Epilepsy
| Epilepsy Classification and external resources |
|
| ICD-10 | G40.-G41. |
|---|---|
| ICD-9 | 345 |
| DiseasesDB | 4366 |
| MedlinePlus | 000694 |
| eMedicine | neuro/415 |
| MeSH | D004827 |
Epilepsy is a common chronic neurological disorder that is characterized by recurrent unprovoked seizures.[1][2] These seizures are transient signs and/or symptoms due to abnormal, excessive or synchronous neuronal activity in the brain.[3] About 50 million people worldwide have epilepsy at any one time.[4] Epilepsy is usually controlled, but not cured, with medication, although surgery may be considered in difficult cases. However, over 30% of people with epilepsy do not have seizure control even with the best available medications [5][6]. Not all epilepsy syndromes are lifelong – some forms are confined to particular stages of childhood. Epilepsy should not be understood as a single disorder, but rather as a group of syndromes with vastly divergent symptoms but all involving episodic abnormal electrical activity in the brain.
Contents |
Classification
Epilepsies are classified in five ways:
- By their first cause (or etiology).
- By the observable manifestations of the seizures, known as semiology.
- By the location in the brain where the seizures originate.
- As a part of discrete, identifiable medical syndromes.
- By the event that triggers the seizures, as in primary reading epilepsy or musicogenic epilepsy.
In 1981, the International League Against Epilepsy (ILAE) proposed a classification scheme for individual seizures that remains in common use.[7] This classification is based on observation (clinical and EEG) rather than the underlying pathophysiology or anatomy and is outlined later on in this article. In 1989, the ILAE proposed a classification scheme for epilepsies and epileptic syndromes.[8] This can be broadly described as a two-axis scheme having the cause on one axis and the extent of localisation within the brain on the other. Since 1997, the ILAE have been working on a new scheme that has five axes: ictal phenomenon, seizure type, syndrome, etiology and impairment.[9]
Diagnosis
The diagnosis of epilepsy requires the presence of recurrent, unprovoked seizures; accordingly, it is usually made based on the medical history. Imaging and measurement technologies such as electroencephalography (EEG), magnetic resonance imaging (MRI), single photon emission computed tomography (SPECT), positron emission tomography (PET), and magnetoencephalography (MEG) may be useful to discover an etiology for the epilepsy, discover the affected brain region, or classify the epileptic syndrome, but these studies are not useful in making the initial diagnosis.
Long-term video-EEG monitoring for epilepsy is the gold standard for diagnosis, but it is not routinely employed owing to its high cost, low availability and inconvenience.
Convulsive or other seizure-like activity, non-epileptic in origin, can be observed in many other medical conditions. These non-epileptic seizures can be hard to differentiate and may lead to misdiagnosis.
Epilepsy covers conditions with different etiologies, natural histories and prognoses, each requiring different management strategies. A full medical diagnosis requires a definite categorization of seizure and syndrome types.[10]
Many people are misdiagnosed, because doctors unfamiliar with the symptoms believe that their patients have another illness, because they are not adequately trained to recognize the early symptoms including odd tastes or smells. Approximately 80% have petit mal seizures which are harder to spot[11].
