Hemorrhoid
| Hemorrhoids Classification and external resources |
|
 |
|
|---|---|
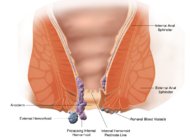
| Schematic demonstrating the anatomy of hemorrhoids. | |
| ICD-10 | I84. |
| ICD-9 | 455 |
| DiseasesDB | 10036 |
| MedlinePlus | 000292 |
| eMedicine | med/2821 emerg/242 |
Hemorrhoids (AmE), haemorrhoids (BrE), emerods, or piles are swelling and inflammation of veins in the rectum and anus. The anatomical term "hemorrhoids" technically refers to "'Cushions of tissue filled with blood vessels at the junction of the rectum and the anus."[1] However, the term is popularly used to refer to varicosities of the hemorrhoid tissue. Perianal hematoma are sometimes misdiagnosed and mislabeled as hemorrhoids, when in fact they have different causes and treatments.[2]
Contents |
Causes
Increased straining during bowel movements, by constipation or diarrhea, may lead to hemorrhoids.[3] It is thus a common condition due to constipation caused by water retention in women experiencing premenstrual syndrome or menstruation.
Hypertension, particularly portal hypertension, can also cause hemorrhoids because of the connections between the portal vein and the vena cava which occur in the rectal wall -- known as portocaval anastomoses.[4]
Obesity can be a factor by increasing rectal vein pressure. Sitting for prolonged periods of time can cause hemorrhoids. Poor muscle tone or poor posture can result in too much pressure on the rectal veins.
Pregnancy causes hypertension and increases strain during bowel movements, so hemorrhoids are often associated with pregnancy.
Excessive consumption of alcohol or caffeine can cause hemorrhoids.[5] Both can cause diarrhea. Note that caffeine ingestion increases blood pressure transiently, but is not thought to cause chronic hypertension. Alcohol can also cause alcoholic liver disease leading to portal hypertension.
Symptoms
Many anorectal problems, including fissures, fistulae, abscesses, or irritation and itching, also called pruritus ani, have similar symptoms and are incorrectly referred to as hemorrhoids.
Hemorrhoids usually are not dangerous or life threatening. In most cases, hemorrhoidal symptoms will go away within a few days.
Although many people have hemorrhoids, not all experience symptoms. The most common symptom of internal hemorrhoids is bright red blood covering the stool, on toilet paper, or in the toilet bowl. However, an internal hemorrhoid may protrude through the anus outside the body, becoming irritated and painful. This is known as a protruding hemorrhoid.
Symptoms of external hemorrhoids may include painful swelling or a hard lump around the anus that results when a blood clot forms. This condition is known as a thrombosed external hemorrhoid.
In addition, excessive straining, rubbing, or cleaning around the anus may cause irritation with bleeding and/or itching, which may produce a vicious cycle of symptoms. Draining mucus may also cause itching.
Food
Insufficient liquid can cause a hard stool, or even chronic constipation, which can lead to hemorrhoidal irritation. An excess of lactic acid in the stool, a product of excessive consumption of dairy products such as cheese, can cause irritation; reducing such consumption can bring relief. Vitamin E deficiency is also a common cause.
Eating fruit helps avoid conditions that lead to hemorrhoids.
Food considered "probiotic", such as yogurt with active culture, may help keep the gut functioning normally and thus prevent flare-ups.
Types of hemorrhoids

- (I84.3-I84.5) External hemorrhoids are those that occur outside of the anal verge (the distal end of the anal canal). Specifically they are varicosities of the inferior rectal arteries, a branch off of the pudendal artery. They are sometimes painful, and can be accompanied by swelling and irritation. Itching, although often thought to be a symptom from external hemorrhoids, is more commonly due to skin irritation.
- (I84.3) External hemorrhoids are prone to thrombosis: if the vein ruptures and a blood clot develops, the hemorrhoid becomes a thrombosed hemorrhoid.[6]
- (I84.0-I84.2) Internal hemorrhoids are those that occur inside the rectum. Specifically they are varicosities of branches off of the superior rectal arteries. As this area lacks pain receptors, internal hemorrhoids are usually not painful and most people are not aware that they have them. Internal hemorrhoids, however, may bleed when irritated.
- (I84.1) Untreated internal hemorrhoids can lead to two severe forms of hemorrhoids: prolapsed and strangulated hemorrhoids:
- Prolapsed hemorrhoids are internal hemorrhoids that are so distended that they are pushed outside the anus.
- If the anal sphincter muscle goes into spasm and traps a prolapsed hemorrhoid outside the anal opening, the supply of blood is cut off, and the hemorrhoid becomes a strangulated hemorrhoid.
By degree of prolapse
The most common grading system was developed by Banov:[7][8]
- Grading of Internal Hemorrhoids
- Grade I: The hemorrhoids do not prolapse.
