Heparin
 |
|
 |
|
|
Heparin
|
|
| Systematic (IUPAC) name | |
| see Heparin structure | |
| Identifiers | |
| CAS number | |
| ATC code | B01 C05 S01 |
| PubChem | |
| DrugBank | |
| ChemSpider | |
| Chemical data | |
| Formula | C12H19NO20S3 |
| Mol. mass | 12000–15000 g/mol |
| Pharmacokinetic data | |
| Bioavailability | nil |
| Metabolism | hepatic |
| Half life | 1.5 hrs |
| Excretion | ? |
| Therapeutic considerations | |
| Pregnancy cat. |
C |
| Legal status |
? |
| Routes | i.v., s.c. |
Heparin, a highly-sulfated glycosaminoglycan, is widely used as an injectable anticoagulant and has the highest negative charge density of any known biological molecule.[1] It can also be used to form an inner anticoagulant surface on various experimental and medical devices such as test tubes and renal dialysis machines. Pharmaceutical grade heparin is derived from mucosal tissues of slaughtered meat animals such as porcine (pig) intestine or bovine (cow) lung.[2]
Although used principally in medicine for anticoagulation, the true physiological role in the body remains unclear, because blood anti-coagulation is achieved mostly by endothelial cell-derived heparan sulfate proteoglycans.[3] Heparin is usually stored within the secretory granules of mast cells and released only into the vasculature at sites of tissue injury. It has been proposed that, rather than anticoagulation, the main purpose of heparin is in a defensive mechanism at sites of tissue injury against invading bacteria and other foreign materials.[4] In addition, it is preserved across a number of widely different species, including some invertebrates which lack a similar blood coagulation system.
Contents |
Heparin structure
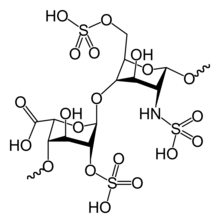
Native heparin is a polymer with a molecular weight ranging from 3 kDa to 50 kDa, although the average molecular weight of most commercial heparin preparations is in the range of 12 kDa to 15 kDa. Heparin is a member of the glycosaminoglycan family of carbohydrates (which includes the closely-related molecule heparan sulfate) and consists of a variably-sulfated repeating disaccharide unit.[5] The main disaccharide units that occur in heparin are shown below. The most common disaccharide unit is composed of a 2-O-sulfated iduronic acid and 6-O-sulfated, N-sulfated glucosamine, IdoA(2S)-GlcNS(6S). For example, this makes up 85% of heparins from beef lung and about 75% of those from porcine intestinal mucosa.[6] Not shown below are the rare disaccharides containing a 3-O-sulfated glucosamine (GlcNS(3S,6S)) or a free amine group (GlcNH3+). Under physiological conditions, the ester and amide sulfate groups are deprotonated and attract positively-charged counterions to form a heparin salt. It is in this form that heparin is usually administered as an anticoagulant.
1 unit of heparin (the "Howell Unit") is an amount approximately equivalent to 0.002 mg of pure heparin, which is the quantity required to keep 1 mL of cat's blood fluid for 24 hours at 0°C. [7]
Abbreviations
- GlcA = β-D-glucuronic acid
- IdoA = α-L-iduronic acid
- IdoA(2S) = 2-O-sulfo-α-L-iduronic acid
- GlcNAc = 2-deoxy-2-acetamido-α-D-glucopyranosyl
- GlcNS = 2-deoxy-2-sulfamido-α-D-glucopyranosyl
- GlcNS(6S) = 2-deoxy-2-sulfamido-α-D-glucopyranosyl-6-O-sulfate
Three-dimensional structure
The three-dimensional structure of heparin is complicated by the fact that iduronic acid may be present in either of two low-energy conformations when internally positioned within an oligosaccharide. The conformational equilibrium being influenced by sulfation state of adjacent glucosamine sugars.[8] Nevertheless, the solution structure of a heparin dodecasacchride composed solely of six GlcNS(6S)-IdoA(2S) repeat units has been determined using a combination of NMR spectroscopy and molecular modeling techniques.[9] Two models were constructed, one in which all IdoA(2S) were in the 2S0 conformation (A and B below), and one in which they are in the 1C4 conformation (C and D below). However there is no evidence to suggest that changes between these conformations occur in a concerted fashion. These models correspond to the protein data bank code 1HPN.
