Periodontitis
| Periodontal disease Classification and external resources |
|
 |
|
|---|---|
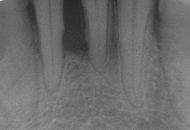
| This radiograph shows significant bone loss between the two roots of a tooth. The spongy bone has receded due to infection under tooth, reducing the bony support for the tooth. | |
| ICD-10 | K05.4 |
| DiseasesDB | 29362 |
| MedlinePlus | 001059 |
Periodontitis (peri = around, odont = tooth, -itis = inflammation) refers to a number of inflammatory diseases affecting the periodontium — that is, the tissues that surround and support the teeth. Periodontitis involves progressive loss of the alveolar bone around the teeth, and if left untreated, can lead to the loosening and subsequent loss of teeth. Periodontitis is caused by a convergence of bacteria that adhere to and grow on the tooth's surfaces, along with an overly aggressive immune response against these bacteria. A diagnosis of periodontitis is established by inspecting the soft gum tissues around the teeth with a probe and radiographs by visual analysis, to determine the amount of bone loss around the teeth. Specialists in the treatment of periodontitis are periodontists; their field is known as "periodontology" and "periodontics".
Although the different forms of periodontitis are all caused by bacterial infections, a variety of factors affect the severity of the disease. Important "risk factors" include smoking, poorly-controlled diabetes, and inherited (genetic) susceptibility.[1] This genetic susceptibility to destructive periodontal disease can now be tested with the PST® test, however the efficacy of this test remains to be studied in a long-term peer-reviewed prospective trials.
Contents |
Epidemiology
Periodontitis is very common, and is widely regarded as the second most common disease worldwide, after dental decay, and in the United States has a prevalence of 30-50% of the population, but only about 10% have severe forms.
Studies found association between ethnic origin and periodontal diseases. In the USA, higher prevalence of periodontal disease was observed among Afro-American individuals in comparison to Latin individuals as well as non-Hispanic Caucasian people. In Israeli population, individuals of Yemenite, North-African, Asian, or Mediterranean origin have higher prevalence of periodontal disease than individuals from Israeli or European descent.[1] This could be attributed to genetic predisposition as well as social-cultural-behavioral differences (eg., smoking, oral hygiene, access to dental treatment) between populations.[1]
Etiology
Periodontitis is an inflammation of the periodontium—the tissues that support the teeth in the mouth. The periodontium consists of four tissues:
- the gingiva, or gum tissue;
- the cementum, or outer layer of the roots of teeth;
- the alveolar bone, or the bony sockets into which the teeth are anchored;
- the periodontal ligaments (PDLs), which are the connective tissue fibers that run between the cementum and the alveolar bone.

If left untreated, periodontitis causes progressive, irreversible bone loss around teeth, looseness of the teeth and eventual tooth loss. Periodontitis is a very common disease affecting approximately 50% of U.S. adults over the age of 30 years. Periodontitis is thought to occur in people who have preexisting gingivitis — an inflammation that is limited to the soft tissues surrounding the tooth and does not yet affect the alveolar bone.
The primary etiology, or cause, of gingivitis is the accumulation of a bacterial matrix at the gum line, called dental plaque. Other contributors are poor nutrition and underlying medical issues such as diabetes. A double blind study showed a supplement that decreased pocket depth and bleeding. New FDA-approved finger nick tests are being used in dental offices to identify and screen patients for possible contributory causes of gum disease such as diabetes.In some people, gingivitis progresses to periodontitis - with the destruction of the gingival fibers, the gum tissues separate from the tooth and deepened sulcus, called a periodontal pocket. Subgingival bacteria (those that exist under the gum line) colonize the periodontal pockets and cause further inflammation in the gum tissues and progressive bone loss. Examples of secondary etiology would be those things that, by definition, cause plaque accumulation, such as restoration overhangs and root proximity.

If left undisturbed, bacterial plaque calcifies to form calculus, which is commonly called tartar. Calculus above and below the gum line must be removed completely by the dental hygienist or dentist to treat gingivitis and periodontitis. Although the primary cause of both gingivitis and periodontitis is the bacterial plaque that adheres to the tooth surface, there are many other modifying factors. A very strong risk factor is one's genetic susceptibility. Several conditions and diseases, including Down syndrome, diabetes, and other diseases that affect one's resistance to infection also increase susceptibility to periodontitis.
Another factor that makes periodontitis a difficult disease to study is that human host response can also affect the alveolar bone resorption. Host response to the bacterial insult is mainly determined by genetics; however, immune development may play some role in susceptibility.
Signs and symptoms
Symptoms may include the following:
- Occasional redness or bleeding of gums while brushing teeth, using dental floss or biting into hard food (e.g. apples) (though this may occur even in gingivitis, where there is no attachment loss)
- Occasional gum swellings that recurs
- Halitosis, or bad breath, and a persistent metallic taste in the mouth
- Gingival recession, resulting in apparent lengthening of teeth. (This may also be caused by heavy handed brushing or with a stiff tooth brush.)
