Huntington's disease
| Huntington's disease Classification and external resources |
|
 |
|
|---|---|
| George Huntington's 1872 paper described the disorder. | |
| ICD-10 | G10., F02.2 |
| ICD-9 | 333.4, 294.1 |
| OMIM | 143100 |
| DiseasesDB | 6060 |
| MeSH | D006816 |
Huntington's disease, also called Huntington's chorea, chorea major, or HD, is a genetic neurological disorder[1] characterized after onset by uncoordinated, jerky body movements and a decline in some mental abilities. These characteristics vary per individual, physical ones less so, but the differing decline in mental abilities can lead to a number of potential behavioral problems. The disorder itself isn't fatal, but as symptoms progress, complications reducing life expectancy increase.[2]
Although recent knowledge of HD has increased greatly, its exact mechanism is unknown, so individual symptoms are managed with a range of medications and supportive services.[3] Globally, up to 7 people in 100,000 have the disorder, although there are localized regions with a higher incidence.[4] Onset of physical symptoms occurs gradually and can begin at any age, although it is statistically most common in a person's mid-forties (with a 30 year spread). If onset is before age twenty, the condition is classified as juvenile HD.[5]
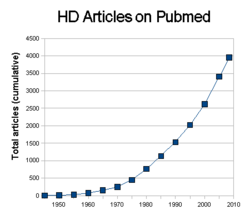
The disorder is named after George Huntington, an American physician who published a remarkably accurate description in 1872.[6] In 1983 a marker for the altered DNA causing the disease was found,[7] followed a decade later by discovery of a single, causal, gene.[8] As it was caused by a single gene, an accurate genetic test for HD was developed; this was one of the first inherited genetic disorders for which such a test was possible. Due to the availability of this test, and similar characteristics with other neurological disorders, the amount of HD research has increased greatly in recent years.[9]
Contents |
Classification
Huntington's disease is one of several trinucleotide repeat disorders, caused by the length of a repeated section of a gene exceeding the normal range. The huntingtin gene (HTT) normally provides the information to produce Huntingtin protein, but when affected, produces mutant Huntingtin (mHTT) instead.[10]
Signs and symptoms
Physical symptoms are usually the first to cause problems and to be noticed, but at this point they are usually accompanied by unrecognized cognitive and psychiatric ones. Almost everyone with Huntington's disease eventually exhibits all physical symptoms, but cognitive and psychiatric symptoms can vary significantly between individuals.[2]
Physical
The most characteristic symptoms are jerky, random, and uncontrollable movements called chorea. In a few cases, very slow movement and stiffness (called bradykinesia and dystonia) occur instead, and often become more prominent than the chorea as the disorder progresses. Abnormal movements are initially exhibited as general lack of coordination, an unsteady gait and slurring of speech, but, as the disease progresses, any function that requires muscle control is affected, causing physical instability, abnormal facial expression, and difficulties chewing and swallowing. Eating difficulties commonly cause weight loss and may lead to malnutrition.[11][12] Associated symptoms involve sleep cycle disturbances, including insomnia and Rapid eye movement sleep alterations.[13][14] Juvenile HD generally progresses faster, is more likely to exhibit rigidity and bradykinesia, instead of chorea, and commonly includes seizures.[2]
Cognitive
Select cognitive abilities are impaired progressively. Specially affected are executive functions which include planning, cognitive flexibility, abstract thinking, rule acquisition, initiating appropriate actions and inhibiting inappropriate actions.[15] Psychomotor function, controlling muscles, perception and spatial skills, is also affected.[15] As the disease progresses, memory deficits tend to appear. Memory impairments reported range from short-term memory deficits to long-term memory difficulties, including deficits in episodic (Memory of one's life), procedural (Memory of the body of how to perform an activity) and working memory.[15]
Psychiatric
These symptoms vary far more than cognitive and physical ones, and may include anxiety, depression, a reduced display of emotions (blunted affect), egocentrism, aggression, and compulsive behavior, which can cause, or worsen addictions, including alcoholism and gambling, or hypersexuality.[16][17] Difficulties in recognizing emotions, with particularly severe problems regarding recognition of expressions of disgust have also been repeatedly described.[15][18]
Genetics
- See also: Trinucleotide repeat disorders
The Huntingtin gene (HTT) is located on the short arm of chromosome 4 (4p16.3). HTT contains a sequence of three DNA bases—cytosine-adenine-guanine (CAG)—repeated multiple times (i.e. ...CAGCAGCAG...) on its 5' end, known as a trinucleotide repeat. CAG is the genetic code for the amino acid glutamine, so a series of them results in the production of a chain of glutamine known as polyglutamine or polyQ, and the repeated part of the gene, the PolyQ region.[19]
| Repeat count | Classification | Disease status |
|---|---|---|
| <27 | Normal | Unaffected |
| 27–35 | Intermediate | Unaffected |
| 36–39 | Reduced Penetrance | +/- Affected |
| >39 | Full Penetrance | Affected |
A polyQ region containing fewer than 36 glutamines results in production of the cytoplasmic protein called huntingtin (Htt). Generally, people have less than 27 repeated glutamines, however, a sequence of 36 or more glutamines, results in the production of form of Htt which has different characteristics. This altered form, called mutant Htt or more commonly mHtt, increases the rate of neuronal decay in certain types of neurons, affecting regions of the brain with a higher proportion or dependency on them. Generally, the number of CAG repeats is related to how much this process is affected, and correlates with age at onset and the rate of progression of symptoms.[10] For example, 36–39 repeats result in much later onset and slower progression of symptoms than the mean, such that some individuals may die of other causes before they even manifest symptoms of Huntington disease, this is termed "reduced penetrance".[20] With very large repeat counts, HD can occur under the age of 20 years, when it is then referred to as juvenile HD, akinetic-rigid, or Westphal variant HD and accounts for about 7 percent of HD carriers.[5]
Inheritance

Huntington's disease is inherited autosomal dominantly, meaning that an affected individual typically inherits a copy of the gene with an expanded trinucleotide repeat (the mutant allele) from an affected parent. In this type of inheritance pattern, each offspring of an affected individual has a 50% chance of inheriting the mutant allele and therefore being affected with the disorder (see figure). It is extremely rare for Huntington's disease to be caused by a de novo mutation,[21][22] however, the inheritance of HD is more complex due to potential dynamic mutations, where DNA replication does not produce an exact copy of the trinucleotide repeat. This can cause the number of repeats to change in successive generations, such that an unaffected parent with an "intermediate" number of repeats (28-35), or "reduced penetrance" (36-39), may pass on a copy of the gene with an increase in the number of repeats that produces fully penetrant HD.[23] These new mutations have occurred in less than 10 percent of people with HD, but explain the origins of the disorder.[24] Maternally inherited alleles are usually of a similar repeat length, whereas paternally inherited ones seem to have a higher chance of increasing in length.[25] Increases in the number of repeats (and hence earlier age of onset and severity of disease) in successive generations is known as genetic anticipation.
