediate to high risk situations. One study found that the combination of six months of androgen suppressive therapy combined with external beam radiation had improved survival compared to radiation alone in patients with localized prostate cancer.[93] Others use a "triple modality" combination of external beam radiation therapy, brachytherapy, and hormonal therapy.
Radiation therapy uses high-energy rays or particles to kill cancer cells.[94] When delivered in the correct dosage, radiation can reduce the risk of recurrence.
Less common applications for radiotherapy are when cancer is compressing the spinal cord, or sometimes after surgery, such as when cancer is found in the seminal vesicles, in the lymph nodes, outside the prostate capsule, or at the margins of the biopsy.
Radiation therapy is often offered to men whose medical problems make surgery more risky. Radiation therapy appears to cure small tumors that are confined to the prostate just about as well as surgery. However, some issues remain unresolved, such as whether radiation should be given to the rest of the pelvis, how much the absorbed dose should be, and whether hormonal therapy should be given at the same time.
Side effects of radiation therapy might occur after a few weeks into treatment. Both types of radiation therapy may cause diarrhea and mild rectal bleeding due to radiation proctitis, as well as urinary incontinence and impotence. Symptoms tend to improve over time. Rates for impotence when comparing radiation to nerve-sparing surgery are similar. Radiation has lower rates of incontinence but higher rates of occasional mild rectal bleeding.[95] Men who have undergone external beam radiation therapy may have a slightly higher risk of later developing colon cancer and bladder cancer.[96]
Cryosurgery
Cryosurgery is another method of treating prostate cancer in which the prostate gland is exposed to freezing temperatures.[97] It is less invasive than radical prostatectomy, and general anesthesia is less commonly used. Under ultrasound guidance, a method invented by Dr. Gary Onik,[98] metal rods are inserted through the skin of the perineum into the prostate. Highly purified Argon gas is used to cool the rods, freezing the surrounding tissue at −186 °C (−302 °F). As the water within the prostate cells freeze, the cells die. The urethra is protected from freezing by a catheter filled with warm liquid. Cryosurgery generally causes fewer problems with urinary control than other treatments, but impotence occurs up to ninety percent of the time. When used as the initial treatment for prostate cancer and in the hands of an experienced cryosurgeon, cryosurgery has a 10 year biochemical disease free rate superior to all other treatments including radical prostatectomy and any form of radiation.[99] Cryosurgery has also been demonstrated to be superior to radical prostatectomy for recurrent cancer following radiation therapy.
Hormonal therapy

Hormonal therapy uses medications or surgery to block prostate cancer cells from getting dihydrotestosterone (DHT), a hormone produced in the prostate and required for the growth and spread of most prostate cancer cells. Blocking DHT often causes prostate cancer to stop growing and even shrink. However, hormonal therapy rarely cures prostate cancer because cancers which initially respond to hormonal therapy typically become resistant after one to two years. Hormonal therapy is therefore usually used when cancer has spread from the prostate. It may also be given to certain men undergoing radiation therapy or surgery to help prevent return of their cancer.[100]
Hormonal therapy for prostate cancer targets the pathways the body uses to produce DHT. A feedback loop involving the testicles, the hypothalamus, and the pituitary, adrenal, and prostate glands controls the blood levels of DHT. First, low blood levels of DHT stimulate the hypothalamus to produce gonadotropin releasing hormone (GnRH). GnRH then stimulates the pituitary gland to produce luteinizing hormone (LH), and LH stimulates the testicles to produce testosterone. Finally, testosterone from the testicles and dehydroepiandrosterone from the adrenal glands stimulate the prostate to produce more DHT. Hormonal therapy can decrease levels of DHT by interrupting this pathway at any point. There are several forms of hormonal therapy:
- Orchiectomy is surgery to remove the testicles. Because the testicles make most of the body's testosterone, after orchiectomy testosterone levels drop. Now the prostate not only lacks the testosterone stimulus to produce DHT, but also it does not have enough testosterone to transform into DHT.
- Antiandrogens are medications such as flutamide, bicalutamide, nilutamide, and cyproterone acetate which directly block the actions of testosterone and DHT within prostate cancer cells.
- Medications which block the production of adrenal androgens such as DHEA include ketoconazole and aminoglutethimide. Because the adrenal glands only make about 5% of the body's androgens, these medications are generally used only in combination with other methods that can block the 95% of androgens made by the testicles. These combined methods are called total androgen blockade (TAB). TAB can also be achieved using antiandrogens.
- GnRH action can be interrupted in one of two ways. GnRH antagonists suppress the production of LH directly, while GnRH agonists suppress LH through the process of downregulation after an initial stimulation effect. Abarelix is an example of a GnRH antagonist, while the GnRH agonists include leuprolide, goserelin, triptorelin, and buserelin. Initially, GnRH agonists increase the production of LH. However, because the constant supply of the medication does not match the body's natural production rhythm, production of both LH and GnRH decreases after a few weeks.[101]
- A very recent Trial I study (N=21) found that Abiraterone Acetate caused dramatic reduction in PSA levels and Tumor sizes in aggressive end-stage prostate cancer for 70% of patients. This is prostate cancer that resists all other treatments (e.g., castration, other hormones, etc.). Officially the impacts on life-span are not yet known because subjects have not been taking the drug very long. Larger Trial III Clinical Studies are in the works. If successful an approved treatment is hoped for around 2011.[102][103]
The most successful hormonal treatments are orchiectomy and GnRH agonists. Despite their higher cost, GnRH agonists are often chosen over orchiectomy for cosmetic and emotional reasons. Eventually, total androgen blockade may prove to be better than orchiectomy or GnRH agonists used alone.
Each treatment has disadvantages which limit its use in certain circumstances. Although orchiectomy is a low-risk surgery, the psychological impact of removing the testicles can be significant. The loss of testosterone also causes hot flashes, weight gain, loss of libido, enlargement of the breasts (gynecomastia), impotence and osteoporosis. GnRH agonists eventually cause the same side effects as orchiectomy but may cause worse symptoms at the beginning of treatment. When GnRH agonists are first used, testosterone surges can lead to increased bone pain from metastatic cancer, so antiandrogens or abarelix are often added to blunt these side effects. Estrogens are not commonly used because they increase the risk for cardiovascular disease and blood clots. The antiandrogens do not generally cause impotence and usually cause less loss of bone and muscle mass. Ketoconazole can cause liver damage with prolonged use, and aminoglutethimide can cause skin rashes.
Palliative care
Palliative care for advanced stage prostate cancer focuses on extending life and relieving the symptoms of metastatic disease. As noted above Abiraterone Acetate is showing some promise in treating advance stage prostate cancer. It causes a dramatic reduction in PSA levels and Tumor sizes in aggressive advanced-stage prostate cancer for 70% of patients. Chemotherapy may be offered to slow disease progression and postpone symptoms. The most commonly used regimen combines the chemotherapeutic drug docetaxel with a corticosteroid such as prednisone.[104] Bisphosphonates such as zoledronic acid have been shown to delay skeletal complications such as fractures or the need for radiation therapy in patients with hormone-refractory metastatic prostate cancer.[105]
Bone pain due to metastatic disease is treated with opioid pain relievers such as morphine and oxycodone. External beam radiation therapy directed at bone metastases may provide pain relief. Injections of certain radioisotopes, such as strontium-89, phosphorus-32, or samarium-153, also target bone metastases and may help relieve pain.