- Deep pockets between the teeth and the gums (pockets are sites where the attachment has been gradually destroyed by collagen-destroying enzymes, known as collagenases)
- Loose teeth, in the later stages (though this may occur for other reasons as well)
Patients should realize that the gingival inflammation and bone destruction are largely painless. Hence, people may wrongly assume that painless bleeding after teeth cleaning is insignificant, although this may be a symptom of progressing periodontitis in that patient.
Prevention
Daily oral hygiene measures to prevent periodontal disease include:
- Brushing properly on a regular basis (at least twice daily), with the patient attempting to direct the toothbrush bristles underneath the gum-line, so as to help disrupt the bacterial growth and formation of subgingival plaque.
- Flossing daily and using interdental brushes (if there is a sufficiently large space between teeth), as well as cleaning behind the last tooth in each quarter.
- Using an antiseptic mouthwash. Chlorhexidine gluconate based mouthwash or hydrogen peroxide in combination with careful oral hygiene may cure gingivitis, although they cannot reverse any attachment loss due to periodontitis.
- Using periodontal trays to maintain hydrogen peroxide or other dentist-prescribed medications at the source of the disease. The use of trays allows the medication to stay in place long enough to penetrate the biofilms where the bacteria are found.
- Regular dental check-ups and professional teeth cleaning as required. Dental check-ups serve to monitor the person's oral hygiene methods and levels of attachment around teeth, identify any early signs of periodontitis, and monitor response to treatment.
Typically dental hygienists (or dentists) use special instruments to clean (debride) teeth below the gumline and disrupt any plaque growing below the gumline. This is a standard treatment to prevent any further progress of established periodontitis. Studies show that after such a professional cleaning (periodontal debridement), bacteria and plaque tend to grow back to pre-cleaning levels after about 3-4 months. Hence, in theory, cleanings every 3-4 months might be expected to also prevent the initial onset of periodontitis. However, analysis of published research has reported little evidence either to support this or the intervals at which this should occur.[2] Instead it is advocated that the interval between dental check-ups should be determined specifically for each patient between every 3 to 24 months.[3][4]
Nonetheless, the continued stabilization of a patient's periodontal state depends largely, if not primarily, on the patient's oral hygiene at home if not on the go too. Without daily oral hygiene, periodontal disease will not be overcome, especially if the patient has a history of extensive periodontal disease.
Treatment of established disease

The cornerstone of successful periodontal treatment starts with establishing excellent oral hygiene. This includes twice daily brushing with daily flossing, mouthwash use. Also the use of an interdental brush (called a Proxi-brush) is helpful if space between the teeth allows. Persons with dexterity problems such as arthritis may find oral hygiene to be difficult and may require more frequent professional care. Persons with periodontitis must realize that it is a chronic inflammatory disease and a lifelong regimen of excellent hygiene and professional maintenance care with a dentist or periodontist is required to maintain affected teeth.
Initial therapy: Removal of bacterial plaque and calculus is necessary to establish periodontal health. The first step in the treatment of periodontitis involves non-surgical cleaning below the gumline with a procedure called Scaling and Root planing. This procedure involves use of specialized curettes to mechanically remove plaque and calculus from below the gumline, and may require multiple visits and local anesthesia to adequately complete. In addition to initial scaling and root planing, it may also be necessary to adjust the occlusion (bite) to prevent excessive force on teeth with reduced bone support. Also it may be necessary to complete any other dental needs such as replacement of rough, plaque retentive restorations, closure of open contacts between teeth, and any other requirements diagnosed at the initial evaluation.
Reevaluation: Multiple clinical studies have shown that non-surgical scaling and root planing is rarely successful in periodontal pocket depths greater than 4-5mm (See articles by Stambaugh RV, Int J Periodontics Rest Dent, 1981 or Waerhaug J, J Periodontol, 1978). Therefore it is necessary for the dentist or periodontist to perform a reevaluation 4-6 weeks after the initial scaling and root planing, to determine if the treatment was successful in reducing pocket depths and eliminating inflammation. It has been found that pocket depths which remain after initial therapy of greater than 5-6mm with bleeding upon probing are indicative of continued active disease and will very likely show further bone loss over time. This is especially true in molar tooth sites where furcations (areas between the roots) have been exposed.
Surgery: If the initial non-surgical treatment was not successful in controlling periodontitis, or if anatomical bony defects persist, periodontal surgery may be necessary to control periodontal disease. There are a myriad of procedures which may be applied, depending on each tooth's site-specific disease pattern. These procedures are usually performed by a periodontist. These procedures include (but are not limited to):
- Open flap debridement
- Modified Widman flap surgery
- Apically positioned flaps with or without osseous resection
- Guided tissue regeneration with or without bone grafting
Maintenance: Once successful periodontal treatment has been completed, with or without surgery, a lifelong regimen of "periodontal maintenance" is required. This involves regular checkups and cleanings of every 3-4 months to prevent repopulation of periodontitis-causing bacteria, and to closely monitor affected teeth so that early treatment can be rendered if disease recurs.