- Grade II: The hemorrhoids prolapse upon defecation but spontaneously reduce.
- Grade III: The hemorrhoids prolapse upon defecation, but must be manually reduced.
- Grade IV: The hemorrhoids are prolapsed and cannot be manually reduced.
Prevention
Prevention of hemorrhoids includes drinking more fluids, eating more dietary fiber (such as fruits, vegetables and cereals high in fiber), exercising, practicing better posture, and reducing bowel movement strain and time. Hemorrhoid sufferers should avoid using laxatives and should strictly limit time straining during bowel movement. Wearing tight clothing and underwear will also contribute to irritation and poor muscle tone in the region and promote hemorrhoid development. Some sufferers report a more comfortable experience without underwear or wearing only very lightweight underwear.
Women who notice they have painful stools around the time of menstruation would be well-advised to begin taking extra dietary fiber and fluids a couple days prior to that time.
Fluids emitted by the intestinal tract may contain irritants that may increase the fissures associated with hemorrhoids. Washing the anus with cool water and soap may reduce the swelling and increase blood supply for quicker healing and may remove irritating fluid.
Kegel exercises for the pelvic floor may also prove helpful.
Many people do not get a sufficient supply of dietary fiber (20 to 25 grams daily) and small changes in a person's daily diet can help tremendously in both prevention and treatment of hemorrhoids.
Use of squat toilets
Based on their very low incidence in the developing world, where people squat for bodily functions, hemorrhoids have been attributed to the use of the unnatural "sitting" toilet.[9][10] In 1987, an Israeli physician, Dr. Berko Sikirov, published a study testing this hypothesis by having hemorrhoid sufferers convert to squat toilets.[11] Eighteen of the 20 patients were completely relieved of their symptoms (pain and bleeding) with no recurrence, even 30 months after completion of the study. This chart summarizes the results.
{kind=link}
No follow-up studies have ever been published. The American Society of Colon & Rectal Surgeons is silent regarding the therapeutic value of squatting.
Examination

After visual examination of the anus and surrounding area for external or prolapsed hemorrhoids, a doctor would conduct a digital examination. In addition to probing for hemorrhoidal bulges, a doctor would also look for indications of rectal tumor or polyp, enlarged prostate and abscesses.
Visual confirmation of hemorrhoids can be done by doing an anoscopy, using a medical device called an anoscope. This device is basically a hollow tube with a light attached at one end that allows the doctor to see the internal hemorrhoids, as well as polyps in the rectum.
If warranted, more detailed examinations, such as sigmoidoscopy and colonoscopy can be performed. In sigmoidoscopy, the last 60cm of the colon and rectum are examined whereas in colonoscopy the entire bowel is examined.
A pathologist will look for dilated vascular spaces which exhibit thrombosis and recanalization.
Treatments
Treatments for hemorrhoids vary in their cost, risk, and effectiveness. Different cultures and individuals approach treatment differently. Some of the treatments used are listed here in increasing order of intrusiveness and cost.
For many people, hemorrhoids are mild and temporary conditions that heal spontaneously or by the same measures recommended for prevention. There is no medicine that will cure hemorrhoids but local treatments such as warm sitz baths, using a bidet, extendable showerhead, cold compress, or topical analgesic (such as Nupercainal), can also provide temporary relief.
Especially in the case of external hemorrhoids with a visible lump of small size, the condition can be improved with warm bath causing the vessels around rectal region to be relaxed. Consistent use of medicated creams during the early stages of a hemorrhoid flare-up will also provide relief and may stave off further development and irritation. However, creams containing steroid preparations weaken the skin and may contribute to further flare-ups. Keep the area clean and dry, with some lubrication provided by hemorrhoidal creams or a lubricant. Ointment or suppositories such as Proctosedyl[12][13] and Faktu[14] can also relieve the symptoms.
Natural treatments
Some people claim to have successfully applied natural procedures for treatment or reversal of chronic conditions. These procedures largely echo the prevention measures. However, self-care measures, including herbal or "natural" remedies, should not be undertaken without medical consent to avoid possible drug interactions. They include:
- Reducing regional pressure in such ways as improving posture and muscle tone, or in severe cases, undergoing a profound psychophysical reeducation, by a method such as the Alexander Technique.
- Taking herbs and dietary supplements that strengthen vein walls, such as Butcher's Broom, Horse-chestnut, bromelain, and Japanese Pagoda Tree extracts. Drinking 99% pure aloe juice can also relieve itching and swelling.
- Topical application of natural astringents and soothing agents, such as Witch hazel (astringent), Cranesbill, Aloe vera, and honey.
- Drinking chamomile tea several times a day.