High Intensity Focused Ultrasound (HIFU)
HIFU for prostate cancer utilizes high intensity focused ultrasound (HIFU) to ablate/destroy the tissue of the prostate. During the HIFU procedure, sound waves are used to heat the prostate tissue thus destroying the cancerous cells. Essentially, ultrasonic waves are precisely focused on specific areas of the prostate to eliminate the prostate cancer with minimal risks of affecting other tissue or organs. Temperatures at the focal point of the sound waves can exceed 100 °C (212 °F).[106] In lay terms, the HIFU technology is similar to using a magnifying glass to burn a piece of paper by focusing sunlight at a small precise point on the sheet. The ability to focus the ultrasonic waves leads to a relatively low occurrence of both incontinence and impotence. (0.6% and 0-20%, respectively)[107] According to international studies, when compared to other procedures, HIFU has a high success rate with a reduced risk of side effects. Studies using the Sonablate 500 HIFU machine have shown that 94% of patients with a pretreatment PSA (Prostate Specific Antigen) of less than 10 ng/mL were cancer-free after three years.[107] However, many studies of HIFU were performed by manufacturers of HIFU devices, or members of manufacturers' advisory panels.[108]
HIFU was first used in the 1940s and 1950s in efforts to destroy tumors in the central nervous system. Since then, HIFU has been shown to be effective at destroying malignant tissue in the brain, prostate, spleen, liver, kidney, breast, and bone.[106] Today, the HIF procedure for prostate cancer is performed using a transrectal probe. This procedure has been performed for over ten years and is currently approved for use in Japan, Europe, Canada, and parts of Central and South America.
Although not yet approved for use in the Unites States, many patients have received the HIFU procedure at facilities in Canada, and Central and South America. Currently, therapy is available using the Sonablate 500 or the Ablatherm. The Sonablate 500 is designed by Focus Surgery of Indianapolis, Indiana and is used in international HIFU centers around the world.
Prognosis
Prostate cancer rates are higher and prognosis poorer in developed countries than the rest of the world. Many of the risk factors for prostate cancer are more prevalent in the developed world, including longer life expectancy and diets high in red meat and dairy products (although it must be noted, that people who consume larger amounts of meat and dairy, also tend to consume fewer portions of fruits and vegetables. It's not currently known whether or not both of this factors, or just one of them, contributes to the occurrence of prostate cancer).[109] Also, where there is more access to screening programs, there is a higher detection rate. Prostate cancer is the ninth most common cancer in the world, but is the number one non-skin cancer in United States men. Prostate cancer affected eighteen percent of American men and caused death in three percent in 2005.[110] In Japan, death from prostate cancer was one-fifth to one-half the rates in the United States and Europe in the 1990s.[111] In India in the 1990s, half of the people with prostate cancer confined to the prostate died within ten years.[112] African-American men have 50–60 times more prostate cancer and prostate cancer deaths than men in Shanghai, China.[113] In Nigeria, two percent of men develop prostate cancer and 64% of them are dead after two years.[114]
In patients who undergo treatment, the most important clinical prognostic indicators of disease outcome are stage, pre-therapy PSA level and Gleason score. In general, the higher the grade and the stage, the poorer the prognosis. Nomograms can be used to calculate the estimated risk of the individual patient. The predictions are based on the experience of large groups of patients suffering from cancers at various stages.[115]
Progression
In 1941, Charles Huggins reported that androgen ablation therapy causes regression of primary and metastatic androgen-dependent prostate cancer.[116] Androgen ablation therapy causes remission in 80-90% of patients undergoing therapy, resulting in a median progression-free survival of 12 to 33 months. After remission an androgen-independent phenotype typically emerges, where the median overall survival is 23–37 months from the time of initiation of androgen ablation therapy.[117] The actual mechanism contributes to the progression of prostate cancer is not clear and may vary between individual patient. A few possible mechanisms have been proposed.[118] Scientists have established a few prostate cancer cell lines to investigate the mechanism involved in the progression of prostate cancer. LNCaP, PC-3, and DU-145 are commonly used prostate cancer cell lines. The LNCaP cancer cell line was established from a human lymph node metastatic lesion of prostatic adenocarcinoma. PC-3 and DU-145 cells were established from human prostatic adenocarcinoma metastatic to bone and to brain, respectively. LNCaP cells express androgen receptor (AR), however, PC-3 and DU-145 cells express very little or no AR. AR, an androgen-activated transcription factor, belongs to the steroid nuclear receptor family. Development of the prostate is dependent on androgen signaling mediated through AR, and AR is also important during the development of prostate cancer. The proliferation of LNCaP cells is androgen-dependent but the proliferation of PC-3 and DU-145 cells is androgen-insensitive.Elevation of AR expression is often observed in advanced prostate tumors in patients.[119][120] Some androgen-independent LNCaP sublines have been developed from the ATCC androgen-dependent LNCaP cells after androgen deprivation for study of prostate cancer progression. These androgen-independent LNCaP cells have elevated AR expression and express prostate specific antigen upon androgen treatment. Androgens paradoxically inhibit the proliferation of these androgen-independent prostate cancer cells.[121][122][123] Androgen at a concentration of 10-fold higher than the physiological concentration has also been shown to cause growth suppression and reversion of androgen-independent prostate cancer xenografts or androgen-independent prostate tumors derived in vivo model to an androgen-stimulated phenotype in athymic mice.[124][125] These observation suggest the possibility to use androgen to treat the development of relapsed androgen-independent prostate tumors in patients. Oral infusion of green tea polyphenols, a potential alternative therapy for prostate cancer by natural compounds, has been shown to inhibit the development, progression, and metastasis as well in autochthonous transgenic adenocarcinoma of the mouse prostate (TRAMP) model, which spontaneously develops prostate cancer.[126]
Epidemiology
Rates of prostate cancer vary widely across the world. Although the rates vary widely between countries, it is least common in South and East Asia, more common in Europe, and most common in the United States.[127] According to the American Cancer Society, prostate cancer is least common among Asian men and most common among black men, with figures for white men in-between.[128][129] However, these high rates may be affected by increasing rates of detection.[130]
Prostate cancer develops most frequently in men over fifty. This cancer can occur only in men, as the prostate is exclusively of the male reproductive tract. It is the most common type of cancer in men in the United States, where it is responsible for more male deaths than any other cancer, except lung cancer. In the United Kingdom it is also the second most common cause of cancer death after lung cancer, where around 35,000 cases are diagnosed every year and of which around 10,000 die of it. However, many men who develop prostate cancer never have symptoms, undergo no therapy, and eventually die of other causes. That is because malignant neoplasms of the prostate are, in most cases, slow-growing, and because most of those affected are over 60. Hence they often die of causes unrelated to the prostate cancer, such as heart/circulatory disease, pneumonia, other unconnected cancers or old age. Many factors, including genetics and diet, have been implicated in the development of prostate cancer. The Prostate Cancer Prevention Trial found that finasteride reduces the incidence of prostate cancer rate by 30%. There had been a controversy about this also increasing the risk of more aggressive cancers, but more recent research showed this was not the case.[131][132]
History

Although the prostate was first described by Venetian anatomist Niccolò Massa in 1536, and illustrated by Flemish anatomist Andreas Vesalius in 1538, prostate cancer was not identified until 1853.[133] Prostate cancer was initially considered a rare disease, probably because of shorter life expectancies and poorer detection methods in the 19th century. The first treatments of prostate cancer were surgeries to relieve urinary obstruction.[134] Removal of the entire gland (radical perineal prostatectomy) was first performed in 1904 by Hugh H. Young at Johns Hopkins Hospital.[135] Surgical removal of the testes (orchiectomy) to treat prostate cancer was first performed in the 1890s, but with limited success. Transurethral resection of the prostate (TURP) replaced radical prostatectomy for symptomatic relief of obstruction in the middle of the 20th century because it could better preserve penile erectile function. Radical retropubic prostatectomy was developed in 1983 by Patrick Walsh.[136] This surgical approach allowed for removal of the prostate and lymph nodes with maintenance of penile function.