Homozygous individuals, who have two affected genes, are very rare except in large consanguineous families. While HD seemed to be the first disease for which homozygotes did not differ in clinical expression or course from typical heterozygotes,[26] more recent analysis suggests that homozygosity affects the phenotype and the rate of disease progression but does not alter the age of onset, suggesting that the mechanisms for these factors differ.[27]
Mechanism
- See also: Huntingtin protein
Like all proteins, Htt and mHtt are translated, perform or affect biological functions, and are then marked by ubiquitin to be degraded by proteasomes, but their exact roles are unknown. Research has focused on identifying the functioning of Htt, how mHtt differs or interferes with it, including its influence in programmed cell death, and the proteopathy of remnants of mHtt left after degradation.[1]
Function
Although the function of the Huntingtin protein is unclear, some hypotheses have been drawn from observations. In mouse models, Htt is essential for development and survival.[28] In "knockin" mice, the extended CAG repeat portion of the gene is all that is needed to cause disease.[29] The protein has no sequence homology with other proteins and is highly expressed in neurons and testes.[30] Experiments have shown Htt acts as a transcription factor in upregulating the expression of Brain Derived Neurotrophic Factor (BDNF), a protein which protects neurons and regulates the neurogenesis of new ones, whereas mHtt suppresses this transcription regulatory function of Huntingtin and hence underexpression of BDNF, which leads to progressive atrophy of select areas of the brain.[31][32][33][34]From immunohistochemistry, electron microscopy, subcellular fractionation studies of the molecule, it has been found that Huntingtin is primarily associated with vesicles and microtubules.[35][36].These indicate a functional role in cytoskeletal anchoring or transport of mitochondria. The Htt protein is involved in vesicle trafficking as it interacts with HIT1, a clathrin binding protein, to mediate endocytosis, the absorption of materials into a cell.[37][38] Initial studies show carriers of the expanded repeat may have better than average immune systems, with higher levels of Interleukin 6 and tumor suppressor protein p53.[39][40]
Degradation
In the first step of degradation, both Htt and mHtt are cleaved by caspase-3, which removes the protein's amino end (the N-terminal).[41] Caspase-2 then further breaks down the amino terminal fragment (which includes the CAG repeat) of Htt, but cannot process all of the mHtt protein.[42] In transgenic mice, the caspase-6 enzyme has been shown to be involved in cleaving the Htt protein, as mice made resistant to this enzyme did not suffer neurodegeneration.[43]The uncleaved pieces of mHtt, left in the cell, called N-fragments, and are able to affect genetic transcription.[44] Specifically, mHtt binds with TAFII130, a coactivator to CREB dependent transcription.[45] The mHtt protein also interacts with the transcription factor protein SP1, preventing it from binding to DNA.[46]
Neuronal intranuclear inclusions containing the huntingtin and ubiquitin proteins have been found in both humans and mice with HD,[47][48]. Such inclusions are most prevalent in cortical pyramidal neurons, less so in striatal medium-sized spiny neurons and almost entirely absent in most other regions.[47][49][50] These inclusions consist mainly of the amino terminal end of mHtt (CAG repeat), and are found in both the cytoplasm and nucleus of neurons,[51] however their presence does not correlate with cell death, and may even act as a protective mechanism to the cell.[52][53] Thus, mHtt acts in the nucleus but does not cause apoptosis through protein aggregation.[54]
Pathophysiology
HD causes astrogliosis[55] and loss of medium spiny neurons[56][57] Areas of the brain are affected according to their structure and the types of neurons they contain, reducing in size as they cumulatively lose cells. The areas affected are mainly in the striatum, but also the frontal and temporal cortices.[58] The striatum's subthalamic nuclei send control signals to the globus pallidus, which initiates and modulates motion. The weaker signals from subthalamic nuclei thus cause reduced initiation and modulation of movement, resulting in the characteristic movements of the disorder.[59]
Although studies are mainly focused on physiopathology of the brain, a few look at how Huntington's disease appears to affect other physiological functions. One study in humans highlighted a systemic, early hypermetabolic state and a lower level of branched chain amino acids in the plasma as the disease progresses, which is hypothesised to be caused by the brain's use of these.[60]
Diagnosis
- Further information: Genetic testing
A physical and/or psychological examination can determine whether initial symptoms are evident. Abnormal movements are often the symptoms that cause initial impetus to seek medical consultation and lead to diagnosis; however, the disease may begin with cognitive or pyschiatric symptoms, which are not always recognized except in hindsight, or if they develop further. Pre-symptomatic testing is possible using a blood test which counts the numbers of CAG repeats in each of the HTT alleles,[61] although a positive result is not considered a diagnosis, since it may be obtained decades before onset of symptoms. A negative blood test means that the individual does not carry the expanded copy of the gene. A full pathological diagnosis can only be established by a neurological examination's findings and/or demonstration of cell loss in the areas affected by HD, supported by a cranial CT or MRI scan findings.[62]
A pre-symptomatic test is a life-changing event and a very personal decision. The personal ramifications to an at-risk individual and lack of cure for the disease necessitate several counseling sessions to ensure that they are prepared for either result before it is given.[63] Unless a person under eighteen years of age is considered to be Gillick competent, testing is not offered by many institutions unless they show significant symptoms or are sexually active.[64] Many organisations and lay groups strongly endorse these restrictions in their testing protocol.
Embryonic screening is also possible, giving affected or at-risk individuals the option of ensuring their children will not inherit the disease. It is possible for women who would consider abortion of an affected fetus to test an embryo in the womb (prenatal diagnosis). Other techniques, such as preimplantation genetic diagnosis in the setting of in vitro fertilisation, can be used to ensure that the newborn is unaffected.[65]
Management
Some symptoms can be reduced or alleviated by medicine, rehabilitation methods, nutrition management and general care methods.
Pharmacological
Treatments for cognitive and psychological symptoms include antidepressants and sedatives, and low doses of antipsychotics.[66] There is limited evidence for specific treatments aimed at controlling the chorea and other movement abnormalities, although tetrabenazine has been shown to reduce the severity of the chorea;[67] it was approved in 2008 specifically for this indication.[3]
Rehabilitation
Although there are relatively few studies of rehabilitation for HD, its general effectiveness when conducted by a team of specialists has been clearly demonstrated in other pathologies such as stroke,[68] or head trauma.[69] As for any patient with neurologic deficits, a multidisciplinary approach is key to limiting and overcoming disability.[70] There is partial evidence for the usefulness of physical therapy and speech therapy but most studies on the subject have been of low quality and further evidence is needed for health authorities to endorse them.[71]
Nutrition
Nutrition is an important part of treatment; most people in the later stages of the disease require two to three times more calories than average to maintain body weight.[72] Thickening agent can be added to drinks as swallowing becomes more difficult, as thicker fluids are easier and safer to swallow. The option of using a percutaneous endoscopic gastrostomy (i.e., a feeding tube into the stomach) is available when eating becomes too hazardous or uncomfortable. A "stomach PEG" greatly reduces the chances of aspiration of food, which can lead to aspiration pneumonia,and also increases the amount of nutrients and calories that can be ingested, aiding the body's natural defenses.[73]
Prognosis
The age of onset decreases, and the rate of progression of symptoms increase, with the number of CAG repeats. Individuals with greater than approximately 60 CAG repeats often develop juvenile Huntington's disease.[74][75] There is a variation in age of onset for any given CAG repeat length, particularly within the intermediate range (40–50 CAGs). For example, a repeat length of 40 CAGs leads to an onset ranging from 40 to 70 years of age in one study. This variation means that, although algorithms have been proposed for predicting the age of onset, in practice, it can not be predicted confidently.[76][77]
The life expectancy is around 15 to 20 years following the onset of characteristic manifestations of the disorder.[78] Mortality is not caused by Huntington’s disease directly, but by associated complications; these include pneumonia (which causes one third of fatalities), heart failure (although heart disease, cerebrovascular disease and atherosclerosis show no increase), choking, malnutrition and physical injury.[79] Suicide is an associated risk, with increased suicide rates of up to 7.3 percent, and attempted suicides of up to 27 percent.[80][81][2]
Epidemiology
As HD is autosomal dominant, and does not usually affect reproduction, areas of increased prevalence occur according to historical migration of carriers, some of which can be traced back thousands of years using genetic haplotypes.[82] Since the discovery of a genetic test that can also be used pre-symptomatically, estimates of the incidence of the disorder are likely to increase. Without the test, only individuals displaying physical symptoms or neurologically examined cases were diagnosed, excluding any who died of other causes before symptoms or diagnosis occurred. These cases can now be included in statistics as the test becomes more widely available and estimates have shown the incidence of HD could be two to three times higher when these results are included.[83]
The prevalence varies greatly according to geographical location, both by ethnicity and local migration; The highest occurrence is in peoples of Western Europe descent, averaging between 3 to 7 per 100,000 people, but is relatively lower in the rest of the world, e.g. 1 per 1,000,000 of Asian and African descent.[4] Some localised areas have a much higher prevalence than their geographical average, for example the isolated populations of the Lake Maracaibo region of Venezuela (where the marker for the gene was discovered), have an extremely high prevalence of up to 700 per 100,000,[84] leading to the conclusion that one of their initial founders must have been a carrier of the gene. This is known as the local founder effect.[7]
History
In the first part of the twentieth century and earlier, many people with HD were misdiagnosed as suffering from alcoholism or manic depression. Previously mortality due to starvation or dehydration was a major risk.