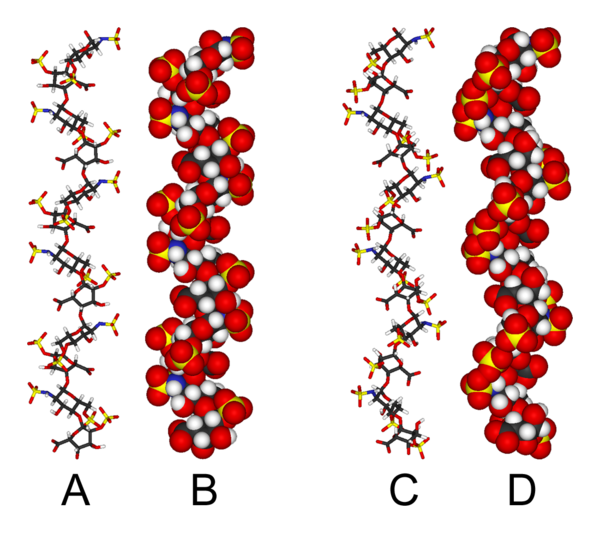
In the image above:
- A = 1HPN (all IdoA(2S) residues in 2S0 conformation) Jmol viewer
- B = van der Waals radius space filling model of A
- C = 1HPN (all IdoA(2S) residues in 1C4 conformation) Jmol viewer
- D = van der Waals radius space filling model of C
In these models, heparin adopts a helical conformation, the rotation of which places clusters of sulfate groups at regular intervals of about 17 angstroms (1.7 nm) on either side of the helical axis.
Medical use
Heparin is a naturally-occurring anticoagulant produced by basophils and mast cells.[10] Heparin acts as an anticoagulant, preventing the formation of clots and extension of existing clots within the blood. While heparin does not break down clots that have already formed (unlike tissue plasminogen activator), it allows the body's natural clot lysis mechanisms to work normally to break down clots that have already formed. Heparin is used for anticoagulation for the following conditions:
- Acute coronary syndrome, e.g., myocardial infarction
- Atrial fibrillation
- Deep-vein thrombosis and pulmonary embolism
- Cardiopulmonary bypass for heart surgery.
Heparin and its derivatives (enoxaparin, dalteparin, and so forth) are effective at preventing deep-vein thromboses and pulmonary emboli in patients at risk,[11][12] but there is no evidence that they are effective at preventing death.[13] Current guidelines recommend aspirin and leg stockings instead.[14]
Mechanism of anticoagulant action
Heparin binds to the enzyme inhibitor antithrombin (AT) causing a conformational change that results in its activation through an increase in the flexibility of its reactive site loop.[15] The activated AT then inactivates thrombin and other proteases involved in blood clotting, most notably factor Xa. The rate of inactivation of these proteases by AT can increase by up to 1000-fold due to the binding of heparin.[16]
AT binds to a specific pentasaccharide sulfation sequence contained within the heparin polymer
GlcNAc/NS(6S)-GlcA-GlcNS(3S,6S)-IdoA(2S)-GlcNS(6S)
The conformational change in AT on heparin-binding mediates its inhibition of factor Xa. For thrombin inhibition however, thrombin must also bind to the heparin polymer at a site proximal to the pentasaccharide. The highly-negative charge density of heparin contributes to its very strong electrostatic interaction with thrombin.[1] The formation of a ternary complex between AT, thrombin, and heparin results in the inactivation of thrombin. For this reason heparin's activity against thrombin is size-dependent, the ternary complex requiring at least 18 saccharide units for efficient formation.[17] In contrast anti factor Xa activity only requires the pentasaccharide binding site.

This size difference has led to the development of low-molecular-weight heparins (LMWHs) and more recently to fondaparinux as pharmaceutical anticoagulants. Low-molecular-weight heparins and fondaparinux target anti-factor Xa activity rather than anti-thrombin (IIa) activity, with the aim of facilitating a more subtle regulation of coagulation and an improved therapeutic index. The chemical structure of fondaparinux is shown to the left. It is a synthetic pentasaccharide, whose chemical structure is almost identical to the AT binding pentasaccharide sequence that can be found within polymeric heparin and heparan sulfate.
With LMWH and fondaparinux, there is a reduced risk of osteoporosis and heparin-induced thrombocytopenia (HIT). Monitoring of the APTT is also not required and indeed does not reflect the anticoagulant effect, as APTT is insensitive to alterations in factor Xa.