In 1941 Charles B. Huggins published studies in which he used estrogen to oppose testosterone production in men with metastatic prostate cancer. This discovery of "chemical castration" won Huggins the 1966 Nobel Prize in Physiology or Medicine.[137] The role of the hormone GnRH in reproduction was determined by Andrzej W. Schally and Roger Guillemin, who both won the 1977 Nobel Prize in Physiology or Medicine for this work. Receptor agonists, such as leuprolide and goserelin, were subsequently developed and used to treat prostate cancer.[138][139]
Radiation therapy for prostate cancer was first developed in the early 20th century and initially consisted of intraprostatic radium implants. External beam radiation became more popular as stronger radiation sources became available in the middle of the 20th century. Brachytherapy with implanted seeds was first described in 1983.[140] Systemic chemotherapy for prostate cancer was first studied in the 1970s. The initial regimen of cyclophosphamide and 5-fluorouracil was quickly joined by multiple regimens using a host of other systemic chemotherapy drugs.[141]
See also
- Atypical small acinar proliferation
- Testosterone
References
- ↑ "IARC Worldwide Cancer Incidence Statistics—Prostate". JNCI Cancer Spectrum. Oxford University Press (December 19, 2001). Retrieved on 2007-04-05 through the Internet Archive
- ↑ Richard Warry. "Drug for deadly prostate cancer", BBC date = July 22, 2008. Retrieved on 2008-07-23.
- ↑ Aumüller, G. (1979). Prostate Gland and Seminal Vesicles. Berlin-Heidecool.lberg: Springer-Verlag.
- ↑ Moore, K.; Dalley, A. (1999). Clinically Oriented Anatomy. Baltimore, Maryland: Lippincott Williams & Wilkins.
- ↑ Steive, H. (1930). "Männliche Genitalorgane". Handbuch der mikroskopischen Anatomie des Menschen. Vol. VII Part 2. Berlin: Springer. pp. 1–399.
- ↑ Miller, DC; Hafez, KS, Stewart, A, et al (2003). "Prostate carcinoma presentation, diagnosis, and staging: an update from the National Cancer Data Base". Cancer 98: 1169. doi:. PMID 12973840.
- ↑ van der Cruijsen-Koeter, IW; Vis AN, Roobol MJ, Wildhagen MF, de Koning HJ, van der Kwast TH, Schroder FH (July 2005). "Comparison of screen detected and clinically diagnosed prostate cancer in the European randomized study of screening for prostate cancer, section rotterdam". Urol 174 (1): 121–5. doi:. PMID 15947595.
- ↑ Hsing, Ann W.; Anand P. Chokkalingam (May 1 2006). "Prostate cancer epidemiology". Frontiers in Bioscience 11: 1388–1413. doi:. http://www.bioscience.org/2006/v11/af/1891/fulltext.htm.
- ↑ Hankey, BF; Feuer EJ, Clegg LX, Hayes RB, Legler JM, Prorok PC, Ries LA, Merrill RM, Kaplan RS (June 16 1999). "Cancer surveillance series: interpreting trends in prostate cancer—part I: Evidence of the effects of screening in recent prostate cancer incidence, mortality, and survival rates". J Natl Cancer Inst 91 (12): 1017–24. doi:. PMID 10379964.
- ↑ Breslow, N; Chan CW, Dhom G, Drury RA, Franks LM, Gellei B, Lee YS, Lundberg S, Sparke B, Sternby NH, Tulinius H. (November 15 1977). "Latent carcinoma of prostate at autopsy in seven areas. The International Agency for Research on Cancer, Lyons, France". Int J Cancer 20 (5): 680–8. doi:. PMID 924691.
- ↑ Jemal A; Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, Feuer EJ, Thun MJ (Jan-Feb 2005). "Cancer statistics, 2005". CA Cancer J Clin 55 (1): 10–30. PMID 15661684. Erratum in: CA Cancer J Clin. 2005 Jul-Aug;55(4):259
- ↑ Hoffman, RM; Gilliland FD; Eley JW; Harlan LC; Stephenson RA; Stanford JL; Albertson PC; Hamilton AS; Hunt WC; Potosky AL (March 7 2001). "Racial and ethnic differences in advanced-stage prostate cancer: the Prostate Cancer Outcomes Study". J Natl Cancer Inst 93 (5): 388–95. doi:. PMID 11238701.
- ↑ Steinberg, GD; Carter BS; Beaty TH; Childs B; Walsh PC (1990). "Family history and the risk of prostate cancer". Prostate 17 (4): 337–47. doi:. PMID 2251225.
- ↑ Lichtenstein, P; Holm NV; Verkasalo PK; Iliadou A; Kaprio J; Koskenvuo M; Pukkala E; Skytthe A; Hemminki K (July 13 2000). "Environmental and heritable factors in the causation of cancer—analyses of cohorts of twins from Sweden, Denmark, and Finland". N Engl J Med 343 (2): 78–85. doi:. PMID 10891514.
- ↑ Struewing, JP; Hartge P; Wacholder S; Baker SM; Berlin M; McAdams M; Timmerman MM; Brody LC; Tucker MA (May 15 1997). "The risk of cancer associated with specific mutations of BRCA1 and BRCA2 among Ashkenazi Jews". N Engl J Med 336 (20): 1401–8. doi:. PMID 9145676.
- ↑ Gann, PH and Giovannucci (2005). "Prostate Cancer and Nutrition" (PDF). Retrieved on February 20, 2006. in .pdf format.
- ↑ Chavarro et al., "A prospective study of blood trans fatty acid levels and risk of prostate cancer," Proc. Amer. Assoc. Cancer Res., Volume 47, 2006 [1]. See also Ledesma 2004 Nutrition & prostate cancer.