- Middle Ages: People with the condition were probably persecuted as being witches or as being possessed by spirits, and were shunned, exiled or worse. Some speculate that the "witches" in the Salem Witch Trials in 1692 had HD.[85][86]
- 1860: One of the early medical descriptions of HD was made in 1860 by a Norwegian district physician, Johan Christian Lund. He noted that in Setesdalen, a remote and rather secluded area, there was a high prevalence of dementia associated with a pattern of jerking movement disorders that tended to run in families. This is the reason for the disease being commonly referred to as Setesdalsrykkja (Setesdalen=the location, rykkja=jerking movements) in Norwegian.[87]
- 1872: George Huntington was the third generation of a family medical practice in Long Island. With their combined experience of several generations of a family with the same symptoms, he realised their conditions were linked and set about describing it. A year after leaving medical school, in 1872, he presented his accurate definition of the disease to a medical society in Middleport, Ohio.[6][88]
- c. 1902: Smith Ely Jelliffe (1866–1945) began studying the history of HD sufferers in New England and published several articles over the next few decades..[89]
- 1932: P. R. Vessie expanded Jelliffe and Tilney's work, tracing about a thousand people with HD back to two brothers and their families who left Bures in Suffolk, England bound for Boston, MA in 1630.[90]
- 1979: The US-Venezuela Huntington's Disease Collaborative Research Project began an extensive study which gave the basis for the gene to be discovered. This was conducted in the small, isolated Venezuelan fishing villages of Barranquitas and Lagunetas, where families have a high presence of the disease.[91]
- 1983: James Gusella, David Housman, P. Michael Conneally, Nancy Wexler, and their colleagues find the general location of the gene, using DNA marking methods for the first time—an important first step toward the Human Genome Project.[7]
- 1992: Anita Harding, et al. find that trinucleotide repeats affect disease severity[92]
- 1993: The Huntington's Disease Collaborative Research Group isolates the precise gene at 4p16.3.[93]
- 1996: A transgenic mouse (the R6 line) was created that could be made to exhibit HD, greatly advancing how much experimentation can be achieved.[94][95]
- 1997: DiFiglia M, Sapp E, Chase KO, et al., discover that mHtt fragments misfold, leading to the formation of nuclear inclusions.[47]
- The full record of research is extensive.[2]
Society and culture
- See also: List of Huntington's disease media depictions
As public awareness has increased, HD has been depicted increasingly in numerous books, films and TV series. Early works were Arlo Guthrie's 1969 film Alice's Restaurant[98] and Jacqueline Susann's 1966 American novel Valley of the Dolls; more recent references were made in ER,[99] Private Practice,[100] Everwood,[101] All Saints,[102] and House.[103] Steven T. Seagle's 2004 graphic novel "It's a Bird" discusses Huntington's disease and the effects on his family.[104] Many support organizations hold an annual HD awareness event, and some have been endorsed by their respective governments, for example, June 6 is designated "National Huntington's Disease Awareness Day" by the USA senate, and the UK HDA holds an awareness campaign in the third week of June.[105]
Social impact
The development of an accurate diagnostic test for Huntington's disease has caused social, legal, and ethical concerns over access and use of a person's results[106][107] There have been guidelines created by the IHA and WFN for the use of genetic testing in HD, but many governments and institutions, although agreeing not to genetically discriminate against an individual, have not reached a consensus.[108] As for the individual, the decision to undergo a presymptomatic test, thereby learning whether they will inherit the disorder, is a complicated one. Genetic counseling is designed to provide information, advice and support for a person to decide, and then throughout all stages of the testing process, if so chosen.[63]
One of the key issues is the level of anxiety that an individual experiences about "not knowing" whether they will some day develop HD, compared to the psychological impact that might occur if the test indicates that one will eventually succumb to the disease. In contrast individuals found to have inherited the normal allele may experience Survivor guilt with regard to their affected family members.[109] Some individuals choose not to undergo testing due to concerns about prejudice in areas such as insurability, employment and financial matters. An important ethical consideration is the testing of asymptomatic minors. As with other genetic conditions with later onset for which no treatment is available, it is ethically questionable to perform presymptomatic testing for a child or individual who has not made a mature, informed decision for themselves.[110] Such information may cause psychological harm, jeopardize that individual's employment or ability to obtain health and life insurance. For this reason, presymptomatic testing in minors is a controversial area, with arguments in favor of permitting testing only when the individual is mature enough to provide assent versus minimizing medical paternalism in favor of parental preferences.[111][112][113][64] The balance of opinion would change drastically if an effective treatment was discovered.
Genetic testing may infer information about relatives who do not want it. Testing a descendant of a undiagnosed parent has implications to other family members, since a positive result automatically reveals the parent as carrying the affected gene, and siblings (and especially identical twins) as being 'at risk' of also inheriting it.[114] This emphasizes the importance of disclosure, as individuals have to decide when and how to reveal the information to their children and other family members. For those at risk, or known to carry a mutant allele, there can be the consideration of prenatal genetic testing and preimplantation genetic diagnosis in order to ensure that the disorder is not passed on.[115]
Huntington's disease has tested society's ethics in various ways. HD was one of the targets of the eugenics movement, in which American scientist Charles Davenport proposed in 1910 that compulsory sterilization and immigration control be used for people with certain diseases, including HD.[116] Since the development of genetic testing for HD, financial institutions and businesses are also faced with the question of whether to use results when assessing an individual, e.g. for life insurance or employment. Some countries' organizations have already agreed not to use this information.[117] Recent passage of the Genetic Information Nondiscrimination Act (GINA) in the United States prevents health insurance companies from denying coverage or charging higher premiums for individuals with predisposition to genetic disease.
Organizations
- 1967: Woody Guthrie's wife, Marjorie, helped found the Committee to Combat Huntington's Disease, after his death from HD complications. This eventually became the Huntington's Disease Society of America.[118] Since then, lay organizations have been formed in many countries around the world.
- 1968: After experiencing HD in his wife's family Dr. Milton Wexler was inspired to start the Hereditary Disease Foundation (HDF). Professor Nancy S. Wexler, Dr. Wexler's daughter, was in the research team in Venezuela and is now president of the HDF.
- 1974: The first international meeting took place when the founders of the Canadian HD Society (Ralph Walker) and of the British HD Society (Mauveen Jones) attended the annual meeting of the American HD Society.
- 1977: Second meeting organized by the Dutch Huntington Society the "Vereniging van Huntington", representatives of six countries were present.
- 1979: International Huntington Association (IHA) formed during international meeting in Oxford, England organized by HDA of England.
- 1981–2001: Biennial meetings held by IHA which became the World Congress on HD.