- Eating fiber-rich bulking agents such as plantain and Psyllium seed husks to help create a softer stool that is easier to pass, to lessen the irritation of existing hemorrhoids.
- Using the squatting position for bowel movements.[15]
- For sufferers of hemorrhoids caused by poor vein circulation (coupled with varicose veins in lower extremities and/or varicocele), sleeping overnight with raised legs helps reduce or completely eliminate especially external hemorrhoids.
- Using a hand held shower massage to direct a pulsating stream of cold water at external hemorrhoidal tissue for a few minutes each day tends to shrink the swelling, stop the itch and over time may reduce or eliminate the condition. Pressure used must be low at first but should be increased over time during future applications as tolerance builds.
The combination of internal and external remedies is particularly recommended, e.g., Witch-hazel suppositories combined with frequent cups of strong chamomile tea.[16]
Dietary supplements can help treat and prevent many complications of hemorrhoids, and natural botanicals such as Butchers Broom, Horse-chestnut, and bioflavonoids can be an effective addition to hemorrhoid treatment.[17]
Butcher's Broom extract, or Ruscus aculeatus, contains ruscogenins that have anti-inflammatory and vasoconstrictor effects that help tighten and strengthen veins. Butcher's Broom has traditionally been used to treat venous problems including hemorrhoids and varicose veins.[18][19][20]
Horse-chestnut extract, or Aesculus hippocastanum, contains a saponin known as aescin, that has anti-inflammatory, anti-edema, and venotonic actions. Aescin improves tone in vein walls, thereby strengthening the support structure of the vein. Double blind studies have shown that supplementation with Horse-chestnut helps relieve the pain and swelling associated with chronic venous insufficiency.[21][22]
Bilberry extract, or Vaccinium myrtillus, is an anthocyanoside bioflavonoid. Supplementation with this potent flavonoid protects and maintains venous strength and function.[18][23]
Surgical and non-medicinal treatments
Some people require the following medical treatments for chronic or severe hemorrhoids:
- Rubber band ligation
Sometimes called Baron ligation. Elastic bands are applied onto an internal hemorrhoid to cut off its blood supply.[24] Within several days, the withered hemorrhoid is sloughed off during normal bowel movement. - Hemorrhoidolysis/Galvanic Electrotherapy
Desiccation of the hemorrhoid by electrical current. - Sclerotherapy (injection therapy)
Sclerosant or hardening agent is injected into hemorrhoids. This causes the vein walls to collapse and the hemorrhoids to shrivel up. - Cryosurgery
A frozen tip of a cryoprobe is used to destroy hemorrhoidal tissues.[25] Rarely used anymore because of side effects. - Laser, infrared or BICAP coagulation
Laser, infrared beam, or electricity is used to cauterize the affected tissues. Lasers are now much less popular. Infrared coagulation has been studied in comparison with RBL and found to be as effective in hemorrhoids up to grade III. These are the most readily available non-surgical procedures in the US. - Hemorrhoidectomy
A true surgical procedure to excise and remove hemorrhoids. Has possible correlation with incontinence issues later in life; in addition, many patients complain that pain during recovery is severe. For this reason is often now recommended only for severe (grade IV) hemorrhoids. - Stapled Hemorrhoidectomy
Also called the procedure for prolapse and hemorrhoids, it is designed to resect soft tissue proximal to the dentate line, which disrupts the blood flow to the hemorrhoids. It is generally less painful than complete removal of hemorrhoids and also allows for faster recovery times. It's meant for hemorrhoids that fall out or bleed and is not helpful for painful outside conditions. - Enema
This practice is used to clean the rectum. While it is a simple procedure, it can be complicated by hemorrhoids, so in such cases, it should be done by a doctor. In an enema, water is injected into the rectum and then flushed out, cleaning the area. - Doppler Guided Hemorrhoidal Artery Ligation
The only evidence-based surgery for all grades of hemorrhoids. It does not involve cutting tissues or even a stay at the hospital; patients are usually back to work on the same day. It is the best treatment for bleeding piles, as the bleeding stops immediately. [26] - HAL-RAR
To date, Doppler Guided Hemorrhoidal Artery Ligation was indicated in management of Grade II & Grade III Hemorrhoids but with the availability of HAL Recto Anal Repair Management of prolapsing hemorrhoids without excision is also possible. - Transanal hemorrhoidal dearterialization (THD)
Similar to HAL, but more standardizable and therefore safer, less painful and has a shorter recovery time.
- Radiofrequency Coagulation
Diseases with similar symptoms
Symptoms associated with rectal cancer, anal fissure, anal abscess, anal fistula, Perianal hematoma, and other diseases may be similar to those produced by hemorrhoids and may be reduced by the topical analgesic methods described above. For this reason, it is a good idea to consult with a physician when these symptoms are encountered, particularly for the first time, and periodically should the problem continue. In the US, colonoscopy is recommended as a general diagnostic for those over age 50 (40 with family history of bowel cancers); a clear (normal) scope is good for 10 years.