- ↑ Peters U, Leitzmann MF, Chatterjee N, Wang Y, Albanes D, Gelmann EP, Friesen MD, Riboli E, Hayes RB (2007). "Serum lycopene, other carotenoids, and prostate cancer risk: a nested case-control study in the prostate, lung, colorectal, and ovarian cancer screening trial". Cancer Epidemiol. Biomarkers Prev. 16 (5): 962–8. doi:. PMID 17507623. http://cebp.aacrjournals.org/cgi/pmidlookup?view=long&pmid=17507623. Retrieved on 2007-12-17.
- ↑ Schulman, CC; Ekane S; Zlotta AR (September 2001). "Nutrition and prostate cancer: evidence or suspicion?". Urology 58 (3): 318–34. doi:. PMID 11549473.
- ↑ Jacobs, EJ; Rodriguez C, Mondul AM, Connell CJ, Henley SJ, Calle EE, Thun MJ (July 6 2005). "A large cohort study of aspirin and other nonsteroidal anti-inflammatory drugs and prostate cancer incidence". J Natl Cancer Inst 97 (13): 975–80. PMID 15998950.
- ↑ Shannon, J; Tewoderos S, Garzotto M, Beer TM, Derenick R, Palma A, Farris PE (August 15 2005). "Statins and prostate cancer risk: a case-control study". Am J Epidemiol 162 (4): 318–25. doi:. PMID 16014776. Epub 2005 July 13
- ↑ 22.0 22.1 22.2 Giles GG, Severi G, English DR, McCredie MR, Borland R, Boyle P, Hopper JL (August 2003). "Sexual factors and prostate cancer". BJU Int. 92 (3): 211–6. doi:. PMID 12887469.
- ↑ Leitzmann, Michael F. (April 7 2004). "Ejaculation Frequency and Subsequent Risk of Prostate Cancer". JAMA 291 (13): 1578–86. doi:. 2004;291:1578-1586. PMID 15069045.PMID: 15069045
- ↑ Dennis, LK; Lynch CF; Torner JC (July 2002). "Epidemiologic association between prostatitis and prostate cancer". Urology 60 (1): 78–83. doi:. PMID 12100928.
- ↑ Calle, EE; Rodriguez C, Walker-Thurmond K, Thun MJ (April 24 2003). "Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults". N Engl J Med 348 (17): 1625–38. doi:. PMID 12711737.
- ↑ Gann, PH; Hennekens CH, Ma J, Longcope C, Stampfer MJ (August 21 1996). "Prospective study of sex hormone levels and risk of prostate cancer". J Natl Cancer Inst 88 (16): 1118–26. doi:. PMID 8757191.
- ↑ "Veterans exposed to Agent Orange have higher rates of prostate cancer recurrence". Medical College of Georgia News (May 20, 2007).
- ↑ "Position of the American Dietetic Association and Dietitians of Canada: Vegetarian diets". J Am Diet Assoc 103 (6): 748–65. 2003. doi:. PMID 12778049.
- ↑ 29.0 29.1 29.2 "Masturbation 'cuts cancer risk'". Health. BBC NEWS (2003-07-16). Retrieved on 2008-04-24.
- ↑ Wigle DT, Turner MC, Gomes J, Parent ME (March 2008). "Role of hormonal and other factors in human prostate cancer". J Toxicol Environ Health B Crit Rev 11 (3-4): 242–59. doi:. PMID 18368555.
- ↑ Strom, SS; Yamamura Y, Duphorne CM, Spitz MR, Babaian RJ, Pillow PC, Hursting SD (1999). "Phytoestrogen intake and prostate cancer: a case-control study using a new database". Nutr Cancer 33 (1): 20–5. PMID 10227039. Erratum in: Nutr Cancer 2000;36(2):243.
- ↑ Steiner, MS; Pound, CR, Gingrich, JR, et al. (2002). "Acapodene (GTx-006) reduces high-grade prostatic intraepithelial neoplasia in phase II clinical trial (abstract)". Proc Am Soc Clin Oncol 21: 180a.
- ↑ Price, D; Stein, B, Goluboff, E, et al. (2005). "Double-blind, placebo-controlled trial of toremifene for the prevention of prostate cancer in men with high-grade prostatic intrapeithelial neoplasia (abstract)". J Clin Oncol 23: 106s.
- ↑ Thompson, IM; Goodman PJ, Tangen CM, Lucia MS, Miller GJ, Ford LG, Lieber MM, Cespedes RD, Atkins JN, Lippman SM, Carlin SM, Ryan A, Szczepanek CM, Crowley JJ, Coltman CA Jr. (July 17 2003). "The influence of finasteride on the development of prostate cancer". N Engl J Med 349 (3): 215–24. doi:. PMID 12824459.
- ↑ Andriole, GL; Roehrborn C, Schulman C, Slawin KM, Somerville M, Rittmaster RS (September 2004). "Effect of dutasteride on the detection of prostate cancer in men with benign prostatic hyperplasia". Urology 64 (3): 537–41; discussion 542–3. doi:. PMID 15351586.
- ↑ Gine Kolata. "New Take on a Prostate Drug, and a New Debate", NY Times date = June 15, 2008. Retrieved on 2008-06-15.
- ↑ Potosky A, Miller B, Albertsen P, Kramer B (2008). "Finasteride Does Not Increase the Risk of High-Grade Prostate Cancer: A Bias-Adjusted Modeling Approach". Cancer Prevention Research Published Online First on May 18, 2008 as 10.1158/1940-6207.CAPR-08-0092: 174. doi:. http://cancerpreventionresearch.aacrjournals.org/cgi/rapidpdf/1940-6207.CAPR-08-0092v1.
- ↑ Lee AH, Fraser ML, Meng X, Binns CW (April 2006). "Protective effects of green tea against prostate cancer". Expert Rev Anticancer Ther 6 (4): 507–13. doi:. PMID 16613539.
- ↑ Kikuchi N, Ohmori K, Shimazu T, et al (August 2006). "No association between green tea and prostate cancer risk in Japanese men: the Ohsaki Cohort Study". Br. J. Cancer 95 (3): 371–3. doi:. PMID 16804523.
- ↑ Bettuzzi S, Brausi M, Rizzi F, Castagnetti G, Peracchia G, Corti A (2006). "Chemoprevention of human prostate cancer by oral administration of green tea catechins in volunteers with high-grade prostate intraepithelial neoplasia: a preliminary report from a one-year proof-of-principle study". Cancer Res 66 (2): 1234–40. doi:. PMID 16424063.
- ↑ "Multivitamin prostate warning". Health. BBC NEWS (2007-05-16). Retrieved on 2008-04-23.
- ↑ Lawson KA, Wright ME, Subar A, Mouw T, Hollenbeck A, Schatzkin A, Leitzmann MF (May 2007). "Multivitamin use and risk of prostate cancer in the National Institutes of Health-AARP Diet and Health Study". J. Natl. Cancer Inst. 99 (10): 754–64. doi:. PMID 17505071.