- 2003: The first World Congress on Huntington's Disease was held in Toronto.[119] This is a biennial meeting for associations and researchers to share ideas and research, which is held on odd-number years. The Euro-HD Network[120] was started as part of the Huntington Project,[121] funded by the High-Q Foundation.[122]
Research directions
Appropriate animal models are critical for understanding the fundamental mechanisms causing the disease and for supporting the early stages of drug development. Neurochemically induced mice or monkeys were first available,[123][124] but they did not mimic the progressive features of the disease. After the HD gene was discovered, transgenic animals exhibiting HD were generated by inserting a CAG repeat expansion into their genome, these were of mice (strain R6/2),[125][126]), Drosophila fruit flies,[127] and more recently monkeys.[128] Expression without insertion of a DNA repeat in nematode worms also produced a valuable model.[129]
Intrabody therapy
Genetically engineered intracellular antibody fragments called intrabodies have shown therapeutic results, by inhibiting mHtt aggregation, in drosophila models. This was achieved using an intrabody called C4 sFv, a single chain variable fragment which binds to the end of mHtt within a cell.[130][131] This therapy prevented larval and pupal mortality (without therapy 77% died) and delayed neurodegeneration in the adult, significantly increasing their lifespan.[132] Intrabody therapy shows promise as a tool for drug discovery, and as a potential therapy for HD and other neurodegenerative disorders caused by protein mis-folding or abnormal protein interactions.[133][134]
Gene silencing
As HD has been conclusively linked to a single gene, gene silencing is potentially possible. Researchers have investigated using gene knockdown of mHTT as a potential treatment. Using a mouse model, siRNA therapy achieved a 60 percent reduction in expression of the mHTT and progression of the disease was stalled.[135] However, this study used the human form of the mHTT protein in the mouse, and was therefore only able to directly target the mHTT, leaving endogenous, wild-type mouse Htt gene expression unaffected. From a practical standpoint, it would be difficult in humans to use siRNA to target the mutant form while leaving the normal copy unaffected. The precise function of HTT is unknown, but in mice, complete deletion of the Htt gene is lethal.[28] Thus, using RNA interference to treat HD could have unexpected effects unless knock-down of the normal HTT protein can be avoided. Other issues include problems delivering the siRNA to the appropriate target tissue, off-target effects of siRNA, and toxicity from shRNA over-expression.[136] Another study showed that mouse models already in late stages of the disease recovered motor function after expression of mHTT was stopped.[137]
Stem cell implants
Stem cell therapy is the replacement of damaged neurons by transplantation of stem cells ( or possibly neural stem cells - a type of somatic (adult) stem cell ) into affected regions of the brain. Hypothetically, embryonic stem cells can be differentiated into neuronal precursors in vitro, and transplanted into damaged areas of the brain to generate replacement neurons, if enough damaged neurons can be replaced and develop the correct synaptic connectivity, symptoms could be alleviated. This treatment would not prevent further neuronal damage, so it would have to be an ongoing treatment. Experiments have yielded some positive results in animal models, but remains highly speculative and has not been tested in clinical trials.[138]
Pharmacological
As of August 2008, several trials of various compounds are in development or ongoing,[139] a few at the point of testing on larger numbers of people, known as phase III of clinical trials. Substances that have shown promise in initial experiments include dopamine receptor blockers, select dopamine antagonists, such as tetrabenazine, creatine, CoQ10, the antibiotic Minocycline, antioxidant-containing foods and nutrients, and antidepressants, including selective serotonin reuptake inhibitors such as sertraline, fluoxetine, and paroxetine.[140][3]
References
- ↑ 1.0 1.1 Imarisio S, Carmichael J, Korolchuk V, et al (June 2008). "Huntington's disease: from pathology and genetics to potential therapies". Biochem. J. 412 (2): 191–209. doi:. PMID 18466116.
- ↑ 2.0 2.1 2.2 2.3 2.4 Gillian Bates, Peter Harper, and Lesley Jones (2002). Huntington's Disease - Third Edition. Oxford: Oxford University Press. ISBN 0-19-851060-8.
- ↑ 3.0 3.1 3.2 Bonelli RM, Wenning GK (2006). "Pharmacological management of Huntington's disease: An evidence-based review". Curr. Pharm. Des. 12 (21): 2701–20. doi:. PMID 16842168. http://www.bentham-direct.org/pages/content.php?CPD/2006/00000012/00000021/0010B.SGM.
- ↑ 4.0 4.1 NCBI OMIM. "Huntington's Disease". Retrieved on 2008-05-22.
- ↑ 5.0 5.1 Nance MA, Myers RH (2001). "Juvenile onset Huntington's disease--clinical and research perspectives". Ment Retard Dev Disabil Res Rev 7 (3): 153–7. doi:. PMID 11553930.
- ↑ 6.0 6.1 Huntington, G. (1872-04-13). "On Chorea". Medical and Surgical Reporter of Philadelphia 26 (15): 317–321. http://en.wikisource.org/wiki/On_Chorea.
- ↑ 7.0 7.1 7.2 Gusella JF, Wexler NS, Conneally PM, et al. (1983). "A polymorphic DNA marker genetically linked to Huntington's disease". Nature 306 (5940): 234–8. doi:. PMID 6316146.
- ↑ Macdonald, M (March 1993). "A novel gene containing a trinucleotide repeat that is expanded and unstable on Huntington's disease chromosomes. The Huntington's Disease Collaborative Research Group". Cell 72 (6): 971–83. doi:. PMID 8458085.
- ↑ Walker FO (January 2007). "Huntington's disease". Lancet 369 (9557): 218–28. doi:. PMID 17240289.
- ↑ 10.0 10.1 Kieburtz K, MacDonald M, Shih C, et al. (1994). "Trinucleotide repeat length and the progression of illness in Huntington's disease". J. Med. Genet. 31 (11): 872–4. PMID 7853373.
- ↑ Gaba AM, Zhang K, Marder K, Moskowitz CB, Werner P, Boozer CN (2005). "Energy balance in early-stage Huntington disease". Am. J. Clin. Nutr. 81 (6): 1335–41. PMID 15941884.
- ↑ "Booklet by the Huntington Society of Canada" (PDF). Caregiver's Handbook for Advanced-Stage Huntington Disease.. HD Society of Canada (2007-04-11). Retrieved on 2008-08-10.
- ↑ Morton AJ, Wood NI, Hastings MH, et al. (January 2005). "Disintegration of the sleep-wake cycle and circadian timing in Huntington's disease". J. Neurosci. 25 (1): 157–63. doi:. PMID 15634777. http://www.jneurosci.org/cgi/pmidlookup?view=long&pmid=15634777.
- ↑ Arnulf I, Nielsen J, Lohmann E, et al. (April 2008). "Rapid eye movement sleep disturbances in Huntington disease". Arch Neurol 65 (4): 482–488. doi:. PMID 18413470.
- ↑ 15.0 15.1 15.2 15.3 Montoya A, Price BH, Menear M, Lepage M (January 2006). "Brain imaging and cognitive dysfunctions in Huntington's disease" (PDF). J Psychiatry Neurosci 31 (1): 21–9. PMID 16496032. PMC: 1325063. http://www.cma.ca/multimedia/staticContent/HTML/N0/l2/jpn/vol-31/issue-1/pdf/pg21.pdf.
- ↑ Sandyk R (1992). "L-tryptophan in neuropsychiatric disorders: A review". Int. J. Neurosci. 67 (1-4): 127–44. PMID 1305630.
- ↑ van Duijn E, Kingma EM, van der Mast RC (2007). "Psychopathology in verified Huntington's disease gene carriers". J Neuropsychiatry Clin Neurosci 19 (4): 441–8. doi:. PMID 18070848.
- ↑ Johnson SA, Stout JC, Solomon AC, et al. (2007). "Beyond disgust: Impaired recognition of negative emotions prior to diagnosis in Huntington's disease". Brain 130 (Pt 7): 1732–44. doi:. PMID 17584778.
- ↑ Katsuno M, Banno H, Suzuki K, et al. (May 2008). "Molecular genetics and biomarkers of polyglutamine diseases". Curr. Mol. Med. 8 (3): 221–34. doi:. PMID 18473821. http://www.bentham-direct.org/pages/content.php?CMM/2008/00000008/00000003/0005M.SGM.
- ↑ Chong SS, Almqvist E, Telenius H, et al. (February 1997). "Contribution of DNA sequence and CAG size to mutation frequencies of intermediate alleles for Huntington disease: Evidence from single sperm analyses" (PDF). Hum. Mol. Genet. 6 (2): 301–9. doi:. PMID 9063751. http://hmg.oxfordjournals.org/cgi/reprint/6/2/301.
- ↑ Myers et al. (1993). "De novo expansion of a (CAG)n repeat in sporadic Huntington's disease". Nature Genetics 5: 168–173. doi:. http://www.nature.com/ng/journal/v5/n2/abs/ng1093-168.html.