Precipitants
The diagnosis of epilepsy usually requires that the seizures occur spontaneously. Nevertheless, certain epilepsy syndromes require particular precipitants or triggers for seizures to occur. These are termed reflex epilepsy. For example, patients with primary reading epilepsy have seizures triggered by reading. Photosensitive epilepsy can be limited to seizures triggered by flashing lights. Other precipitants can trigger an epileptic seizure in patients who otherwise would be susceptible to spontaneous seizures. For example, children with childhood absence epilepsy may be susceptible to hyperventilation. In fact, flashing lights and hyperventilation are activating procedures used in clinical EEG to help trigger seizures to aid diagnosis. Finally, other precipitants can facilitate, rather than obligately trigger, seizures in susceptible individuals. Emotional stress, sleep deprivation, sleep itself, and febrile illness are examples of precipitants cited by patients with epilepsy. Notably, the influence of various precipitants varies with the epilepsy syndrome. [12]. Likewise, the menstrual cycle in women with epilepsy can influence patterns of seizure recurrence. Catamenial epilepsy is the term denoting seizures linked to the menstrual cycle.[13]
Epidemiology
Epilepsy is one of the most common of the serious neurological disorders.[14] Genetic, congenital, and developmental conditions are mostly associated with it among younger patients; tumors are more likely over age 40; head trauma and central nervous system infections may occur at any age. The prevalence of active epilepsy is roughly in the range 5–10 per 1000 people. Up to 5% of people experience non febrile seizures at some point in life; epilepsy's lifetime prevalence is relatively high because most patients either stop having seizures or (less commonly) die of it. Epilepsy's approximate annual incidence rate is 40–70 per 100,000 in industrialized countries and 100–190 per 100,000 in resource-poor countries; socioeconomically deprived people are at higher risk. In industrialized countries the incidence rate decreased in children but increased among the elderly during the three decades prior to 2003, for reasons not fully understood.[15]
Beyond symptoms of the underlying diseases that can cause certain epilepsies, people with epilepsy are at risk for death from four main problems: status epilepticus (most often associated with anticonvulsant noncompliance), suicide associated with depression, trauma from seizures, and sudden unexpected death in epilepsy (SUDEP) [16][17][18] Those at highest risk for epilepsy-related deaths usually have underlying neurological impairment or poorly controlled seizures; those with more benign epilepsy syndromes have little risk for epilepsy-related death.
Certain diseases also seem to occur in higher than expected rates in people with epilepsy, and the risk of these "comorbities" often varies with the epilepsy syndrome. These diseases include depression and anxiety disorders, migraine and other headaches, infertility and low sexual libido. Attention-deficit/hyperactivity disorder (ADHD) affects three to five times more children with epilepsy than children in the general population. [19] Epilepsy is prevalent in autism. [20]
Seizure types
Seizure types are organized firstly according to whether the source of the seizure within the brain is localized (partial or focal onset seizures) or distributed (generalized seizures). Partial seizures are further divided on the extent to which consciousness is affected. If it is unaffected, then it is a simple partial seizure; otherwise it is a complex partial (psychomotor) seizure. A partial seizure may spread within the brain - a process known as secondary generalization. Generalized seizures are divided according to the effect on the body but all involve loss of consciousness. These include absence (petit mal), myoclonic, clonic, tonic, tonic-clonic (grand mal) and atonic seizures.
Epilepsy syndromes
There are many different epilepsy syndromes, each presenting with its own unique combination of seizure type, typical age of onset, EEG findings, treatment, and prognosis. The most widespread classification of the epilepsies [8] divides epilepsy syndromes by location or distribution of seizures (as revealed by the appearance of the seizures and by EEG) and by cause. Syndromes are divided into localization-related epilepsies, generalized epilepsies, or epilepsies of unknown localization.
Localization-related epilepsies, sometimes termed partial or focal epilepsies, arise from an epileptic focus, a small portion of the brain that serves as the irritant driving the epileptic response. Generalized epilepsies, in contrast, arise from many independent foci (multifocal epilepsies) or from epileptic circuits that involve the whole brain. Epilepsies of unknown localization remain unclear whether they arise from a portion of the brain or from more widespread circuits.
Epilepsy syndromes are further divided by presumptive cause: idiopathic, symptomatic, and cryptogenic. Idiopathic epilepsies are generally thought to arise from genetic abnormalities that lead to alteration of basic neuronal regulation. Symptomatic epilepsies arise from the effects of an epileptic lesion, whether that lesion is focal, such as a tumor, or a defect in metabolism causing widespread injury to the brain. Cryptogenic epilepsies involve a presumptive lesion that is otherwise difficult or impossible to uncover during evaluation.
Some epileptic syndromes are difficult to fit within this classification scheme and fall in the unknown localization/etiology category. People who only have had a single seizure, or those with seizures that occur only after specific precipitants ("provoked seizures"), have "epilepsies" that fall into this category. Febrile convulsions are an example of seizures bound to a particular precipitant. Landau-Kleffner syndrome is another epilepsy which, because of its variety of EEG distributions, falls uneasily in clear categories. More confusingly, certain syndromes like West syndrome featuring seizures such as Infantile spasms can be classified as idiopathic, syndromic, or cryptogenic depending on cause and can arise from both focal or generalized epileptic lesions.