- ↑ "Broccoli May Help Cut Prostate Cancer, Broccoli, Cauliflower May Make Aggressive Prostate Cancer Less Likely". CBS News (2007-07-24). Retrieved on 2008-04-23.
- ↑ Kirsh VA, Peters U, Mayne ST, Subar AF, Chatterjee N, Johnson CC, Hayes RB (August 2007). "Prospective study of fruit and vegetable intake and risk of prostate cancer". J. Natl. Cancer Inst. 99 (15): 1200–9. doi:. PMID 17652276.
- ↑ Sarkar FH, Li Y (December 2004). "Indole-3-carbinol and prostate cancer". J. Nutr. 134 (12 Suppl): 3493S–3498S. PMID 15570059.
- ↑ Hsu JC, Zhang J, Dev A, Wing A, Bjeldanes LF, Firestone GL (November 2005). "Indole-3-carbinol inhibition of androgen receptor expression and downregulation of androgen responsiveness in human prostate cancer cells". Carcinogenesis 26 (11): 1896–904. doi:. PMID 15958518. http://carcin.oxfordjournals.org/cgi/content/full/26/11/1896. Retrieved on 2008-09-12.
- ↑ [2]Giles, et al., Sexual factors and prostate cancer, BJU International, Volume 92 Issue 3, Ausust 2003, pp. 211-216
- ↑ Douglas Fox (2003-07-16). "Masturbating may protect against prostate cancer". New Scientist. Retrieved on 2008-04-23.
- ↑ Leitzmann MF, Platz EA, Stampfer MJ, Willett WC, Giovannucci E (April 2004). "Ejaculation frequency and subsequent risk of prostate cancer". JAMA 291 (13): 1578–86. doi:. PMID 15069045.
- ↑ Early Detection of Prostate Cancer, American Urological Association, Washington, D.C., revised: October 2008.Accessed: 12-01-2008
- ↑ USPSTF (December 2002). "Screening for Prostate Cancer". Agency for Healthcare Research and Quality. USPSTF (December 3, 2002). "Screening for prostate cancer: recommendation and rationale" (PDF). Ann Intern Med 137 (11): 915–6. PMID 12458992. http://www.annals.org/cgi/reprint/137/11/915.pdf.
Harris R, Lohr KN (December 3, 2002). "Screening for prostate cancer: an update of the evidence for the U.S. Preventive Services Task Force" (PDF). Ann Intern Med 137 (11): 917–29. PMID 12458993. http://www.annals.org/cgi/reprint/137/11/917.pdf. - ↑ Arias E (April 19, 2006). "United States Life Tables, 2003" (PDF). Natl Vital Stat Rep 54 (14): 1–40. PMID 16681183. http://www.cdc.gov/nchs/data/nvsr/nvsr54/nvsr54_14.pdf.
- ↑ von Eschenbach A, Ho R, Murphy GP, Cunningham M, Lins N (September-October 1997). "American Cancer Society guideline for the early detection of prostate cancer: update 1997" (PDF). CA Cancer J Clin 47 (5): 261–4. doi:. PMID 9314820. http://caonline.amcancersoc.org/cgi/reprint/47/5/261.pdf. ACS (March 28, 2007). "Prostate Cancer: Early Detection". Retrieved on 2007-11-19.
Smith RA, Cokkinides V, Eyre HJ (March-April 2007). "Cancer screening in the United States, 2007: a review of current guidelines, practices, and prospects" (PDF). CA Cancer J Clin 57 (2): 90–104. PMID 17392386. http://caonline.amcancersoc.org/cgi/reprint/57/2/90.pdf.
Smith RA, Cokkinides V, Eyre HJ (January-February 2006). "American Cancer Society guidelines for the early detection of cancer, 2006" (PDF). CA Cancer J Clin 56 (1): 11–25. PMID 16449183. http://caonline.amcancersoc.org/cgi/reprint/57/2/90.pdf. - ↑ ACS (March 29, 2007). "Chronological History of ACS Recommendations on Early Detection of Cancer".
- ↑ NCCN (May 10, 2007). "Prostate Cancer Early Detection V.2.2007" (PDF). NCCN Clinical Practice Guidelines in Oncology.
- ↑ "Study suggests value of regular PSA tests for tracking prostate cancer". Dana-Farber Cancer Institute (July 2004). Kladko B (August 15, 2005). "Prostate cancer test gets another look". The Boston Globe. http://www.boston.com/yourlife/health/men/articles/2005/08/15/prostate_cancer_test_gets_another_look/?page=full.
- ↑ Strum SB, Pogliano D (May 2005). "What every doctor who treats male patients should know" (PDF). PCRI Insights 8 (2): 4–5. http://www.prostate-cancer.org/resource/pdf/Is8-2.pdf.
- ↑ AUA (2008). "Prostate Cancer Patient Guide" (PDF). AUA Patient Guidelines.
- ↑ 59.0 59.1 Ross LE, Coates RJ, Breen N, Uhler RJ, Potosky AL, Blackman D (2004). "Prostate-specific antigen test use reported in the 2000 National Health Interview Survey". Prev Med 38 (6): 732–44. doi:. PMID 15193893.
- ↑ Lewis MH, Gohagan JK, Merenstein DJ (2007). "The locality rule and the physician's dilemma: local medical practices vs the national standard of care". JAMA 297 (23): 2633–7. doi:. PMID 17579232.
- ↑ Merenstein D (2004). "Winners and losers". JAMA 291 (1): 15–6. doi:. PMID 14709561.
- ↑ De Angelis G, Rittenhouse HG, Mikolajczyk SD, Blair Shamel L, Semjonow A (2007). "Twenty years of PSA: from prostate antigen to tumor marker". Rev Urol 9 (3): 113–23. PMID 17934568. http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=2002501&blobtype=pdf.
- ↑ Swan J, Breen N, Coates RJ, Rimer BK, Lee NC (2003). "Progress in cancer screening practices in the United States: results from the 2000 National Health Interview Survey". Cancer 97 (6): 1528–40. doi:. PMID 12627518. http://www3.interscience.wiley.com/cgi-bin/fulltext/103521394/PDFSTART.
- ↑ Ward E, Halpern M, Schrag N, Cokkinides V, DeSantis C, Bandi P, Siegel R, Stewart A, Jemal A (Jan-Feb 2008). "Association of insurance with cancer care utilization and outcomes" (PDF). CA Cancer J Clin 58 (1): 9–31. doi:. PMID 18096863. http://caonline.amcancersoc.org/cgi/reprint/58/1/9.pdf.
- ↑ Beaulac JA, Fry RN, Onysko J (2006). "Lifetime and recent prostate specific antigen (PSA) screening of men for prostate cancer in Canada". Can J Public Health 97 (3): 171–6. PMID 16827400.
- ↑ Gibbons L, Waters C (May 2003). "Prostate cancer--testing, incidence, surgery and mortality" (PDF). Health Rep 14 (3): 9–20. PMID 12816012. http://www.statcan.ca/english/studies/82-003/archive/2003/14-3-a.pdf.