- ↑ Sánchez A, Milà M, Castellví-Bel S, Rosich M, Jiménez D, Badenas C, Estivill X. (1997). "Maternal transmission in sporadic Huntington's disease". J Neurol Neurosurg Psychiatry 62 (5): 535–537. PMID 9153618.
- ↑ Chong SS, Almqvist E, Telenius H, et al (February 1997). "Contribution of DNA sequence and CAG size to mutation frequencies of intermediate alleles for Huntington disease: evidence from single sperm analyses". Hum. Mol. Genet. 6 (2): 301–9. doi:. PMID 9063751. http://hmg.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=9063751.
- ↑ García-Planells J, Burguera JA, Solís P, et al. (May 2005). "Ancient origin of the CAG expansion causing Huntington disease in a Spanish population". Hum. Mutat. 25 (5): 453–9. doi:. PMID 15832309.
- ↑ RM Ridley, CD Frith, TJ Crow and PM Conneally (1988). "Anticipation in Huntington's disease is inherited through the male line but may originate in the female". Journal of Medical Genetics 25: 589–595. PMID 2972838. http://jmg.bmjjournals.com/cgi/content/abstract/25/9/589.
- ↑ Wexler NS, Young AB, Tanzi RE, et al. (1987). "Homozygotes for Huntington's disease". Nature 326 (6109): 194–197. doi:. PMID 2881213.
- ↑ Squitieri F, Gellera C, Cannella M, Mariotti C, Cislaghi G, Rubinsztein DC, Almqvist EW, Turner D, Bachoud-Lévi AC, Simpson SA, Delatycki M, Maglione V, Hayden MR, Donato SD (2003). "Homozygosity for CAG mutation in Huntington disease is associated with a more severe clinical course". Brain 126 (4): 946–955. doi:. PMID 12615650. http://brain.oxfordjournals.org/cgi/content/full/126/4/946.
- ↑ 28.0 28.1 Nasir J, Floresco S, et al (1995). "Targeted disruption of the Huntington's disease gene results in embryonic lethality and behavioral and morphological changes in heterozygotes". Cell 81: 811–823. doi:. PMID 7774020.
- ↑ Murphy KP, Carter RJ, Lione LA, et al. (2000). "Abnormal synaptic plasticity and impaired spatial cognition in mice transgenic for exon 1 of the human Huntington's disease mutation". J. Neurosci. 20 (13): 5115–23. PMID 10864968.
- ↑ Cattaneo E, Zuccato C, Tartari M (December 2005). "Normal huntingtin function: an alternative approach to Huntington's disease". Nature Reviews Neuroscience 6: 919–930. doi:.
- ↑ Zuccato C, Ciammola A, Rigamonti D, Leavitt BR, Goffredo D, et al (2001-07-20). "Loss of huntingtin-mediated BDNF gene transcription in Huntington's disease". Science 293 (5529): 445–6. doi:. PMID 11463904.
- ↑ Canals JM, Pineda JR, Torres-Peraza JF, et al. (2004). "Brain-derived neurotrophic factor regulates the onset and severity of motor dysfunction associated with enkephalinergic neuronal degeneration in Huntington's disease". J. Neurosci. 24 (35): 7727–39. doi:. PMID 15342740.
- ↑ Sawa A, Nagata E, Sutcliffe S, et al. (2005). "Huntingtin is cleaved by caspases in the cytoplasm and translocated to the nucleus via perinuclear sites in Huntington's disease patient lymphoblasts". Neurobiol. Dis. 20 (2): 267–74. doi:. PMID 15890517.
- ↑ Strand AD, Baquet ZC, Aragaki AK, et al. (October 2007). "Expression profiling of Huntington's disease models suggests that brain-derived neurotrophic factor depletion plays a major role in striatal degeneration". J. Neurosci. 27 (43): 11758–68. doi:. PMID 17959817. http://www.jneurosci.org/cgi/content/full/27/43/11758.
- ↑ Hoffner G, Kahlem P, Djian P (March 2002). "Perinuclear localization of huntingtin as a consequence of its binding to microtubules through an interaction with β-tubulin: relevance to Huntington's disease". J Cell Sci 115: 941–948. PMID 11870213. http://jcs.biologists.org/cgi/pmidlookup?view=long&pmid=11870213.
- ↑ DiFiglia M, et al. (1995). "Huntingtin is a cytoplasmic protein associated with vesicles in human and rat brain neurons". Neuron 14: 1075–1081. doi:.
- ↑ Velier J, Kim M, Schwarz C, et al. (1998). "Wild-type and mutant huntingtins function in vesicle trafficking in the secretory and endocytic pathways". Exp. Neurol. 152 (1): 34–40. doi:. PMID 9682010.
- ↑ Waelter S, Scherzinger E, Hasenbank R, et al. (2001). "The huntingtin interacting protein HIP1 is a clathrin and alpha-adaptin-binding protein involved in receptor-mediated endocytosis". Hum. Mol. Genet. 10 (17): 1807–17. doi:. PMID 11532990.
- ↑ Björkqvist M, Wild EJ, Thiele J, et al. (August 2008). "A novel pathogenic pathway of immune activation detectable before clinical onset in Huntington's disease". J. Exp. Med. 205 (8): 1869–77. doi:. PMID 18625748. http://www.jem.org/cgi/pmidlookup?view=long&pmid=18625748.
- ↑ Eskenazi BR,Wilson-Rich NS, Starks PT (2007). "A Darwinian approach to Huntington’s disease: Subtle health benefits of a neurological disorder". Med. Hypotheses 69 (6): 1183–9. doi:. PMID 17689877.
- ↑ Kim YJ, Yi Y, Sapp E, et al. (2001). "Caspase 3-cleaved N-terminal fragments of wild-type and mutant huntingtin are present in normal and Huntington's disease brains, associate with membranes, and undergo calpain-dependent proteolysis". Proc. Natl. Acad. Sci. U.S.A. 98 (22): 12784–9. doi:. PMID 11675509.
- ↑ Hermel E, Gafni J, Propp SS, et al. (2004). "Specific caspase interactions and amplification are involved in selective neuronal vulnerability in Huntington's disease". Cell Death Differ. 11 (4): 424–38. doi:. PMID 14713958.
- ↑ Graham RK, Deng Y, Slow EJ, et al. (2006). "Cleavage at the caspase-6 site is required for neuronal dysfunction and degeneration due to mutant huntingtin". Cell 125 (6): 1179–91. doi:. PMID 16777606.
- ↑ Freiman RN, Tjian R (2002). "Neurodegeneration. A glutamine-rich trail leads to transcription factors". Science 296 (5576): 2149–50. doi:. PMID 12077389.
- ↑ Bae BI, Xu H, Igarashi S, et al. (2005). "p53 mediates cellular dysfunction and behavioral abnormalities in Huntington's disease". Neuron 47 (1): 29–41. doi:. PMID 15996546.
- ↑ Dunah AW, Jeong H, Griffin A, et al. (2002). "Sp1 and TAFII130 transcriptional activity disrupted in early Huntington's disease". Science 296 (5576): 2238–43. doi:. PMID 11988536.
- ↑ 47.0 47.1 47.2 DiFiglia M, Sapp E, Chase KO, et al. (1997). "Aggregation of huntingtin in neuronal intranuclear inclusions and dystrophic neurites in brain". Science 277 (5334): 1990–3. doi:. PMID 9302293.
- ↑ Davies SW, Turmaine M, Cozens BA, et al. (1997). "Formation of neuronal intranuclear inclusions underlies the neurological dysfunction in mice transgenic for the HD mutation". Cell 90 (3): 537–48. doi:. PMID 9267033.
- ↑ Gutekunst CA, Li SH, Yi H, et al. (1999). "Nuclear and neuropil aggregates in Huntington's disease: Relationship to neuropathology". J. Neurosci. 19 (7): 2522–34. PMID 10087066.