Danaparoid, a mixture of heparan sulfate, dermatan sulfate, and chondroitin sulfate can be used as an anticoagulant in patients who have developed HIT. Because danaparoid does not contain heparin or heparin fragments, cross-reactivity of danaparoid with heparin-induced antibodies is reported as less than 10%.[18]
The effects of heparin are measured in the lab by the partial thromboplastin time (aPTT), (the time it takes the blood plasma to clot).
Administration
Details of administration are available in clinical practice guidelines by the American College of Chest Physicians:[19]
Heparin is given parenterally, as it is degraded when taken by mouth. It can be injected intravenously or subcutaneously (under the skin). Intramuscular injections (into muscle) are avoided because of the potential for forming hematomas.
Because of its short biologic half-life of approximately one hour, heparin must be given frequently or as a continuous infusion. However, the use of low molecular weight heparin (LMWH) has allowed once daily dosing, thus not requiring a continuous infusion of the drug. If long-term anticoagulation is required, heparin is often used only to commence anticoagulation therapy until the oral anticoagulant warfarin takes effect.
Adverse reactions
A serious side-effect of heparin is heparin-induced thrombocytopenia (HIT syndrome). HITS is caused by an immunological reaction that makes platelets a target of immunological response, resulting in the degradation of platelets. This is what causes thrombocytopenia. This condition is usually reversed on discontinuation, and can generally be avoided with the use of synthetic heparins. There is also a benign form of thrombocytopenia associated with early heparin use, which resolves without stopping heparin.
Two nonhemorrhagic side effects of heparin treatment. The first is elevation of serum aminotransferase levels, which has been reported in as many as 80% of patients receiving heparin. This abnormality is not associated with liver dysfunction, and it disappears after the drug is discontinued. The other complication is hyperkalemia, which occurs in 5 to 10% of patients receiving heparin, and is the result of heparin-induced aldosterone suppression. The hyperkalemia can appear within a few days after the onset of heparin therapy.
Rarer side-effects include alopecia and osteoporosis with chronic use.
As with many drugs, overdoses of heparin can be fatal. In September 2006, heparin received worldwide publicity when 3 prematurely-born infants died after they were mistakenly given overdoses of heparin at an Indianapolis hospital.[20]
Treatment of overdose
In case of overdose, protamine sulfate (1 mg per 100 Units of Heparin that had been given over 4 hours) can be given to counteract the action of heparin.
History
Heparin is one of the oldest drugs currently still in widespread clinical use. Its discovery in 1916 predates the establishment of the United States Food and Drug Administration, although it did not enter clinical trials until 1935.[21] It was originally isolated from canine liver cells, hence its name (hepar or "ηπαρ" is Greek for "liver"). Heparin's discovery can be attributed to the research activities of two men, Jay McLean and William Henry Howell.
In 1916, McLean, a second-year medical student at Johns Hopkins University, was working under the guidance of Howell investigating pro-coagulant preparations, when he isolated a fat-soluble phosphatide anti-coagulant. It was Howell who coined the term heparin for this type of fat-soluble anticoagulant in 1918. In the early 1920s, Howell isolated a water-soluble polysaccharide anticoagulant, which was also termed heparin, although it was distinct from the phosphatide preparations previously isolated. It is probable that the work of McLean changed the focus of the Howell group to look for anticoagulants, which eventually led to the polysaccharide discovery.