- ↑ Chodak, GW; Keller P, Schoenberg HW (May 1989). "Assessment of screening for prostate cancer using the digital rectal examination". J Urol 141 (5): 1136–8. PMID 2709500.
- ↑ Krahn, MD; Mahoney JE, Eckman MH, Trachtenberg J, Pauker SG, Detsky AS (September 14 1994). "Screening for prostate cancer.. A decision analytic view". JAMA 272 (10): 773–80. doi:. PMID 7521400.
- ↑ Catalona WJ (August 16, 2007). "How I manage a patient with a newly elevated PSA" (PDF). 2007 CDC Cancer Conference.
- ↑ Kolota G (May 30, 2004). "It was medical gospel, but it wasn't true". The New York Times: p. 4.7. http://query.nytimes.com/gst/fullpage.html?res=9F05E5DD1E3EF933A05756C0A9629C8B63&sec=&spon=&pagewanted=all.
Thompson IM, Pauler DK, Goodman PJ, Tangen CM, Lucia MS, Parnes HL, Minasian LM, Ford LG, Lippman SM, Crawford ED, Crowley JJ, Coltman CA Jr (May 27, 2004). "Prevalence of prostate cancer among men with a prostate-specific antigen level < or =4.0 ng per milliliter". N Engl J Med 350 (22): 2239–46. PMID 15163773.
Carter HB (May 27, 2004). "Prostate cancers in men with low PSA levels--must we find them?". N Engl J Med 350 (22): 2292–4. doi:. PMID 15163780.
Catalona WJ, Richie JP, Ahmann FR, Hudson MA, Scardino PT, Flanigan RC, deKernion JB, Ratliff TL, Kavoussi LR, Dalkin BL, et al. (May 1994). "Comparison of digital rectal examination and serum prostate specific antigen in the early detection of prostate cancer: results of a multicenter clinical trial of 6,630 men". J Urol 151 (5): 1283–90. PMID 7512659.
FDA (August 29, 1994). "FDA approves test for prostate cancer". - ↑ Roobol, MJ; Kranse R, de Koning HJ, Schroder FH (February 2004). "Prostate-specific antigen velocity at low prostate-specific antigen levels as screening tool for prostate cancer: results of second screening round of ERSPC (ROTTERDAM)". Urology 63 (2): 309–13; discussion 313–5. doi:. PMID 14972478.
- ↑ Catalona, WJ; Richie JP, deKernion JB, Ahmann FR, Ratliff TL, Dalkin BL, Kavoussi LR, MacFarlane MT, Southwick PC (December 1994). "Comparison of prostate specific antigen concentration versus prostate specific antigen density in the early detection of prostate cancer: receiver operating characteristic curves". J Urol 152 (6 Pt 1): 2031–6. PMID 7525994.
- ↑ Hoffman, RM; Clanon DL, Littenberg B, Frank JJ, Peirce JC (October 2000). "Using the free-to-total prostate-specific antigen ratio to detect prostate cancer in men with nonspecific elevations of prostate-specific antigen levels". J Gen Intern Med 15 (10): 739–48. doi:. PMID 11089718.
- ↑ Partin, AW; Brawer MK; Bartsch G; Horninger W; Taneja SS; Lepor H; Babaian R; Childs SJ; Stamey T; Fritsche HA; Sokoll L; Chan DW; Thiel RP; Cheli CD (November 2003). "Complexed prostate specific antigen improves specificity for prostate cancer detection: results of a prospective multicenter clinical trial". J Urol 170 (5): 1787–91. doi:. PMID 14532777.
- ↑ Essink-Bot, ML; de Koning HJ, Nijs HG, Kirkels WJ, van der Maas PJ, Schroder FH (June 17 1998). "Short-term effects of population-based screening for prostate cancer on health-related quality of life". J Natl Cancer Inst 90 (12): 925–31. doi:. PMID 9637143.
- ↑ Chuang AY, Demarzo AM, Veltri RW, Sharma RB, Bieberich CJ, Epstein JI (2007). "Immunohistochemical Differentiation of High-grade Prostate Carcinoma From Urothelial Carcinoma". The American Journal of Surgical Pathology 31 (8): 1246–1255. doi:. PMID 17667550.
- ↑ Iyer M, Salazar FB, Lewis X, Zhang L, Wu L, Carey M and Gambhir SS. Non-invasive imaging of a transgenic mouse model using a prostate-specific two-step transcriptional amplification strategy. Transg Res.2005; 14(1): 47–55
- ↑ A Prostate Cancer Revolution. Newsweek, April 26, 2007.
- ↑ Hansel DE, DeMarzo AM, Platz EA, et al (2007). "Early prostate cancer antigen expression in predicting presence of prostate cancer in men with histologically negative biopsies". J. Urol. 177 (5): 1736–40. doi:. PMID 17437801.
- ↑ Ronquist G, Carlsson L, Larsson A, Nilsson BO: "Prostasomes: Proceedings from a symposium held at the Wenner-Gren Centre, Stockholm, June 2001" pp. 1-9. Portland Press , London
- ↑ 81.0 81.1 Smith JA, Chan RC, Chang SS, et al (2007). "A comparison of the incidence and location of positive surgical margins in robotic assisted laparoscopic radical prostatectomy and open retropubic radical prostatectomy". J. Urol. 178 (6): 2385–9; discussion 2389–90. doi:. PMID 17936849. http://linkinghub.elsevier.com/retrieve/pii/S0022-5347(07)01979-9.
- ↑ Mouraviev V, Evans B, Polascik TJ (2006). "Salvage prostate cryoablation after primary interstitial brachytherapy failure: a feasible approach". Prostate Cancer Prostatic Dis. 9 (1): 99–101. doi:. PMID 16314889.
- ↑ Wu, H; Sun L, Moul JW, Wu HY, McLeod DG, Amling C, Lance R, Kusuda L, Donahue T, Foley J, Chung A, Sexton W, Soderdahl D (March 2004). "Watchful waiting and factors predictive of secondary treatment of localized prostate cancer". J Urol 171 (3): 1111–6. doi:. PMID 14767282.
- ↑ Ornish, D; Weidner G, Fair WR, et al. (2005). "Intensive lifestyle changes may affect the progression of prostate cancer". J Urol 174 (3): 1065-70. PMID 16094059.
- ↑ Frattaroli, J; Weidner G, Kemp C, et al. (July 2008). "Clinical events in Prostate CAncer Lifestyle Trial: Results from two years of follow-up". Urology. PMID 18602144.
- ↑ Pantuck, AJ; Leppert JT, Zomorodian N, et al. (2006). "Phase II study of pomegranate juice for men with rising prostate-specific antigen following surgery or radiation for prostate cancer". Clin Cancer Res 12 (13): 4018-26. PMID 16818701.
- ↑ Kumar, NB; Cantor A, Allen K, et al. (2004). "The specific role of isoflavones in reducing prostate cancer risk". Prostate 59 (2): 141-7. PMID 15042614.