Below are some common seizure syndromes:
- Benign centrotemporal lobe epilepsy of childhood or Benign rolandic epilepsy is an idiopathic localization-related epilepsy that occurs in children between the ages of 3 and 13 years with peak onset in prepubertal late childhood. Apart from their seizure disorder, these patients are otherwise normal. This syndrome features simple partial seizures that involve facial muscles and frequently cause drooling. Although most episodes are brief, seizures sometimes spread and generalize. Seizures are typically nocturnal and confined to sleep. The EEG may demonstrate spike discharges that occur over the centrotemporal scalp over the central sulcus of the brain (the Rolandic sulcus) that are predisposed to occur during drowsiness or light sleep. Seizures cease near puberty. [21] Seizures may require anticonvulsant treatment, but sometimes are infrequent enough to allow physicians to defer treatment.
- Benign occipital epilepsy of childhood (BOEC) is an idiopathic localization-related epilepsy and consists of an evolving group of syndromes. Most authorities include two subtypes, an early subtype with onset between 3-5 years and an late onset between 7-10 years. Seizures in BOEC usually feature visual symptoms such as scotoma or fortifications (brightly colored spots or lines) or amaurosis (blindness or impairment of vision). Convulsions involving one half the body, hemiconvulsions, or forced eye deviation or head turning are common. Younger patients typically experience symptoms similar to migraine with nausea and headache, and older patients typically complain of more visual symptoms. The EEG in BOEC shows spikes recorded from the occipital (back of head) regions. Lately, a group of epilepsies termed Panayiotopoulos syndrome[22] that share some clinical features of BOEC but have a wider variety of EEG findings are classified by some as BOEC.
- Autosomal dominant nocturnal frontal lobe epilepsy (ADNFLE) is an idiopathic localization-related epilepsy that is an inheirited epileptic disorder that causes seizures during sleep. Onset is usually in childhood. These seizures arise from the frontal lobes and consist of complex motor movements, such as hand clenching, arm raising/lowering, and knee bending. Vocalizations such as shouting, moaning, or crying are also common. ADNFLE is often misdiagnosed as nightmares. ADNFLE has a genetic basis[23]. These genes encode various nicotinic acetylcholine receptors.
- Primary reading epilepsy is a reflex epilepsy classified as an idiopathic localization-related epilepsy. Reading in susceptible individuals triggers characteristic seizures[24].
- Childhood absence epilepsy (CEA) is an idiopathic generalized epilepsy that affects children between the ages of 4 and 12 years of age, although peak onset is around 5-6 years old. These patients have recurrent absence seizures, brief episodes of unresponsive staring, sometimes with minor motor features such as eye blinking or subtle chewing. The EEG finding in CAE is generalized 3 Hz spike and wave discharges. Some go on to develop generalized tonic-clonic seizures. This condition carries a good prognosis because children do not usually show cognitive decline or neurological deficits, and the seizures in the majority cease spontaneously with onging maturation.
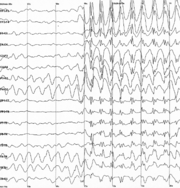 Generalized 3 Hz spike and wave discharges in EEG
Generalized 3 Hz spike and wave discharges in EEG
- Juvenile absence epilepsy is an idiopathic generalized epilepsy with later onset that CAE, typically in prepubertal adolescence, with the most frequent seizure type being absence seizures. Generalized tonic-clonic seizures can occur. 3 Hz spike-wave or multiple spike discharges can be seen on EEG. Prognosis is mixed, with some patients going on to a syndrome that is poorly distinguishable from JME.
- Juvenile myoclonic epilepsy (JME) is an idiopathic generalized epilepsy that occurs in patients aged 8 to 20 years. Patients have normal cognition and are otherwise neurologically intact. The most common seizures are myoclonic jerks, although generalized tonic-clonic seizures and absence seizures may occur as well. Myoclonic jerks usually cluster in the early morning after awakening. The EEG reveals generalized 4-6 Hz spike wave discharges or multiple spike discharges. Interestingly, these patients are often first diagnosed when they have their first generalized tonic-clonic seizure later in life when they experience sleep deprivation (e.g., freshman year in college after staying up late to study for exams). Alcohol withdrawal can also be a major contributing factor in breakthrough seizures as well. The risk of the tendency to have seizures is lifelong; however, the majority have well-controlled seizures with anticonvulsant medication and avoidance of seizure precipitants.