Between 1933 and 1936, Connaught Medical Research Laboratories, then a part of the University of Toronto, perfected a technique for producing safe, non-toxic heparin that could be administered to patients in a salt solution. The first human trials of heparin began in May 1935, and, by 1937, it was clear that Connaught's heparin was a safe, easily-available, and effective blood anticoagulant. Prior to 1933, heparin was available, but in small amounts, and was extremely expensive, toxic, and, as a consequence, of no medical value.[22]
For a full discussion of the events surrounding heparin's discovery see Marcum J. (2000).[23]
Novel drug development opportunities for heparin
As detailed in the table below, there is a great deal of potential for the development of heparin-like structures as drugs to treat a wide range of diseases, in addition to their current use as anticoagulants.[24][25]
| Disease states sensitive to heparin | Heparins effect in experimental models | Clinical status |
| Adult respiratory distress syndrome | Reduces cell activation and accumulation in airways, neutralizes mediators and cytotoxic cell products, and improves lung function in animal models | Controlled clinical trials |
| Allergic encephalomyelitis | Effective in animal models | - |
| Allergic rhinitis | Effects as for adult respiratory distress syndrome, although no specific nasal model has been tested | Controlled clinical trial |
| Arthritis | Inhibits cell accumulation, collagen destruction and angiogenesis | Anecdotal report |
| Asthma | As for adult respiratory distress syndrome, however it has also been shown to improve lung function in experimental models | Controlled clinical trials |
| Cancer | Inhibits tumour growth, metastasis and angiogenesis, and increases survival time in animal models | Several anecdotal reports |
| Delayed type hypersensitivity reactions | Effective in animal models | - |
| Inflammatory bowel disease | Inhibits inflammatory cell transport in general. No specific model tested | Controlled clinical trials |
| Interstitial cystitis | Effective in a human experimental model of interstitial cystitis | Related molecule now used clinically |
| Transplant rejection | Prolongs allograph survival in animal models | - |
- indicates no information available
As a result of heparin's effect on such a wide variety of disease states a number of drugs are indeed in development whose molecular structures are identical or similar to those found within parts of the polymeric heparin chain.[24]
| Drug molecule | Effect of new drug compared to heparin | Biological activities |
| Heparin tetrasaccharide | Non-anticoagulant, non-immunogenic, orally active | Anti-allergic |
| Pentosan polysulfate | Plant derived, little anticoagulant activity, Anti-inflammatory, orally active | Anti-inflammatory, anti-adhesive, anti-metastatic |
| Phosphomannopentanose sulfate | Potent inhibitor of heparanase activity | Anti-metastatic, anti-angiogenic, anti-inflammatory |
| Selectively chemically O-desulphated heparin | Lacks anticoagulant activity | Anti-inflammatory, anti-allergic, anti-adhesive |
De-polymerisation techniques
Either chemical or enzymatic de-polymerisation techniques or a combination of the two underlie the vast majority of analyses carried out on the structure and function of heparin and heparan sulfate (HS).
Enzymatic
The enzymes traditionally used to digest heparin or HS are naturally produced by the soil bacterium Pedobacter heparinus (formerly named Flavobacterium heparinum).[26] This bacterium is capable of utilizing either heparin or HS as its sole carbon and nitrogen source. In order to do this it produces a range of enzymes such as lyases, glucuronidases, sulfoesterases and sulfamidases.[27] It is the lyases that have mainly been used in heparin/HS studies. The bacterium produces three lyases, heparinases I (EC 4.2.2.7), II (no EC number assigned) and III (EC 4.2.2.8) and each has distinct substrate specificities as detailed below.[28][29]
| Heparinase enzyme | Substrate specificity |
| Heparinase I | GlcNS(±6S)-IdoA(2S) |
| Heparinase II | GlcNS/Ac(±6S)-IdoA(±2S) GlcNS/Ac(±6S)-GlcA |
| Heparinase III | GlcNS/Ac(±6S)-GlcA/IdoA (with a preference for GlcA) |

The lyases cleave heparin/HS by a beta elimination mechanism. This action generates an unsaturated double bond between C4 and C5 of the uronate residue.[30][31] The C4-C5 unsaturated uronate is termed ΔUA or UA. It is a sensitive UV chromaphore (max absorption at 232nm) and allows the rate of an enzyme digest to be followed as well as providing a convenient method for detecting the fragments produced by enzyme digestion.
Chemical
Nitrous acid can be used to chemically de-polymerise heparin/HS. Nitrous acid can be used at pH 1.5 or at a higher pH of 4. Under both conditions nitrous acid effects deaminative cleavage of the chain.[32]

At both 'high' (4) and 'low' (1.5) pH, deaminative cleavage occurs between GlcNS-GlcA and GlcNS-IdoA, all be it at a slower rate at the higher pH. The deamination reaction, and therefore chain cleavage, is regardless of O-sulfation carried by either monosaccharide unit.
At low pH deaminative cleavage results in the release of inorganic SO4, and the conversion of GlcNS into anhydromannose (aMan). Low pH nitrous acid treatment is an excellent method to distinguish N-sulfated polysaccharides such as heparin and HS from non N-sulfated polysacchrides such as chondroitin sulfate and dermatan sulfate; chondroitin sulfate and dermatan sulfate being un-susceptable to nitrous acid cleavage.
Evolutionary conservation
In addition to the bovine and porcine tissue from which pharmaceutical-grade heparin is commonly extracted, heparin has also been extracted and characterised from the following species:
The biological activity of heparin within species 6–11 is unclear and further supports the idea that the main physiological role of heparin is not anticoagulation. These species do not possess any blood coagulation system similar to that present within the species listed 1–5. The above list also demonstrates how heparin has been highly evolutionarily conserved with molecules of a similar structure being produced by a broad range of organisms belonging to many different phyla.