- ↑ Sieradzan KA, Mechan AO, Jones L, et al. (1999). "Huntington's disease intranuclear inclusions contain truncated, ubiquitinated huntingtin protein". Exp. Neurol. 156 (1): 92–9. doi:. PMID 10192780.
- ↑ Cooper JK, Schilling G, Peters MF, et al. (1998). "Truncated N-terminal fragments of huntingtin with expanded glutamine repeats form nuclear and cytoplasmic aggregates in cell culture". Hum. Mol. Genet. 7 (5): 783–90. doi:. PMID 9536081.
- ↑ Fusco FR, Chen Q, Lamoreaux WJ, et al. (1999). "Cellular localization of huntingtin in striatal and cortical neurons in rats: Lack of correlation with neuronal vulnerability in Huntington's disease". J. Neurosci. 19 (4): 1189–202. PMID 9952397.
- ↑ Arrasate M, Mitra S, Schweitzer ES, Segal MR, Finkbeiner S (2004). "Inclusion body formation reduces levels of mutant Huntingtin and the risk of neuronal death". Nature 431: 805–810. PMID 15483602.
- ↑ Saudou F, Finkbeiner S, Devys D, Greenberg ME (1998). "Huntingtin acts in the nucleus to induce apoptosis but death does not correlate with the formation of intranuclear inclusions". Cell 95 (1): 55–66. doi:. PMID 9778247.
- ↑ Lobsiger CS, Cleveland DW (November 2007). "Glial cells as intrinsic components of non-cell-autonomous neurodegenerative disease". Nat. Neurosci. 10 (11): 1355–60. doi:. PMID 17965655.
- ↑ Purves D, Augustine GA, Fitzpatrick D, Hall W, LaMantia A-S, McNamara JO, Williams SM. "Modulation of Movement by the Basal Ganglia - Circuits within the Basal Ganglia System". in Dale Purves. Neuroscience (2nd edition ed.). Sunderland, MA: Sinauer Associates. ISBN 0-87893-742-0. http://www.ncbi.nlm.nih.gov/books/bv.fcgi?highlight=Huntington's%20disease&rid=neurosci.section.1251.
- ↑ Estrada Sánchez AM, Mejía-Toiber J, Massieu L (April 2008). "Excitotoxic neuronal death and the pathogenesis of Huntington's disease". Arch. Med. Res. 39 (3): 265–76. doi:. PMID 18279698. http://linkinghub.elsevier.com/retrieve/pii/S0188-4409(07)00412-2.
- ↑ Purves D, Augustine GA, Fitzpatrick D, Hall W, LaMantia A-S, McNamara JO, Williams SM. "Modulation of Movement by the Basal Ganglia - Box A. Huntington's Disease". in Dale Purves. Neuroscience (2nd edition ed.). Sunderland, MA: Sinauer Associates. ISBN 0-87893-742-0. http://www.ncbi.nlm.nih.gov/books/bv.fcgi?highlight=Huntington's%20disease&rid=neurosci.box.1240.
- ↑ Crossman AR (May 2000). "Functional anatomy of movement disorders" (PDF). J. Anat. 196 ( Pt 4): 519–25. doi:. PMID 10923984. PMC: 1468094. http://www3.interscience.wiley.com/cgi-bin/fulltext/119004203/PDFSTART.
- ↑ Mochel F, Charles P, Seguin F, Barritault J, Coussieu C, Perin L, Le Bouc Y, Gervais C, Carcelain G, Vassault A, Feingold J, Rabier D, Durr A (2007). "Early energy deficit in Huntington disease: Identification of a plasma biomarker traceable during disease progression". PLoS ONE 2 (7): e647. doi:. PMID 17653274.
- ↑ Myers RH (April 2004). "Huntington's disease genetics". NeuroRx 1 (2): 255–62. doi:. PMID 15717026.
- ↑ Stober T, Wussow W, Schimrigk K (1984). "Bicaudate diameter--the most specific and simple CT parameter in the diagnosis of Huntington's disease". Neuroradiology 26 (1): 25–8. doi:. PMID 6234475.
- ↑ 63.0 63.1 Burson CM, Markey KR (September 2001). "Genetic counseling issues in predictive genetic testing for familial adult-onset neurologic diseases". Semin Pediatr Neurol 8 (3): 177–86. doi:. PMID 11575847.
- ↑ 64.0 64.1 Borry P, Goffin T, Nys H, Dierickx K (August 2008). "Predictive genetic testing in minors for adult-onset genetic diseases". Mt. Sinai J. Med. 75 (3): 287–296. doi:. PMID 18704981.
- ↑ Kuliev A, Verlinsky Y (April 2005). "Preimplantation diagnosis: A realistic option for assisted reproduction and genetic practice". Curr. Opin. Obstet. Gynecol. 17 (2): 179–83. PMID 15758612. http://meta.wkhealth.com/pt/pt-core/template-journal/lwwgateway/media/landingpage.htm?issn=1040-872X&volume=17&issue=2&spage=179.
- ↑ "UK NHS guide to Huntington's medications". NHS. Retrieved on 2008-08-10.
- ↑ "Tetrabenazine as antichorea therapy in Huntington disease: a randomized controlled trial". Neurology 66 (3): 366–72. February 2006. doi:. PMID 16476934. http://www.neurology.org/cgi/pmidlookup?view=long&pmid=16476934.
- ↑ "Organised inpatient (stroke unit) care for stroke. Stroke Unit Trialists' Collaboration". Cochrane Database Syst Rev (2): CD000197. 2000. doi:. PMID 10796318.
- ↑ Turner-Stokes L, Disler PB, Nair A, Wade DT (2005). "Multi-disciplinary rehabilitation for acquired brain injury in adults of working age". Cochrane Database Syst Rev (3): CD004170. doi:. PMID 16034923.
- ↑ Zinzi P, Salmaso D, De Grandis R, et al (July 2007). "Effects of an intensive rehabilitation programme on patients with Huntington's disease: a pilot study". Clin Rehabil 21 (7): 603–13. doi:. PMID 17702702. http://cre.sagepub.com/cgi/pmidlookup?view=long&pmid=17702702.
- ↑ Bilney B, Morris ME, Perry A (March 2003). "Effectiveness of physiotherapy, occupational therapy, and speech pathology for people with Huntington's disease: a systematic review". Neurorehabil Neural Repair 17 (1): 12–24. doi:. PMID 12645441. http://nnr.sagepub.com/cgi/pmidlookup?view=long&pmid=12645441.
- ↑ Gaba, Anna. "Family Guide Series - Nutrition and Huntington's Disease". Huntington's Disease Society of America Publications. Retrieved on 2008-04-02.
- ↑ Panagiotakis PH, DiSario JA, Hilden K, Ogara M, Fang JC (2008). "DPEJ tube placement prevents aspiration pneumonia in high-risk patients". Nutr Clin Pract 23 (2): 172–5. doi:. PMID 18390785. http://ncp.sagepub.com/cgi/pmidlookup?view=long&pmid=18390785.
- ↑ Harper PS (1999). "Huntington's disease: A clinical, genetic and molecular model for polyglutamine repeat disorders". Philos. Trans. R. Soc. Lond., B, Biol. Sci. 354 (1386): 957–61. doi:. PMID 10434293.
- ↑ Andrew SE, Goldberg YP, Kremer B, et al. (1993). "The relationship between trinucleotide (CAG) repeat length and clinical features of Huntington's disease". Nat. Genet. 4 (4): 398–403. doi:. PMID 8401589.
- ↑ Rubinsztein DC, Leggo J, Chiano M, et al. (1997). "Genotypes at the GluR6 kainate receptor locus are associated with variation in the age of onset of Huntington disease". Proc. Natl. Acad. Sci. U.S.A. 94 (8): 3872–6. doi:. PMID 9108071.
- ↑ Adams P, Falek A, Arnold J (1988). "Huntington disease in Georgia: Age at onset". Am. J. Hum. Genet. 43 (5): 695–704. PMID 2973230.