- Symptomatic localization-related epilepsies Symptomatic localization-related epilepsies are divided by the location in the brain of the epileptic lesion, since the symptoms of the seizures are more closely tied to the brain location rather than the cause of the lesion. Tumors, atriovenous malformations, cavernous malformations, trauma, and cerebral infarcts can all be causes of epileptic foci in different brain regions.
- Temporal lobe epilepsy (TLE), a symptomatic localization-related epilepsy, is the most common epilepsy of adults who experience seizures poorly controlled with anticonvulsant medications. In most cases, the epileptogenic region is found in the midline (mesial) temporal structures (e.g., the hippocampus, amygdala, and parahippocampal gyrus). Seizures begin in late childhood and adolescence. Most of these patients have complex partial seizures sometimes preceded by an aura, and some TLE patients also suffer from secondary generalized tonic-clonic seizures. If the patient does not respond sufficiently to medical treatment, epilepsy surgery may be considered.
- Frontal lobe epilepsy, usually a symptomatic or cryptogenic localization-related epilepsy, arises from lesions causing seizures that occur in the frontal lobes of the brain. These epilepsies can be difficult to diagnose because the symptoms of seizures can easily be confused with nonepileptic spells and, because of limitations of the EEG, be difficult to "see" with standard scalp EEG.
- Rasmussen's encephalitis is a symptomatic localization-related epilepsy that is a progressive, inflammatory lesion affecting children with onset before the age of 10. Seizures start as separate simple partial or complex partial seizures and may progress to epilepsia partialis continuata (simple partial status epilepticus). Neuroimaging shows inflammatory encephalitis on one side of the brain that may spread if not treated. Dementia and hemiparesis are other problems. The cause is hypothesized to involve an immulogical attack against glutamate receptors, a common neurotransmitter in the brain. [25]
- West syndrome is a triad of developmental delay, seizures termed infantile spasms, and EEG demonstrating a pattern termed hypsarrhythmia. Onset occurs between 3 months and 2 years, with peak onset between 8-9 months. West syndrome may arise from idiopathic, symptomatic, or cryptogenic causes. The most common cause is tuberous sclerosis. The prognosis varies with the underlying cause. In general most surviving patients remain with significant cognitive impairment and continuing seizures and may evolve to another eponymic syndrome, Lennox-Gastaut syndrome.
- Dravet's syndrome Severe myoclonic epilepsy of infancy (SMEI). This generalized epilepsy syndrome is distinguished from benign myoclonic epilepsy by its severity and must be differentiated from the Lennox-Gastaut syndrome and Doose’s myoclonic-astatic epilepsy. Onset is in the first year of life and symptoms peak at about 5 months of age with febrile hemiclonic or generalized status epilepticus. Boys are twice as often affected as girls. Prognosis is poor. Most cases are sporadic. Family history of epilepsy and febrile convulsions is present in around 25 percent of the cases.[26]
- Progressive myoclonic epilepsies define a group of symptomatic generalized epilepsies characterized by progressive dementia and myoclonic seizures. Tonic-clonic seizures may occur as well. Diseases usually classified in this group are Unverricht-Lundborg disease, myoclonus epilepsy with ragged red fibers (MERRF syndrome), Lafora disease, neuronal ceroid lipofucinosis, and sialdosis.
- Lennox-Gastaut syndrome (LGS) is a generalized epilepsy that consists of a triad of developmental delay or childhood dementia, mixed generalized seizures, and EEG demonstrating a pattern of approximately 2 Hz "slow" spike-wave. Onset occurs between 2-18 years. As in West syndrome, LGS result from idiopathic, symptomatic, or cryptogenic causes, and many patients first have West syndrome. Authorities emphasize different seizure types as important in LGS, but most have astatic seizures (drop attacks), tonic seizures, tonic-clonic seizures, atypical absence seizures, and sometimes, complex partial seizures. Anticonvulsants are usually only partially successful in treatment.