Other uses/information
- Heparin gel (topical) may sometimes be used to treat sports injuries. It is known that the diprotonated form of histamine binds site specifically to heparin.[43] The release of histamine from mast cells at a site of tissue injury contributes to an inflammatory response. The rationale behind the use of such topical gels may be to block the activity of released histamine, and so help to reduce inflammation.
- Heparin gains the capacity to initiate angiogenesis when its copper salt is formed. Copper-free molecules are non-angiogenic.[44][45] In contrast heparin may inhibit angiogenesis when it is administered in the presence of corticosteroids.[46] This anti-angiogenic effect is independent of heparins anticoagulant activity.[47]
- Test tubes, Vacutainers, and capillary tubes that use the lithium salt of heparin (lithium heparin) as an anticoagulant are usually marked with green stickers and green tops. Heparin has the advantage over EDTA of not affecting levels of most ions. However it has been shown that the levels of ionized calcium may be decreased if the concentration of heparin in the blood specimen is too high.[48] Heparin can interfere with some immunoassays, however. As lithium heparin is usually used, a person's lithium levels cannot be obtained from these tubes; for this purpose, royal-blue-topped Vacutainers containing sodium heparin are used.
- Heparin-coated blood oxygenators are available for use in heart-lung machines. Among other things, these specialized oxygenators are thought to improve overall biocompatibility and host homeostasis by providing characteristics similar to native endothelium.
- The DNA binding sites on RNA polymerase can be occupied by heparin, preventing the polymerase binding to promoter DNA. This property is exploited in a range of molecular biological assays.
- Common diagnostic procedures require PCR amplification of a patient's DNA, which is easily extracted from white blood cells treated with heparin. This poses a potential problem, since heparin may be extracted along with the DNA, and it has been found to interfere with the PCR reaction at levels as low as 0.002 U in a 50 μL reaction mixture.[49]
- Immobilized heparin can be used as an affinity ligand in protein purification. The format of immobilized heparin can vary widely from coated plastic surfaces for diagnostic purposes to chromatography resin. Most types of immobilized heparin can be used in three ways. The first of which is to use heparin to select out specific coagulation factors or other types of heparin-binding proteins from a complex mixture of non-heparin-binding proteins. Specific proteins can then be selectively dissociated from heparin with the use of differing salt concentrations or by use of a salt gradient. The second use is to use heparin as a high-capacity cation exchanger. This use takes advantage of heparins high number of anionic sulfate groups. These groups will capture common cations such as Na+ or Ca2+ in solution. The third use for immoblized heparin is group-specific purification of RNA and DNA binding proteins such as transcription factors and/or virus coat proteins. This methodology takes advantage of heprin's similar properties to RNA and DNA i.e. negatively charged sugar molecule.
- Heparin does not break up fibrin, it only prevents conversion of fibrinogen to fibrin. Only thrombolytics can break up a clot.
Controversies
Contamination recalls
In December 2007, the FDA recalled a shipment of heparin because of a growth of Serratia marcescens in several unopened syringes of this product. The bacteria Serratia marcescens can lead to life-threatening injuries and/or death.[50]
In March 2008, major recalls of heparin were announced by the FDA due to contamination of the raw heparin stock imported from China.[51][52] The contaminant was identified as an "over-sulphated" derivative of chondroitin sulfate, a popular shellfish-derived supplement often used for arthritis.[53]
Use in homicide
In 2006, Petr Zelenka, a nurse in the Czech Republic, deliberately administered large doses to patients, killing 7, and attempting to kill 10 others.[54]
Overdose issues
Actor Dennis Quaid's twelve-day-old twins mistakenly were given an adult dosage, which is 1,000 times the recommended dosage for infants, in November 2007.[55] The overdose allegedly arose because the labeling and design of the adult and infant versions of the product were easily confused. The Quaid family subsequently sued the manufacturer, Baxter Healthcare Corp., for over $50,000.[56][57]
In July 2008, another set of twins born at Christus Spohn Hospital South, a Texas hospital, died after an accidentally administered overdose of the drug. The overdose was due to a mixing error at the hospital pharmacy and, unlike the Quaid case, was unrelated to the product's packaging or labeling.[58] As of July 2008[update], whether the deaths were due to the overdose is under investigation.[59][60]
Popular culture
- Heparin was featured in Dan Brown's novel Angels and Demons, in which the intentional overdose of the drug was used in the murder of a significant character that was disguised to resemble a death by stroke.