References
- ↑ MedlinePlus Medical Encyclopedia:Hemorrhoid surgery - series: Normal anatomy
- ↑ Perianal hematoma - Medbroadcast
- ↑ Harms R (November 3, 2007). "Hemorrhoids during pregnancy: Treatment options". MayoClinic. Retrieved on 2007-11-28.
- ↑ "Causes of Hemorrhoids". Mayo Clinic (November 28, 2006). Retrieved on 2007-12-07.
- ↑ Burney RE (November 2005). "Hemorrhoids". University of Michigan Health System. Retrieved on 2007-11-28.
- ↑ E. Gojlan, Pathology, 2nd ed. Mosby Elsevier, Rapid Review series.
- ↑ Hemorrhoid at eMedicine
- ↑ Banov L, Knoepp LF, Erdman LH, Alia RT (1985). "Management of hemorrhoidal disease". J S C Med Assoc 81 (7): 398–401. PMID 3861909.
- ↑ Sikirov BA (1989). "Primary constipation: an underlying mechanism". Med. Hypotheses 28 (2): 71–3. doi:. PMID 2927355.
- ↑ Sikirov D (2003). "Comparison of straining during defecation in three positions: results and implications for human health". Dig. Dis. Sci. 48 (7): 1201–5. doi:. PMID 12870773.
- ↑ Sikirov BA (1987). "Management of hemorrhoids: a new approach". Isr. J. Med. Sci. 23 (4): 284–6. PMID 3623887.
- ↑ Proctosedyl ointment/suppositories
- ↑ Proctosedyl - Drugs - Medbroadcast
- ↑ http://www.vghks.gov.tw/ph/%E8%99%95%E6%96%B9%E9%9B%86/drug/faktu.htm
- ↑ Christine Dimmer, Brian Martin, Noeline Reeves and Frances Sullivan (October 1996). "Squatting for the Prevention of Hemorrhoids". Townsend Letter for Doctors & Patients (159): 66–70. http://www.uow.edu.au/arts/sts/bmartin/pubs/96tldp.html.
- ↑ K. Kraft and C. Hobbs, Pocket Guide to Herbal Medicine. New York: Thieme.
- ↑ MacKay D (2001). "Hemorrhoids and varicose veins: a review of treatment options" (PDF). Altern Med Rev 6 (2): 126–40. PMID 11302778. http://www.thorne.com/altmedrev/.fulltext/6/2/126.pdf.
- ↑ 18.0 18.1 Pizzorno JE and Murray MT, eds., ed. (1998). Encyclopedia of Natural Medicine (revised 2nd edition ed.). CA: Prima Publishing. pp. 829.
- ↑ Rudofsky G (1989). "[Improving venous tone and capillary sealing. Effect of a combination of Ruscus extract and hesperidine methyl chalcone in healthy probands in heat stress]" (in German). Fortschr. Med. 107 (19): 52, 55–8. PMID 2668140.
- ↑ Cappelli R, Nicora M, Di Perri T (1988). "Use of extract of Ruscus aculeatus in venous disease in the lower limbs". Drugs Exp Clin Res 14 (4): 277–83. PMID 3048951.
- ↑ Pittler MH, Ernst E (1998). "Horse-chestnut seed extract for chronic venous insufficiency. A criteria-based systematic review". Arch Dermatol 134 (11): 1356–60. doi:. PMID 9828868.
- ↑ Diehm C, Trampisch HJ, Lange S, Schmidt C (1996). "Comparison of leg compression stocking and oral Horse-chestnut seed extract therapy in patients with chronic venous insufficiency". Lancet 347 (8997): 292–4. doi:. PMID 8569363.
- ↑ Murray MT. (1996). Encyclopedia of Nutritional Supplements. NY: Three Rivers Press. pp. 326.
- ↑ Longman RJ, Thomson WH (2006). "A prospective study of outcome from rubber band ligation of piles". Colorectal Dis 8 (2): 145–8. doi:. PMID 16412076.
- ↑ MacLeod JH (1982). "In defense of cryotherapy for hemorrhoids. A modified method". Dis. Colon Rectum 25 (4): 332–5. PMID 6979469.
- ↑ Scheyer M, Antonietti E, Rollinger G, Mall H, Arnold S (2006). "Doppler-guided hemorrhoidal artery ligation". Am. J. Surg. 191 (1): 89–93. doi:. PMID 16399113.
See also
- Anal fissure
- Anal fistula
- Perianal hematoma
- Proctoscopy
- Anal abscess
External links
- Hemorrhoid at the Open Directory Project
|
|||||||||||||||||||||||||||||||||||||||||