Treatment
Epilepsy is usually treated with medication prescribed by a physician; primary caregivers, neurologists, and neurosurgeons all frequently care for people with epilepsy. In some cases the implantation of a stimulator of the vagus nerve, or a special diet can be helpful. Neurosurgical operations for epilepsy can be palliative, reducing the frequency or severity of seizures; or, in some patients, an operation can be curative.
Responding to a seizure
In most cases, the proper emergency response to a generalized tonic-clonic epileptic seizure is simply to prevent the patient from self-injury by moving him or her away from sharp edges, placing something soft beneath the head, and carefully rolling the person into the recovery position to avoid asphyxiation. In some cases the person may seem to start snoring loudly following a seizure, before coming to. This merely indicates that the person is beginning to breathe properly and does not mean he or she is suffocating. Should the person regurgitate, the material should be allowed to drip out the side of the person's mouth by itself. If a seizure lasts longer than 5 minutes, or if the seizures begin coming in 'waves' one after the other - then Emergency Medical Services should be contacted immediately. Prolonged seizures may develop into status epilepticus, a dangerous condition requiring hospitalization and emergency treatment.
Objects should never be placed in a person's mouth by anybody - including paramedics - during a seizure as this could result in serious injury to either party. Despite common folklore, it is not possible for a person to swallow their own tongue during a seizure. However, it is possible that the person will bite their own tongue, especially if an object is placed in the mouth.
With other types of seizures such as simple partial seizures and complex partial seizures where the person is not convulsing but may be hallucinating, disoriented, distressed, or unconscious, the person should be reassured, gently guided away from danger, and sometimes it may be necessary to protect the person from self-injury, but physical force should be used only as a last resort as this could distress the person even more. In complex partial seizures where the person is unconscious, attempts to rouse the person should not be made as the seizure must take its full course. After a seizure, the person may pass into a deep sleep or otherwise they will be disoriented and often unaware that they have just had a seizure, as amnesia is common with complex partial seizures. The person should remain observed until they have completely recovered, as with a tonic-clonic seizure.
After a seizure, it is typical for a person to be exhausted and confused. Often the person is not immediately aware that they have just had a seizure. During this time one should stay with the person - reassuring and comforting them - until they appear to act as they normally would. Seldom during seizures do people lose bladder or bowel control. In some instances the person may vomit after coming to. People should not eat or drink until they have returned to their normal level of awareness, and they should not be allowed to wander about unsupervised. Many patients will sleep deeply for a few hours after a seizure - this is common for those having just experienced a more violent type of seizure such as a tonic-clonic. In about 50% of people with epilepsy, headaches may occur after a seizure. These headaches share many features with migraines, and respond to the same medications.
It is helpful if those present at the time of a seizure make note of how long and how severe the seizure was. It is also helpful to note any mannerisms displayed during the seizure. For example, the individual may twist the body to the right or left, may blink, might mumble nonsense words, or might pull at clothing. Any observed behaviors, when relayed to a neurologist, may be of help in diagnosing the type of seizure which occurred.
Pharmacologic treatment
The mainstay of treatment of epilepsy is anticonvulsant medications. Often, anticonvulsant medication treatment will be lifelong and can have major effects on quality of life. The choice among anticonvulsants and their effectiveness differs by epilepsy syndrome. Mechanisms, effectiveness for particular epilepsy syndromes, and side effects, of course, differ among the individual anticonvulsant medications. Some general findings about the use of anticonvulsants are outlined below.
History and Availability- The first anticonvulsant was bromide, suggested in 1857 by Charles Locock who used it to treat women with "hysterical epilepsy" (probably catamenial epilepsy). Potassium bromide was also noted to cause impotence in men. Authorities concluded that potassium bromide would dampen sexual excitement thought to cause the seizures, which in fact it did (athough we know now that impotence is a side effect of bromide treatment, not a treatment of epilepsy). Phenobarbital was first used in 1912 for both its sedative and antiepileptic properties. By the 1930s, the development of animal models in epilepsy research lead to the development of phenytoin by Tracy Putnam and H. Houston Merritt, which had the distinct advantage of treating epileptic seizures with less sedation[27]. By the 1970s, an National Institutes of Health initiative, the Anticonvulsant Screening Program, headed by J. Kiffin Penry, served as a mechanism for drawing the interest and abilities of pharmaceutical companies in the development of new anticonvulsant medications.