- ↑ Roos RA, Hermans J, Vegter-van der Vlis M, et al. (1993). "Duration of illness in Huntington's disease is not related to age at onset". J. Neurol. Neurosurg. Psychiatr. 56 (1): 98–100. PMID 8429330.
- ↑ Lanska DJ, Lanska MJ, Lavine L, Schoenberg BS (1988). "Conditions associated with Huntington's disease at death. A case-control study". Arch. Neurol. 45 (8): 878–80. PMID 2969233.
- ↑ Di Maio L, Squitieri F, Napolitano G, et al. (1993). "Suicide risk in Huntington's disease". J. Med. Genet. 30 (4): 293–5. PMID 8487273.
- ↑ Schoenfeld M, Myers RH, Cupples LA, et al. (1984). "Increased rate of suicide among patients with Huntington's disease". J. Neurol. Neurosurg. Psychiatr. 47 (12): 1283–7. PMID 6239910.
- ↑ Squitieri F, Andrew SE, Goldberg YP, et al. (December 1994). "DNA haplotype analysis of Huntington disease reveals clues to the origins and mechanisms of CAG expansion and reasons for geographic variations of prevalence". Hum. Mol. Genet. 3 (12): 2103–14. doi:. PMID 7881406. http://hmg.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=7881406.
- ↑ Almqvist EW, Elterman DS, MacLeod PM, Hayden MR (September 2001). "High incidence rate and absent family histories in one quarter of patients newly diagnosed with Huntington disease in British Columbia". Clin. Genet. 60 (3): 198–205. doi:. PMID 11595021. http://www.blackwell-synergy.com/openurl?genre=article&sid=nlm:pubmed&issn=0009-9163&date=2001&volume=60&issue=3&spage=198.
- ↑ Avila-Giron R. (1973). "Medical and Social Aspects of Huntington's chorea in the state of Zulia, Venezuela". Advances in Neurology 1: 261–6.
- ↑ "The brief history of HD" (PDF). The HOPES Timeline - A Brief History of Huntington's Disease. standford hopes (2005-04-05). Retrieved on 2008-08-10.
- ↑ Okun MS (July 2003). "Huntington's disease: what we learned from the original essay". Neurologist 9 (4): 175–9. doi:. PMID 12864927. http://meta.wkhealth.com/pt/pt-core/template-journal/lwwgateway/media/landingpage.htm?issn=1074-7931&volume=9&issue=4&spage=175.
- ↑ Lund, Johan Christian (1860), "Chorea Sti Viti i Sætersdalen. Uddrag af Distriktslæge J. C. Lunds Medicinalberetning for 1860", Beretning om Sundhedstilstanden (Norway): 137–138
- ↑ Lanska DJ (April 2000). "George Huntington (1850-1916) and hereditary chorea". J Hist Neurosci 9 (1): 76–89. doi:. PMID 11232352.
- ↑ Jelliffe SE, Muncey EB, Davenport CB (1913). "Huntington's Chorea: A Study in Heredity". The Journal of Nervous and Mental Disease 40 (12): 796. http://scholar.google.co.uk/scholar?hl=en&lr=&q=info:s7u8s5gzl6oJ:scholar.google.com/&output=viewport&pg=1.
- ↑ Vessie, P.R. (1932), "On the transmission of Huntington's chorea for 300 years – the Bures family group", Nervous and Mental Disease (Baltimore) 76 (6): 553–573, http://scholar.google.co.uk/scholar?hl=en&lr=&q=info:12mCk4CjFKAJ:scholar.google.com/&output=viewport&pg=1
- ↑ "THE VENEZUELA HUNTINGTON'S DISEASE PROJECT". Hereditary Disease Foundation website. Hereditary Disease Foundation (2008). Retrieved on 2008-09-08.
- ↑ La Spada AR, Roling DB, Harding AE, et al. (1992). "Meiotic stability and genotype-phenotype correlation of the trinucleotide repeat in X-linked spinal and bulbar muscular atrophy". Nat. Genet. 2 (4): 301–4. doi:. PMID 1303283.
- ↑ Macdonald, M (March 1993). "A novel gene containing a trinucleotide repeat that is expanded and unstable on Huntington's disease chromosomes. The Huntington's Disease Collaborative Research Group". Cell 72 (6): 971–83. doi:. PMID 8458085. http://linkinghub.elsevier.com/retrieve/pii/0092-8674(93)90585-E.
- ↑ Sathasivam K, Hobbs C, Mangiarini L, et al (June 1999). "Transgenic models of Huntington's disease". Philos. Trans. R. Soc. Lond., B, Biol. Sci. 354 (1386): 963–9. doi:. PMID 10434294. PMC: 1692600. http://journals.royalsociety.org/openurl.asp?genre=article&issn=0962-8436&volume=354&issue=1386&spage=963.
- ↑ Li JY, Popovic N, Brundin P (July 2005). "The use of the R6 transgenic mouse models of Huntington's disease in attempts to develop novel therapeutic strategies". NeuroRx 2 (3): 447–64. doi:. PMID 16389308.
- ↑ "Achievements of Hereditary Disease Foundation". Achievements of Hereditary Disease Foundation. Hereditary Disease Foundation. Retrieved on 2008-08-10.
- ↑ "HDA research news—medical research into treatment & prevention on hda.org.uk". Retrieved on 2008-08-10.
- ↑ "Alice's Restaurant". IMDB. Retrieved on 2008-08-30.
- ↑ "ER (1994)". IMDB. Retrieved on 2008-08-30.
- ↑ "Private Practice (2007)". IMDB. Retrieved on 2008-08-30.
- ↑ "Everwood (2002)". IMDB. Retrieved on 2008-08-30.
- ↑ "All Saints (1998)". IMDB. Retrieved on 2008-08-30.
- ↑ "House M.D.". IMDB. Retrieved on 2008-08-30.
- ↑ Seagle, Steven T.; Teddy Kristiansen (2004). It's a Bird. New York: Vertigo. pp. 123. ISBN 978-1401203115. http://www.worldcat.org/oclc/55071368?tab=details#tabs.
- ↑ "US Senate s. resolution 531" (PDF). S. Res. 531. US Senate (2008-04-06). Retrieved on 2008-08-10.
- ↑ Chapman MA (July 1990). "Predictive testing for adult-onset genetic disease: ethical and legal implications of the use of linkage analysis for Huntington disease". Am. J. Hum. Genet. 47 (1): 1–3. PMID 2140926.
- ↑ Huggins M, Bloch M, Kanani S, et al (July 1990). "Ethical and legal dilemmas arising during predictive testing for adult-onset disease: the experience of Huntington disease". Am. J. Hum. Genet. 47 (1): 4–12. PMID 1971997.
- ↑ "Guidelines for the molecular genetics predictive test in Huntington's disease. International Huntington Association (IHA) and the World Federation of Neurology (WFN) Research Group on Huntington's Chorea". Neurology 44 (8): 1533–6. August 1994. PMID 8058167.
- ↑ Tibben A, Vegter-van der Vlis M, Skraastad MI, et al (September 1992). "DNA-testing for Huntington's disease in The Netherlands: a retrospective study on psychosocial effects". Am. J. Med. Genet. 44 (1): 94–9. doi:. PMID 1387764.
- ↑ Bloch M, Hayden MR (January 1990). "Opinion: predictive testing for Huntington disease in childhood: challenges and implications". Am. J. Hum. Genet. 46 (1): 1–4. PMID 2136787.
- ↑ Binedell J, Soldan JR, Scourfield J, Harper PS (November 1996). "Huntington's disease predictive testing: the case for an assessment approach to requests from adolescents". J. Med. Genet. 33 (11): 912–8. PMID 8950670.
- ↑ Wertz DC, Fanos JH, Reilly PR (September 1994). "Genetic testing for children and adolescents. Who decides?". JAMA 272 (11): 875–81. doi:. PMID 8078166.
- ↑ Hoffmann DE, Wulfsberg EA (1995). "Testing children for genetic predispositions: is it in their best interest?". J Law Med Ethics 23 (4): 331–44. doi:. PMID 8715053.
