Methotrexate
 |
|
 |
|
|
Methotrexate
|
|
| Systematic (IUPAC) name | |
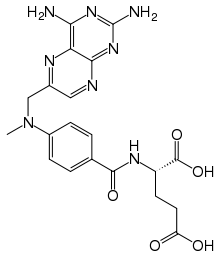
| (S)-2-(4-(((2,4-diaminopteridin-6-yl)methyl) (methyl)amino)benzamido)pentanedioic acid | |
| Identifiers | |
| CAS number | |
| ATC code | L01 L04 |
| PubChem | |
| DrugBank | |
| ChemSpider | |
| Chemical data | |
| Formula | C20H22N8O5 |
| Mol. mass | 454.44 g/mol |
| Pharmacokinetic data | |
| Bioavailability | 17–90% |
| Metabolism | hepatic |
| Half life | 3–15 hours (dose dependent) |
| Excretion | renal 48–100% |
| Therapeutic considerations | |
| Pregnancy cat. | |
| Legal status | |
| Routes | oral, IV, IM, SC, intrathecal |
Methotrexate (rINN) (pronounced /mɛθəˈtrɛkseɪt/), abbreviated MTX and formerly known as amethopterin, is an antimetabolite and antifolate drug used in treatment of cancer and autoimmune diseases. It acts by inhibiting the metabolism of folic acid. Methotrexate replaced the more powerful and toxic antifolate aminopterin, and the two should not be confused with each other.
Contents |
History
Methotrexate originated in the 1940s when Dr. Sidney Farber at Children's Hospital Boston was testing the effects of folic acid on acute leukemic children (severe blood cancer). Inspired, he asked Dr. Y. SubbaRow, then Director of the Research Division of Lederle Labs (part of American Cyanamid), to synthesize the anti-folate (methotrexate). Dr. Row, who also happened to be the head of the team which had earlier synthesized folic acid (1946) readily synthesized this anti-folate and handed it over to Dr. Farber, who in turn administered it to a small group of very ill leukemic children. The remarkable clinical improvement that was observed in these patients heralded the era of cancer chemotherapy in modern medicine. This was reported by Dr. S. Farber in the June 3rd, 1948 issue of NEJM. In 1950 Dr. Farber founded in Boston the world's first Cancer Research Center. Methotrexate gained Food and Drug Administration (FDA) approval as an oncology drug in 1953.
Mode of action
Methotrexate competitively and reversibly inhibits dihydrofolate reductase (DHFR), an enzyme that participates in the tetrahydrofolate synthesis. The affinity of methotrexate for DHFR is about one thousand-fold that of folate for DHFR. Dihydrofolate reductase catalyses the conversion of dihydrofolate to the active tetrahydrofolate. Folic acid is needed for the de novo synthesis of the nucleoside thymidine, required for DNA synthesis. Also, folate is needed for purine base synthesis, so all purine synthesis will be inhibited. Methotrexate, therefore, inhibits the synthesis of DNA, RNA, thymidylates, and proteins.
Methotrexate acts specifically during DNA and RNA synthesis, and thus it is cytotoxic during the S-phase of the cell cycle. Logically, it therefore has a greater toxic effect on rapidly dividing cells (such as malignant and myeloid cells, and GI & oral mucosa), which replicate their DNA more frequently, and thus inhibits the growth and proliferation of these non-cancerous cells as well as causing the side effects listed above.
Lower doses of methotrexate have been shown to be very effective for the management of rheumatoid arthritis, Crohn's disease, and psoriasis. In these cases inhibition of dihydrofolate reductase (DHFR) is not thought to be the main mechanism, but rather the inhibition of enzymes involved in purine metabolism, leading to accumulation of adenosine, or the inhibition of T cell activation and suppression of intercellular adhesion molecule expression by T cells.[1]
Uses
In cancer chemotherapy
Methotrexate was originally used as part of combination chemotherapy regimens to treat many kinds of cancers. It is still the mainstay for the treatment of many neoplastic disorders including acute lymphoblastic leukemia.
Other uses
It has come into use as a treatment for some autoimmune diseases, including ankylosing spondylitis, Crohn's disease, psoriasis, psoriatic arthritis, rheumatoid arthritis, and scleroderma (see disease-modifying antirheumatic drugs). A parallel use with TNFα blockers such as infliximab or etanercept has been shown to markedly improve symptoms.[2]
Although not indicated for this use, methotrexate is also sometimes used (generally in combination with misoprostol) to terminate early pregnancies, particularly ectopic pregnancies. In the case of early missed miscarriage (particularly a blighted ovum), in which fetal demise has occurred but the body has not expelled the fetus, methotrexate may be used to help the body begin the miscarriage process.