- ↑ Yarnell, E (1999). "A naturopathic approach to prostate cancer. Part 2: Guidelines for treatment and prevention". Altern Complemen Ther 5 (6): 360-8.
- ↑ Bill-Axelson A, Holmberg L, Ruutu M, et al (2005). "Radical prostatectomy versus watchful waiting in early prostate cancer". N. Engl. J. Med. 352 (19): 1977–84. doi:. PMID 15888698.
- ↑ Gerber, GS; Thisted RA, Scardino PT, Frohmuller HG, Schroeder FH, Paulson DF, Middleton AW Jr, Rukstalis DB, Smith JA Jr, Schellhammer PF, Ohori M, Chodak GW (August 28 1996). "Results of radical prostatectomy in men with clinically localized prostate cancer". JAMA 276 (8): 615–9. doi:. PMID 8773633.
- ↑ Nag, S; Beyer D, Friedland J, Grimm P, Nath R (? 1999). "American Brachytherapy Society Recommendations for Transperineal Permanent Brachytherapy of Prostate Cancer". Int. J. Rad. Onc. Biol. Phys. 44 (4): 789–799. ?. Review.
- ↑ Perez, CA; Hanks GE, Leibel SA, Zietman AL, Fuks Z, Lee WR (December 1 1993). "Localized carcinoma of the prostate (stages T1B, T1C, T2, and T3). Review of management with external beam radiation therapy". Cancer 72 (11): 3156–73. doi:. PMID 7694785. Review.
- ↑ D'Amico AV, Manola J, Loffredo M, Renshaw AA, DellaCroce A, Kantoff PW (2004). "6-month androgen suppression plus radiation therapy vs radiation therapy alone for patients with clinically localized prostate cancer: a randomized controlled trial". JAMA 292 (7): 821–7. doi:. PMID 15315996.
- ↑ American Cancer Society: Radiation Treatment
- ↑ Lawton, CA; Won M, Pilepich MV, Asbell SO, Shipley WU, Hanks GE, Cox JD, Perez CA, Sause WT, Doggett SR, et al (September 1991). "Long-term treatment sequelae following external beam irradiation for adenocarcinoma of the prostate: analysis of RTOG studies 7506 and 7706". Int J Radiat Oncol Biol Phys 21 (4): 935–9. PMID 1917622.
- ↑ Brenner, DJ; Curtis RE, Hall EJ, Ron E (January 15 2000). "Second malignancies in prostate carcinoma patients after radiotherapy compared with surgery". Cancer 88 (2): 398–406. doi:. PMID 10640974.
- ↑ PreventProstateCancer.info: A Brief Overview of Prostate Cancer [3]
- ↑ "Cryosurgical system for destroying tumors by freezing". Retrieved on 1994-08-02.
- ↑ Bahn, DK; Lee F, Badalament R, Kumar A, Greski J, Chernick M (August 2002). "Targeted cryoablation of the prostate: 7-year outcomes in the primary treatment of prostate cancer". Urology 60 (2 Suppl 1): 3–11. doi:. PMID 12206842.
- ↑ Robson, M; Dawson N (June 1996). "How is androgen-dependent metastatic prostate cancer best treated?". Hematol Oncol Clin North Am 10 (3): 727–47. doi:. PMID 8773508. Review.
- ↑ Loblaw, DA; Mendelson DS, Talcott JA, Virgo KS, Somerfield MR, Ben-Josef E, Middleton R, Porterfield H, Sharp SA, Smith TJ, Taplin ME, Vogelzang NJ, Wade JL Jr, Bennett CL, Scher HI; American Society of Clinical Oncology (July 15 2004). "American Society of Clinical Oncology recommendations for the initial hormonal management of androgen-sensitive metastatic, recurrent, or progressive prostate cancer". J Clin Oncol 22 (14): 2927–41. doi:. PMID 15184404. Erratum in: J Clin Oncol. 2004 November 1;22(21):4435.
- ↑ de Bono, Johann; Gerhardt Attard, Alison H.M. Reid, Timothy A. Yap, Florence Raynaud, Mitch Dowsett, Sarah Settatree, Mary Barrett, Christopher Parker, Vanessa Martins, Elizabeth Folkerd, Jeremy Clark, Colin S. Cooper, Stan B. Kaye, David Dearnaley, Gloria Lee (July 21 2004). "Phase I Clinical Trial of a Selective Inhibitor of CYP17, Abiraterone Acetate, Confirms That Castration-Resistant Prostate Cancer Commonly Remains Hormone Driven". J Clin Oncol: online. doi:. PMID 15184404. http://jco.ascopubs.org/cgi/content/abstract/JCO.2007.15.9749v1. Erratum in: J Clin Oncol. Early Release, published ahead of print July 21, 2008
- ↑ Richard Warry (July 22, 2008). "Drug for deadly prostate cancer", BBC. Retrieved on 2008-07-23.
- ↑ Tannock, IF; de Wit R, Berry WR, Horti J, Pluzanska A, Chi KN, Oudard S, Theodore C, James ND, Turesson I, Rosenthal MA, Eisenberger MA; TAX 327 Investigators (October 7 2004). "Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer". N Engl J Med 351 (15): 1502–12. doi:. PMID 1547021.
- ↑ Saad F, Gleason DM, Murray R, Tchekmedyian S, Venner P, Lacombe L, Chin JL, Vinholes JJ, Goas JA, Chen B (2002). "A randomized, placebo-controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinoma". J Natl Cancer Inst 94 (19): 1458–68. PMID 12359855.
- ↑ 106.0 106.1 Thomas A. Gardner and Michael A Koch, Indiana University Medical Center, Indianapolis. Prostate Cancer Therapy with High-Intensity Focused Ultrasound-Comprehensive Review. Clinical Genitourinary Cancer Vol 4. No.3, 2005.
- ↑ 107.0 107.1 Toyoaki Uchida, et al. Five years experience of transrectal high-intensity focused ultrasound using the Sonablate device in the treatment of localized prostate cancer. Dept of Urology University of Tokai Hachioji Hospital. International Journal of Urology
- ↑ Tom Pickles, Larry Goldenberg, Gary Steinhoff. High Intensity Focused Ultrasound for Prostate Cancer. British Columbia Cancer Agency http://www.bccancer.bc.ca/NR/rdonlyres/08EA1C8E-4345-4C7E-A83A-1F84853A1C27/8101/HIFUreport2005Feb10revised1.pdf
- ↑ ACS :: What Are The Risk Factors for Prostate Cancer?
- ↑ Jemal, A; Murray T; Ward E; Samuels A; Tiwari RC; Ghafoor A; Feuer EJ; Thun MJ (Jan-Feb 2005). "Cancer statistics, 2005". CA Cancer J Clin 55 (1): 10–30. PMID 15661684. Erratum in: CA Cancer J Clin. 2005 Jul-Aug;55(4):259.
- ↑ Wakai, K (February 2005). "Descriptive epidemiology of prostate cancer in Japan and Western countries". Nippon Rinsho 63 (2): 207–12. PMID 15714967. Review. (Japanese)
- ↑ Yeole, BB; Sunny L (Jun-Dec 2001). "Population based survival from prostate cancer in Mumbai (Bombay), India". Indian J Cancer 38 (2–4): 126–32. PMID 1259345.