- Heparin was also featured in the television film The Andromeda Strain as a way to stop a mysterious alien disease from clotting people's blood.
- Heparin was used in the movie Untraceable when a serial killer injects a man with an overdose of Heparin live on the internet. The steady drip causes the man to bleed to death in front of millions of viewers.
- Heparin was used in the television series Dexter to prevent clotting of the blood drained from the victims of a serial killer, so it can be stored for a later purpose
References
- ↑ 1.0 1.1 Cox, M.; Nelson D. (2004). Lehninger, Principles of Biochemistry. Freeman. pp. 1100. ISBN 0-71674339-6.
- ↑ Linhardt RJ, Gunay NS. (1999). "Production and Chemical Processing of Low Molecular Weight Heparins". Sem. Thromb. Hem. 3: 5–16. PMID 10549711.
- ↑ Marcum JA, McKenney JB. et al. (1986). "Anticoagulantly active heparin-like molecules from mast cell-deficient mice". Am. J. Physiol. 250 (5 Pt 2): H879–888. PMID 3706560.
- ↑ Nader, HB et al. (1999). "Heparan sulfates and heparins: similar compounds performing the same functions in vertebrates and invertebrates?". Braz. J. Med. Biol. Res. 32 (5): 529–538. doi:. PMID 10412563.
- ↑ Bentolila, A. et al.. "Synthesis and heparin-like biological activity of amino acid-based polymers". Wiley InterScience. Retrieved on 2008-03-10.
- ↑ Gatti, G., Casu, B. et al. (1979). "Studies on the Conformation of Heparin by lH and 13C NMR Spectroscopy". Macromolecules 12 (5): 1001–1007. doi:. http://pubs.acs.org/cgi-bin/abstract.cgi/mamobx/1979/12/i05/f-pdf/f_ma60071a044.pdf.
- ↑ "Online Medical Dictionary". Centre for Cancer Education (2000). Retrieved on 2008-07-11.
- ↑ Ferro D, Provasoli A, et al. (1990). "Conformer populations of L-iduronic acid residues in glycosaminoglycan sequences". Carbohydr. Res. 195: 157–167. doi:. PMID 2331699.
- ↑ Mulloy B, Forster MJ, Jones C, Davies DB. (1993). "NMR and molecular-modelling studies of the solution conformation of heparin". Biochem. J. 293: 849–858. PMID 8352752. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pubmed&pubmedid=8352752.
- ↑ Guyton, A. C.; Hall, J. E. (2006). Textbook of Medical Physiology. Elsevier Saunders. pp. 464. ISBN 0-7216-0240-1.
- ↑ Agnelli G, Piovella F, Buoncristiani P, et al. (1998). "Enoxaparin plus compression stockings compared with compression stockings alone in the prevention of venous thromboembolism after elective neurosurgery". N Engl J Med 339 (2): 80–5. doi:. PMID 9654538.
- ↑ Bergqvist D, Agnelli G, Cohen AT, et al. (2002). "Duration of prophylaxis against venous thromboembolism with enoxaparin after surgery for cancer". N Engl J Med 346 (13): 975–980. doi:. PMID 11919306. http://content.nejm.org/cgi/content/abstract/346/13/975.
- ↑ Handoll HHG, Farrar MJ, McBirnie J, Tytherleigh-Strong G, Milne AA, Gillespie WJ (2002). "Heparin, low molecular weight heparin and physical methods for preventing deep vein thrombosis and pulmonary embolism following surgery for hip fractures". Cochrane Database Syst Rev 4: CD000305. doi:.
- ↑ Scottish Intercollegiate Guidelines Network (2002). "Prophylaxis of venous thromboembolism". Edinburgh: Scottish Intercollegiate Guidelines Network. Retrieved on 2008-06-08.
- ↑ Chuang YJ, Swanson R. et al. (2001). "Heparin enhances the specificity of antithrombin for thrombin and factor Xa independent of the reactive center loop sequence. Evidence for an exosite determinant of factor Xa specificity in heparin-activated antithrombin". J. Biol. Chem. 276 (18): 14961–14971. doi:. PMID 11278930.
- ↑ Bjork I, Lindahl U. (1982). "Mechanism of the anticoagulant action of heparin". Mol. Cell. Biochem. 48: 161–182. doi:. http://www.springerlink.com/content/g67115564280w013/.