Currently there are 19 medications approved by the Food and Drug Administration for the use of treatment of epileptic seizures in the US: carbamazepine (common US brand name Tegretol), clorazepate (Tranxene) clonazepam (Klonopin), ethosuximide (Zarontin), felbamate (Felbatol), fosphenytoin (Cerebyx), gabapentin (Neurontin), lamotrigine (Lamictal), levetiracetam (Keppra), oxcarbazepine (Trileptal), phenobarbital (Luminal), phenytoin (Dilantin), pregabalin (Lyrica), primidone (Mysoline), tiagabine (Gabitril), topiramate (Topamax), valproate semisodium (Depakote), valproic acid (Depakene), and zonisamide (Zonegran). Most of these appeared after 1990.
Medications commonly available outside the US but still labelled as "investigational" within the US are clobazam (Frisium) and vigabatrin (Sabril).
Other drugs are commonly used to abort an active seizure or interrupt a seizure flurry; these include diazepam (Valium, Diastat) and lorazepam (Ativan). Drugs used only in the treatment of refractory status epilepticus include paraldehyde (Paral), midazolam (Versed), and pentobarbital (Nembutal).
Some anticonvulsant medications do not have primary FDA-approved uses in epilepsy but are used in limited trials, remain in rare use in difficult cases, have limited "grandfather" status, are bound to particular severe epilepsies, or are under current investigation. These include acetazolamide (Diamox), progesterone, adrenocorticotropic hormone (ACTH, Acthar), various corticotropic steroid hormones (prednisone), or bromide.
Effectiveness - The definition of "effective" varies. FDA-approval usually requires that 50% of the patient treatment group had at least a 50% improvement in the rate of epileptic seizures. About 20% of patients with epilepsy continue to have breakthrough epileptic seizures despite best anticonvulsant treatment. [28][29].
Safety and Side Effects - 88% of patients with epilepsy, in a European survey, reported at least one anticonvulsant related side effect. [30] Most side effects are mild and "dose-related" and can often be avoided or minimized by the use of the smallest effective amount. Some examples include mood changes, sleepiness, or unsteadiness in gait. Some anticonvulsant medications have "idiosyncratic" side-effects that can not be predicted by dose. Some examples include drug rashes, liver toxicity (hepatitis), or aplastic anemia. Safety includes the consideration of tetragenicity (the effects of medications on fetal development) when women with epilepsy become pregnant.
Principles of Anticonvulsant Use and Management - The goal for individual patients is, of course, no seizures and no side effects, and the job of the physician is to aid the patient to find the best balance between the two during the prescribing of anticonvulsants. Most patients can achieve this balance best with monotherapy, the use of a single anticonvulsant medication. Some patients, however, require polypharmacy; the use of two or more anticonvulsants.
Serum levels of AEDs can be checked to determine medication compliance, to assess the effects of new drug-drug interactions upon previous stable medication levels, or to help establish if particular symptoms such as instability or sleepiness can be considered a drug side-effect or are due to different causes. Children or impaired adults who may not be able to communicate side effects may benefit from routine screening of drug levels. Beyond baseline screening, however, trials of recurrent, routine blood or urine monitoring show no proven benefits and may lead to unnecessary medication adjustments in most older children and adults using routine anticonvulsants.[31][32]
If a person's epilepsy cannot be brought under control after adequate trials of two or three (experts vary here) different drugs, that person's epilepsy is generally said to be medically refractory. A study of patients with previously untreated epilepsy demonstrated that 47% achieved control of seizures with the use of their first single drug. 14% became seizure free during treatment with a second or third drug. An additional 3% became seizure-free with the use of two drugs simultaneously.[33] Other treatments, in addition to or instead of, anticonvulsant medications may be considered by those people with continuing seizures.