- ↑ Gómez-Esteban JC, Lezcano E, Zarranz JJ, et al (2007). "Monozygotic twins suffering from Huntington's disease show different cognitive and behavioral symptoms". Eur. Neurol. 57 (1): 26–30. doi:. PMID 17108691. http://content.karger.com/produktedb/produkte.asp?typ=fulltext&file=ENE2007057001026.
- ↑ Kuliev A, Verlinsky Y (April 2005). "Place of preimplantation diagnosis in genetic practice". Am. J. Med. Genet. A 134A (1): 105–10. doi:. PMID 15732064.
- ↑ Davenport CB (May 1915). "Huntington's chorea in relation to heredity and eugenics". Proc. Natl. Acad. Sci. U.S.A. 1 (5): 283–5. doi:. PMID 16575999.
- ↑ "BBC article: Genetic data banned for insurers". BBC (2008-06-13). Retrieved on 2008-08-10.
- ↑ "Huntington's Disease Society of America HDSA". http://www.hdsa.org/ Huntington's Disease Society of America website. HDSA. Retrieved on 2008-08-10.
- ↑ "World Congress on Huntington's Disease World Congress on Huntington's Disease website". Retrieved on 2008-08-10.
- ↑ "Euro-HD Network Euro-HD website". Retrieved on 2008-08-10.
- ↑ "Huntington Project Huntington Porject website". Retrieved on 2008-08-10.
- ↑ "High-Q Foundation HighQ foundation website". HighQ. Retrieved on 2008-08-10.
- ↑ Beal MF, Kowall NW, Ellison DW, Mazurek MF, Swartz KJ, Martin JB (1986). "Replication of the neurochemical characteristics of Huntington's disease by quinolinic acid". Nature 321 (321): 168–71. doi:. PMID 2422561.
- ↑ Brouillet E, Hantraye P, Ferrante RJ, Dolan R, Leroy-Willig A, Kowall NW, Beal MF (1995). "Chronic mitochondrial energy impairment produces selective striatal degeneration and abnormal choreiform movements in primates". Proc Natl Acad Sci USA 92: 7105–7109. doi:. PMID 7624378.
- ↑ Mangiarini L, Sathasivam K, Seller M, Cozens B, Harper A, Hetherington C, Lawton M, Trottier Y, Lehrach H, Davies SW, Bates GP (November 1996). "Exon 1 of the HD gene with an expanded CAG repeat is sufficient to cause a progressive neurological genotype in transgenic mice". Cell 87 (3): 493–506. doi:. PMID 8898202.
- ↑ Carter RJ, Lione LA, Humby T, Mangiarini L, Mahal A, Bates GP, Dunnett SB, and Morton AJ (April 1999). "Characterization of Progressive Motor Deficits in Mice Transgenic for the Human Huntington's Disease Mutation". The Journal of Neuroscience 19 (8): 3248–3257. PMID 10191337. http://www.jneurosci.org/cgi/content/full/19/8/3248.
- ↑ Marsh JL, Pallos J and Thompson LM (2003). "Fly models of Huntington's disease". Human Molecular Genetics 12 (2): 187–193. doi:. PMID 12925571. http://hmg.oxfordjournals.org/cgi/content/full/12/suppl_2/R187.
- ↑ "Science Daily article on HD monkey model". First Transgenic Monkey Model Of Huntington's Disease Developed. ScienceDaily (2008-05-19). Retrieved on 2008-08-10.
- ↑ Voisine C, Varma H, Walker N, Bates EA, Stockwell BR, Hart AC (2007). "Identification of potential therapeutic drugs for huntington's disease using Caenorhabditis elegans". PLoS ONE 2 (6): e504. doi:. PMID 17551584. PMC: 1876812. http://www.plosone.org/article/info:doi/10.1371/journal.pone.0000504.
- ↑ Lecerf JM, Shirley TL, Zhu Q, et al. (2001). "Human single-chain Fv intrabodies counteract in situ huntingtin aggregation in cellular models of Huntington's disease". Proc. Natl. Acad. Sci. U.S.A. 98 (8): 4764–9. doi:. PMID 11296304.
- ↑ Miller TW, Zhou C, Gines S, et al. (2005). "A human single-chain Fv intrabody preferentially targets amino-terminal Huntingtin's fragments in striatal models of Huntington's disease". Neurobiol. Dis. 19 (1-2): 47–56. doi:. PMID 15837560.
- ↑ Wolfgang WJ, Miller TW, Webster JM, et al. (2005). "Suppression of Huntington's disease pathology in Drosophila by human single-chain Fv antibodies". Proc. Natl. Acad. Sci. U.S.A. 102 (32): 11563–8. doi:. PMID 16061794.
- ↑ Miller TW, Messer A (2005). "Intrabody applications in neurological disorders: Progress and future prospects". Mol. Ther. 12 (3): 394–401. doi:. PMID 15964243.
- ↑ Messer A, McLear J (2006). "The therapeutic potential of intrabodies in neurologic disorders: focus on Huntington and Parkinson diseases". BioDrugs 20 (6): 327–33. doi:. PMID 17176119.
- ↑ Harper SQ, Staber PD, He X, et al. (2005). "RNA interference improves motor and neuropathological abnormalities in a Huntington's disease mouse model". Proc. Natl. Acad. Sci. U.S.A. 102 (16): 5820–5. doi:. PMID 15811941.
- ↑ Jodi L. McBride et al. (2008). "Artificial miRNAs mitigate shRNA-mediated toxicity in the brain: Implications for the therapeutic development of RNAi". PNAS 105 (15): 5868–5873. doi:. PMID 18398004.
- ↑ Miguel Díaz-Hernández, Jesús Torres-Peraza, Alejandro Salvatori-Abarca, et al. (October 19, 2005). "Full Motor Recovery Despite Striatal Neuron Loss and Formation of Irreversible Amyloid-Like Inclusions in a Conditional Mouse Model of Huntington's Disease". The Journal of Neuroscience 25 (42): 9773–9781. doi:. PMID 16237181.
- ↑ "Pig cell implants in Huntington's trial". WorldHealth.net. Retrieved on 2008-05-15.
- ↑ "Trials for Huntington's disease at clinicaltrials.gov". Retrieved on 2008-08-10.
- ↑ Mostert JP, Koch MW, Heerings M, Heersema DJ, De Keyser J (2008). "Therapeutic potential of fluoxetine in neurological disorders". CNS Neurosci Ther 14 (2): 153–64. doi:. PMID 18482027.
Bibliography
- Conomy, John P., M.D., J.D. "Dr. George Huntington and the Disease Bearing His Name". Retrieved on 2008-08-15.
- Online 'Mendelian Inheritance in Man' (OMIM) Huntington Disease -143100
- Online 'Mendelian Inheritance in Man' (OMIM) Huntingtons Disease-Like 2 -606438
- Stevenson, Charles S. (April 1934). "A Biography of George Huntington, M.D" (Microsoft Word). Bulletin of the Institute of the History of Medicine (Johns Hopkins University) II (2). http://www.shv.ch/download/BiographyGeorgeHuntington.doc. Retrieved on 2007-12-05.
- Vessie, P. R. (1932). "On the transmission of Huntington's chorea for 300 years—the Bures family group". Journal of Nervous and Mental Disease, Baltimore 76: 553–573.
- Gillian Bates, Peter Harper, and Lesley Jones (2002). Huntington's Disease - Third Edition. Oxford: Oxford University Press. ISBN 0-19-851060-8.
External links
- DMOZ HD links directory at the Open Directory Project.
Professional and research
- Huntington Project - worldwide umbrella organization for the clinical research efforts for HD.
- Huntington Study Group
- Huntington's Disease Research - Research abstracts on HD.
- Huntington's Outreach Project for Education, at Stanford (HOPES) - A layperson's guide to HD
- Worldwide Education and Awareness for Movement Disorders - HD section
- University College London Huntington's Disease Research
- TRACK-HD, an international observational study of HD
- University California and San Francisco Memory and Aging Center - HD Info
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||