- ↑ Hsing, AW; Tsao L, Devesa SS (January 1 2000). "International trends and patterns of prostate cancer incidence and mortality". Int J Cancer 85 (1): 60–7. doi:. PMID 10585584.
- ↑ Osegbe, DN (April 1997). "Prostate cancer in Nigerians: facts and nonfacts". J Urol 157 (4): 1340–3. doi:. PMID 9120935.
- ↑ Di Blasio CJ, Rhee AC, Cho D, Scardino PT, Kattan MW (2003). "Predicting clinical end points: treatment nomograms in prostate cancer". Semin Oncol 30 (5): 567–86. doi:. PMID 14571407.
- ↑ Huggins C, Steven RE and Hodges CV, Studies on prostatic cancer. Arch. Sug. 43:209–223, 1941.
- ↑ Hellerstedt BA and Pienta KJ, The current state of hormonal therapy for prostate cancer, CA Cancer J. Clin. 52: 154–179, 2002.PMID 12018929
- ↑ Feldman BJ, Feldman D. The development of androgen-independent prostate cancer. Nat Rev Cancer. 2001 Oct;1(1):34–45. PMID 11900250
- ↑ Linja MJ, Savinainen KJ, Saramaki OR, Tammela TL, Vessella RL, Visakorpi T. Amplification and overexpression of androgen receptor gene in hormone-refractory prostate cancer. Cancer Res. 2001 May 1;61(9):3550–5. PMID 11325816
- ↑ Ford OH 3rd, Gregory CW, Kim D, Smitherman AB, Mohler JL. Androgen receptor gene amplification and protein expression in recurrent prostate cancer. J Urol. 2003 Nov;170(5):1817–21.PMID 14532783
- ↑ Kokontis J, Takakura K, Hay N, Liao S. Increased androgen receptor activity and altered c-myc expression in prostate cancer cells after long-term androgen deprivation. Cancer Res. 1994 March 15;54(6):1566–73. PMID 7511045
- ↑ Umekita Y, Hiipakka RA, Kokontis JM, Liao S. Human prostate tumor growth in athymic mice: inhibition by androgens and stimulation by finasteride. Proc Natl Acad Sci U S A. 1996 October 15;93(21):11802-7. PMID 8876218
- ↑ Kokontis JM, Hsu S, Chuu CP, Dang M, Fukuchi J, Hiipakka RA, Liao S. Role of androgen receptor in the progression of human prostate tumor cells to androgen independence and insensitivity. Prostate. 2005 December 1;65(4):287-98. PMID 16015608
- ↑ Chuu CP, Hiipakka RA, Fukuchi J, Kokontis JM, Liao S. Androgen causes growth suppression and reversion of androgen-independent prostate cancer xenografts to an androgen-stimulated phenotype in athymic mice. Cancer Res. 2005 March 15;65(6):2082–4. PMID 15781616
- ↑ Chuu CP, Hiipakka RA, Kokontis JM, Fukuchi J, Chen RY, Liao S. Inhibition of tumor growth and progression of LNCaP prostate cancer cells in athymic mice by androgen and liver X receptor agonist. Cancer Res. 2006 July 1;66(13):6482–6. PMID 16818617
- ↑ Gupta S, Hastak K, Ahmad N, Lewin JS, Mukhtar H. Inhibition of prostate carcinogenesis in TRAMP mice by oral infusion of green tea polyphenols. Proc Natl Acad Sci U S A. 2001 August 28;98(18):10350-5. PMID 11504910
- ↑ "IARC Worldwide Cancer Incidence Statistics—Prostate". JNCI Cancer Spectrum. Oxford University Press (December 19, 2001). Retrieved on 2007-04-05 through the Internet Archive
- ↑ Overview: Prostate Cancer—What Causes Prostate Cancer? American Cancer Society (2006-05-02). Retrieved on 2007-04-05
- ↑ Prostate Cancer FAQs. State University of New York School of Medicine Department of Urology (2006-08-31). Retrieved on 2007-04-05
- ↑ Potosky A, Miller B, Albertsen P, Kramer B (1995). "The role of increasing detection in the rising incidence of prostate cancer". JAMA 273 (7): 548–52. doi:. PMID 7530782.
- ↑ Gine Kolata (June 15, 2008). "New Take on a Prostate Drug, and a New Debate", NY Times. Retrieved on 2008-06-15.
- ↑ Potosky A, Miller B, Albertsen P, Kramer B (2008). "Finasteride Does Not Increase the Risk of High-Grade Prostate Cancer: A Bias-Adjusted Modeling Approach". Cancer Prevention Research Published Online First on May 18, 2008 as 10.1158/1940-6207.CAPR-08-0092: 174. doi:. http://cancerpreventionresearch.aacrjournals.org/cgi/rapidpdf/1940-6207.CAPR-08-0092v1.
- ↑ Adams, J. The case of scirrhous of the prostate gland with corresponding affliction of the lymphatic glands in the lumbar region and in the pelvis. Lancet 1, 393 (1853).
- ↑ Lytton, B. Prostate cancer: a brief history and the discovery of hormonal ablation treatment. J. Urol. 165, 1859–1862
- ↑ Young, H. H. Four cases of radical prostatectomy. Johns Hopkins Bull. 16, 315 (1905).
- ↑ Walsh, P. C., Lepor, H. & Eggleston, J. C. Radical prostatectomy with preservation of sexual function: anatomical and pathological considerations. Prostate 4, 473-485 (1983). PMID 6889192
- ↑ Huggins, C. B. & Hodges, C. V. Studies on prostate cancer: 1. The effects of castration, of estrogen and androgen injection on serum phosphatases in metastatic carcinoma of the prostate. Cancer Res. 1, 203 (1941).
- ↑ Schally, A. V., Kastin, A. J. & Arimura, A. Hypothalamic FSH and LH-regulating hormone. Structure, physiology and clinical studies. Fertil. Steril. 22, 703–721 (1971).
- ↑ Tolis G, Ackman D, Stellos A, Mehta A, Labrie F, Fazekas AT, Comaru-Schally AM, Schally AV. Tumor growth inhibition in patients with prostatic carcinoma treated with luteinizing hormone-releasing hormone agonists. Proc Natl Acad Sci U S A. 1982 Mar;79(5):1658–62 PMID 6461861
- ↑ Denmeade SR, Isaacs JT. A History of Prostate Cancer Treatment. Nature Reviews Cancer 2, 389–396 (2002). PMID 12044015
- ↑ Scott, W. W. et al. Chemotherapy of advanced prostatic carcinoma with cyclophosphamide or 5-fluorouracil: results of first national randomized study. J. Urol. 114, 909–911 (1975). PMID 1104900
External links
- Prostate Cancer & Endothelin: PMAP The Proteolysis Map-animation
- Prostate cancer at the Open Directory Project
|
||||||||||||||||||||||||||||||||||||