It is also sometimes used to treat a rare condition called Behçet's disease where it is taken weekly, along with folic acid daily. In the case of immune disorders, such as Behcet's disease and rheumatoid disorders, the clinical goal of the low dose methotrexate regimen is to inhibit AICAR transformylase, which leads to increased AICA ribose (AICAR transformylase's substrate). The AICA ribose inhibits adenosine deaminase, resulting in a build-up of extracellular adenosine. Extracellular adenosine inhibits the expression of IL-2 receptors on circulating T-lymphocytes, causing a suppression of the immune system, and thus ameliorating the effects of the immune disorder.
Pharmacokinetics
Methotrexate is a weak dicarboxylic acid with pKa 4.8 and 5.5, and thus it is mostly ionized at physiologic pH. Oral absorption is saturatable and thus dose-dependent, with doses less than 40mg/M2 having 42% bioavailability and doses greater than 40mg/M2 only 18%. Mean oral bioavailability is 33% (13-76% range), and there is no clear benefit to subdividing an oral dose. Mean intramuscular bioavailability is 76%.
Methotrexate is metabolized by intestinal bacteria to the inactive metabolite 4-amino-4-deoxy-N-methylpteroic acid (DAMPA) and accounts for less than 5% loss of the oral dose.
Factors that decrease absorption include food, oral non-absorbable antibiotics (e.g. vancomycin, neomycin, and bacitracin), and more rapid transit through the Gastrointestinal (GI) tract such as diarrhea, while slower transit time in the GI tract from constipation will increase absorption.
Administration
It can be taken orally or administered by injection (subcutaneous, intramuscular, intravenous or intrathecal). Although daily preparations are occasionally used, most patients take weekly doses, which decreases the risk of certain side-effects.
Adverse effects
Possible side effects can include anemia, neutropenia, increased risk of bruising, nausea and vomiting, dermatitis and diarrhea. A small percentage of patients develop hepatitis, and there is an increased risk of pulmonary fibrosis.
The higher doses of methotrexate often used in cancer chemotherapy can cause toxic effects to the rapidly-dividing cells of bone marrow and gastrointestinal mucosa. The resulting myelosuppression and mucositis are often prevented (termed Leucovorin "rescue"- as this is the folic acid based drug used)
Methotrexate is a highly teratogenic drug and categorized in Pregnancy Category X by the FDA. Women must not take the drug during pregnancy, if there is a risk of becoming pregnant, or if they are breastfeeding. Men who are trying to get their partner pregnant must also not take the drug. To engage in any of these activities (after discontinuing the drug), women must wait until the end of a full ovulation cycle and men must wait three months.
There is a risk of a severe adverse reaction if penicillin is prescribed alongside methotrexate. There have also been some reports of central nervous system reactions to methotrexate especially when given via the intrathecal route which include myelopathies and leucoencephalopathies.
There have been reports of exacerbation of depressive illness with methotrexate.
References
- ↑ Johnston A, Gudjonsson JE, Sigmundsdottir H, Ludviksson BR, Valdimarsson H; (2005). "The anti-inflammatory action of methotrexate is not mediated by lymphocyte apoptosis, but by the suppression of activation and adhesion molecules". Clin Immunol. 114 (Feb.): 154–163. doi:. PMID 15639649.
- ↑ Klareskog L, van der Heijde D, de Jager JP, Gough A, Kalden J, Malaise M, Martin Mola E, Pavelka K, Sany J, Settas L, Wajdula J, Pedersen R, Fatenejad S, Sanda M (2004). "Therapeutic effect of the combination of etanercept and methotrexate compared with each treatment alone in patients with rheumatoid arthritis: double-blind randomised controlled trial". Lancet 363 (9410): 675–81. doi:. PMID 15001324.
External links
- Chembank entry on methotrexate
- Methotrexate general article from NIH
- Methotrexate Injection MedlinePlus article from NIH
- High Dose Methorexate as a potential treatment for Glioblastoma
- Patient Education - Methotrexate from American College of Rheumatology
- Methotrexate-resistant mutants of human dihydrofolate reductase for use as a selection marker in gene therapyas seen on Flintbox
|
||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||