- ↑ Petitou M, Herault JP, Bernat A, Driguez PA, et al. (1999). "Synthesis of Thrombin inhibiting Heparin mimetics without side effects". Nature 398: 417–422. doi:. PMID 10201371.
- ↑ Shalansky, Karen. DANAPAROID (Orgaran®) for Heparin-Induced Thrombocytopenia. Vancouver Hospital & Health Sciences Centre, February 1998 Drug & Therapeutics Newsletter. Retrieved on 2007-01-08.
- ↑ Hirsh J, Raschke R (2004). "Heparin and low-molecular-weight heparin: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy". Chest 126 (3 Suppl): 188S–203S. doi:. PMID 15383472.
- ↑ Kusmer, Ken (2006-09-20). "3rd Ind. preemie infant dies of overdose", Fox News (Associated Press). Retrieved on 2007-01-08.
- ↑ Linhardt RJ. (1991). "Heparin: An important drug enters its seventh decade". Chem. Indust. 2: 45–50.
- ↑ Rutty, CJ. "Miracle Blood Lubricant: Connaught and the Story of Heparin, 1928–1937". Health Heritage Research Services. Retrieved on 2007-05-21.
- ↑ Marcum J. (2000). "The origin of the dispute over the discovery of heparin". J. Hist. Med. Allied. Sci. 55: 37–66. doi:. PMID 10734720.
- ↑ 24.0 24.1 Lever R. and Page C.P. (2002). "Novel drug opportunities for heparin". Nat. Rev. Drug Discov. 1 (2): 140–148. doi:. PMID 12120095.
- ↑ Coombe D.R and Kett W.C. (2005). "Heparan sulfate-protein interactions: therapeutic potential through structure-function insights". Cell. Mol. Life Sci. 62 (4): 410–424. doi:. PMID 15719168.
- ↑ Shaya D, Tocilj A. et al. (2006). "Crystal structure of heparinase II from Pedobacter heparinus and its complex with a disaccharide product". J. Biol. Chem. 281 (22): 15525–15535. doi:. PMID 16565082.
- ↑ Galliher PM, Cooney CL. et al. (1981). "Heparinase production by Flavobacterium heparinum". Appl. Environ. Microbiol. 41 (2): 360–365. PMID 7235692.
- ↑ Linhardt RJ, Turnbull JE. et al. (1990). "Examination of the substrate specificity of heparin and heparan sulfate lyases". Biochemistry 29 (10): 2611–2617. doi:. PMID 2334685.
- ↑ Desai UR, Wang HM. and Linhardt RJ. (1993). "Specificity studies on the heparin lyases from Flavobacterium heparinum". Biochemistry 32 (32): 8140–8145. doi:. PMID 8347612.
- ↑ Linker A, Hovingh P. (1972). "Isolation and characterization of oligosaccharides obtained from heparin by the action of heparinase". Biochemistry 11 (4): 563–568. doi:. PMID 5062409.
- ↑ Linhardt RJ, Rice KG. et al. (1988). "Mapping and quantification of the major oligosaccharide components of heparin". Biochem. J. 254 (3): 781–787. PMID 3196292.
- ↑ Shively JE, Conrad HE. (1976). "Formation of anhydrosugars in the chemical depolymerization of heparin". Biochemistry 15 (18): 3932–3942. doi:. PMID 9127.
- ↑ Warda M, Mao W. et al. (2003). "Turkey intestine as a commercial source of heparin? Comparative structural studies of intestinal avian and mammalian glycosaminoglycans.". Comp. Biochem. Physiol. B Biochem. Mol. Biol. 134 (1): 189–197. doi:. PMID 12524047.
- ↑ Ototani N, Kikuchi M, Yosizawa Z. (1981). "Comparative studies on the structures of highly-active and relatively-inactive forms of whale heparin". J Biochem (Tokyo) 90 (1): 241–246. PMID 7287679.
- ↑ Warda M, Gouda EM. et al. (2003). "Isolation and characterization of raw heparin from dromedary intestine: evaluation of a new source of pharmaceutical heparin". Comp. Biochem. Physiol. C Toxicol. Pharmacol. 136 (4): 357–365. doi:. PMID 15012907.
- ↑ Bland CE, Ginsburg H. et al (1982). "Mouse heparin proteoglycan. Synthesis by mast cell-fibroblast monolayers during lymphocyte-dependent mast cell proliferation.". J. Biol. Chem. 257 (15): 8661–8666. PMID 6807978.