Assessment and prognosis
Dentists and dental hygienists "measure" periodontal disease using a device called a periodontal probe. This is a thin "measuring stick" that is gently placed into the space between the gums and the teeth, and slipped below the gum-line. If the probe can slip more than 3 millimetres length below the gum-line, the patient is said to have a "gingival pocket" around that tooth. This is somewhat of a misnomer, as any depth is in essence a pocket, which in turn is defined by its depth, i.e., a 2 mm pocket or a 6 mm pocket. However, it is generally accepted that pockets are self-cleansable (at home, by the patient, with a toothbrush) if they are 3 mm or less in depth. This is important because if there is a pocket which is deeper than 3 mm around the tooth, at-home care will not be sufficient to cleanse the pocket, and professional care should be sought. When the pocket depths reach 5, 6 and 7 mm in depth, even the hand instruments and cavitrons used by the dental professionals cannot reach deeply enough into the pocket to clean out the bacterial plaque that cause gingival inflammation. In such a situation the pocket or the gums around that tooth will always have inflammation which will likely result in bone loss around that tooth. The only way to stop the inflammation would be for the patient to undergo some form of gingival surgery to access the depths of the pockets and perhaps even change the pocket depths so that they become 3 or less mm in depth and can once again be properly cleaned by the patient at home with his or her toothbrush.
If a patient has 5 mm or deeper pockets around their teeth, then they would risk eventual tooth loss over the years. If this periodontal condition is not identified and the patient remains unaware of the progressive nature of the disease then, years later, they may be surprised that some teeth will gradually become loose and may need to be extracted, sometimes due to a severe infection or even pain.
According to the Sri Lankan Tea Labourer study, in the absence of any oral hygiene activity, approximately 10% will suffer from severe periodontal disease with rapid loss of attachment (>2 mm/year). 80% will suffer from moderate loss (1-2 mm/year) and the remaining 10% will not suffer any loss.[5][6]
See also
- Periodontist
- Actinomyces naeslundii, a kind of bacterium
- Calculus (dental), tartar
- Campylobacter, a kind of bacterium
- Dental plaque, bacterial biofilm that clings to teeth
- Halitosis, bad breath due to oral bacteria
- Oral hygiene, how to promote good health of the mouth
- Edentulism, condition of one or more missing teeth
- Gingivitis, inflammation of the gums
- Gum graft, a type of gum surgery, to replace lost gum tissue
- Head and neck anatomy, biological composition above the shoulders
- Osteoimmunology, studies the immune system with respect to bones
- Oral microbiology, study of the microorganisms of the oral cavity
- LANAP, Laser Assisted New Attachement Procedure
Further reading
- Pihlstrom, BL; Michalowicz BS, Johnson NW (2005). "Periodontal diseases". Lancet 366 (9499): 1809–20. doi:. ISSN 0140-6736. PMID 16298220.
Footnotes
- ↑ 1.0 1.1 1.2 Zadik Y, Bechor R, Sochat Z, Galor S (April 2008). "Ethnic origin and alveolar bone loss in Israeli adults". J Isr Dent Assoc 25 (2): 19-22. PMID 18780541. http://www.ncbi.nlm.nih.gov/pubmed/18780541?ordinalpos=2&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DefaultReportPanel.Pubmed_RVDocSum. Retrieved on 2008-09-11.
- ↑ Beirne P, Forgie A, Clarkson J, Worthington HV (2005). "Recall intervals for oral health in primary care patients". Cochrane Database for Systematic Reviews (2): CD004346. doi:. ISSN 1469-493X. PMID 15846709.
- ↑ National Institute for Health and Clinical Excellence (27 October, 2004). "NICE guidance issued on frequency of dental check-ups". National Library for Health (UK). Retrieved on 2006-05-07.
- ↑ BBC News (27 October, 2004). "Call for tailored dental checks - Routine six-monthly dental check-ups should become a thing of the past, new guidance recommends". Retrieved on 2006-05-07.
- ↑ Preus HR, Anerud A, Boysen H, Dunford RG, Zambon JJ, Loe H (1995). "The natural history of periodontal disease. The correlation of selected microbiological parameters with disease severity in Sri Lankan tea workers". J Clin Periodontol 22 (9): 674–8. doi:. PMID 7593696.
- ↑ Ekanayaka A (1984). "Tooth mortality in plantation workers and residents in Sri Lanka". Community Dent Oral Epidemiol 12 (2): 128–35. doi:. PMID 6584263.
External links
- PERIOBLOG: Clases y artículos de Periodoncia - Cátedra de Periodoncia II de la Facultad de Odontología de la UNMSM, Decana de América a cargo del Dr. Sixto Grados Pomarino
- Mayo Clinic
- Canadian Academy of Periodontology - What is periodontitis?
- Healthy behaviors equal healthy gums - An article from ADA (American Dental Association)
- Perio Trays - Non-invasive treatment for periodontitis
|
||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||