- ↑ Linhardt RJ, Ampofo SA. et al (1992). "Isolation and characterization of human heparin". Biochemistry 31 (49): 12441–12445. doi:. PMID 1463730.
- ↑ Hovingh P, Linker A. (1982). "An unusual heparan sulfate isolated from lobsters (Homarus americanus)". J. Biol. Chem. 257 (16): 9840–9844. PMID 6213614.
- ↑ Hovingh P, Linker A. (1993). "Glycosaminoglycans in Anodonta californiensis, a freshwater mussel". Biol. Bull 185 (2): 263–276. doi:. http://www.biolbull.org/cgi/content/abstract/185/2/263.
- ↑ Pejler G, Danielsson A. et al (1987). "Structure and antithrombin-binding properties of heparin isolated from the clams Anomalocardia brasiliana and Tivela mactroides". J. Biol. Chem. 262 (24): 11413–11421. PMID 3624220.
- ↑ Dietrich CP, Paiva JF. et al (1999). "Structural features and anticoagulant activities of a novel natural low-molecular-weight heparin from the shrimp Penaeus brasiliensis". Biochim. Biophys. Acta. 1428 (2–3): 273–283. PMID 10434045.
- ↑ 42.0 42.1 Medeiros GF, Mendes, A. et al (2000). "Distribution of sulfated glycosaminoglycans in the animal kingdom: widespread occurrence of heparin-like compounds in invertebrates". Biochim. Biophys. Acta. 1475 (3): 287–294. PMID 10913828.
- ↑ Chuang W, Christ MD, Peng J, Rabenstein DL. (2000). "An NMR and molecular modeling study of the site-specific binding of histamine by heparin, chemically-modified heparin, and heparin-derived oligosacchrides". Biochemistry. 39: 3542–3555. doi:. PMID 10736153.
- ↑ Alessandri, G. Raju, K. and Gullino, PM. (1983). "Mobilization of capillary endothelium in-vitro induced by effectors of angiogenesis in-vivo". Cancer. Res. 43: 1790–1797. PMID 6187439.
- ↑ Raju, K. Alessandri, G. Ziche, M. and Gullino, PM. (1982). "Ceruloplasmin, copper ions, and angiogenesis". J. Natl. Cancer. Inst. 69: 1183–1188. PMID 6182332.
- ↑ Folkman J. (1985). "Regulation of angiogenesis: a new function of heparin". Biochem. Pharmacol. 34: 905–909. doi:. PMID 2580535.
- ↑ Folkman J. and Ingber DE. (1987). "Angiostatic steroids. Method of discovery and mechanism of action". Ann. Surg. 206 (3): 374–383. doi:. PMID 2443088.
- ↑ Higgins, C. (October 2007). "The use of heparin in preparing samples for blood-gas analysis". Medical Laboratory Observer. http://www.mlo-online.com/articles/1007/1007cover_story.pdf.
- ↑ Yokota M, Tatsumi N, Nathalang O, Yamada T, Tsuda I. (1999). "Effects of Heparin on Polymerase Chain Reaction for Blood White Cells". J. Clin. Lab. Anal. 13: 133–140. doi:. PMID 10323479.
- ↑ AM2 PAT, Inc. Issues Nationwide Recall of Pre-Filled Heparin Lock Flush Solution USP (5 mL in 12 mL Syringes), Am2pat, Inc. Press release, December 20, 2007
- ↑ CBS News, Blood-thinning drug under suspicion
- ↑ FDA informational page with information and links about FDA investigation.
- ↑ Zawisza, Julie (2008-03-29). "FDA Media Briefing on Heparin" (PDF). FDA. Retrieved on 2008-04-23.
- ↑ Nurse committed murders to "test" doctors, Radio Praha, May 12, 2006
- ↑ Ornstein, Charles; Gorman, Anna. (November 21, 2007) Los Angeles Times Report: Dennis Quaid's twins get accidental overdose.
- ↑ Dennis Quaid and wife sue drug maker, USA Today, December 4, 2007
- ↑ Dennis Quaid files suit over drug mishap, Los Angeles Times, December 5, 2007
- ↑ Statement by Dr. Richard Davis, Chief Medical Officer, CHRISTUS Spohn Health System, July 10, 2008
- ↑ At a Glance Heparin Overdose at Hospital, Dallas Morning News, July 11. 2008
- ↑ "Officials Investigate Infants' Heparin OD at Texas Hospital." ABC News. July 11, 2008. Retrieved on July 24, 2008.
External links
|
||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||
|
|||||||||||