Surgical treatment
Epilepsy surgery is an option for patients whose seizures remain resistant to treatment with anticonvulsant medications who also have symptomatic localization-related epilepsy; a focal abnormality that can be located and therefore removed. The goal for these procedures is total control of epileptic seizures [34], although anticonvulsant medications may still be required. [35]
The evaluation for epilepsy surgery is designed to locate the "epileptic focus" (the location of the epileptic abnormality) and to determine if resective surgery will affect normal brain function. Physicians will also confirm the diagnosis of epilepsy to make sure that spells arise from epilepsy (as opposed to non-epileptic seizures). The evaluation typically includes neurological examination, routine EEG, Long-term video-EEG monitoring, neuropsychological evaluation, and neuroimaging such as MRI, Single photon emission computed tomography (SPECT), positron emission tomography (PET). Some epilepsy centers use intracarotid sodium amobarbital test (Wada test), functional MRI or Magnetoencephalography (MEG) as supplementary tests.
Certain lesions require Long-term video-EEG monitoring with the use of intracranial electrodes if noninvasive testing was inadequate to identify the epileptic focus or distinguish the surgical target from normal brain tissue and function. Brain mapping by the technique of cortical electrical stimulation or Electrocorticography are other procedures used in the process of invasive testing in some patients.
The most common surgeries are the resection of lesions like tumors or arteriovenous malformations which, in the process of treating the underlying lesion, often result in control of epileptic seizures caused by these lesions.
Other lesions are more subtle and feature epilepsy as the main or sole symptom. The most common form of intractable epilepsy in these disorders in adults is temporal lobe epilepsy with hippocampal sclerosis, and the most common type of epilepsy surgery is the anterior temporal lobectomy, or the removal of the front portion of the temporal lobe including the amygdala and hippocampus. Some neurosurgeons recommend selective amygdalahippocampectomy because of possible benefits in postoperative memory or language function. Surgery for temporal lobe epilepsy is effective, durable, and results in decreased health care costs. [36][37]. Despite the efficacy of epilepsy surgery, some patients decide not to undergo surgery owing to fear or the uncertainty of having a brain operation.
Palliative surgery for epilepsy is intended to reduce the frequency or severity of seizures. Examples are callosotomy or commissurotomy to prevent seizures from generalizing (spreading to involve the entire brain), which results in a loss of consciousness. This procedure can therefore prevent injury due to the person falling to the ground after losing consciousness. It is performed only when the seizures cannot be controlled by other means. Multiple subpial transection can also be used to decrease the spread of seizures across the cortex especially when the epileptic focus is located near important functional areas of the cortex. Resective surgery can be considered palliative if it is undertaken with the expectation that it will reduce but not eliminate seizures.
Hemispherectomy involves removal or a functional disconnection of most or all of one half of the cerebrum. It is reserved for people suffering from the most catastrophic epilepsies, such as those due to Rasmussen syndrome. If the surgery is performed on very young patients (2-5 years old), the remaining hemisphere may acquire some rudimentary motor control of the ipsilateral body; in older patients, paralysis results on the side of the body opposite to the part of the brain that was removed. Because of these and other side effects it is usually reserved for patients who have exhausted other treatment options.
Other treatment
Ketogenic diet- a high fat, low carbohydrate diet developed in the 1920s, largely forgotten with the advent of effective anticonvulsants, and resurrected in the 1990s. The mechanism of action is unknown. It is used mainly in the treatment of children with severe, medically-intractable epilepsies.
Electrical stimulation [38]- methods of anticonvulsant treatment with both currently approved and investigational uses. A currently approved device is vagus nerve stimulation (VNS). Investigational devices include the responsive neurostimulation system and deep brain stimulation.
Vagus nerve stimulation (VNS)- The VNS (US manufacturer = Cyberonics) consists of a computerized electrical device similar in size, shape and implant location to a heart pacemaker that connects to the vagus nerve in the neck. The device stimulates the vagus nerve at pre-set intervals and intensities of current. Efficacy has been tested in patients with localization-related epilepsies demonstrating that 50% of patients experience a 50% improvement in seizure rate. Case series have demonstrated similar efficacies in certain generalized epilepsies such as Lennox-Gastaut syndrome. Although success rates are not usually equal to that of epilepsy surgery, it is a reasonable alternative when the patient is reluctant to proceed with any required invasive monitoring, when appropriate presurgical evaluation fails to uncover the location of epileptic foci, or when there are multiple epileptic foci.
Responsive Neurostimulator System (RNS) (US manufacturer Neuropace) consists of an computerized electrical device implanted in the skull with electrodes implanted in presumed epileptic foci within the brain. The brain electrodes send EEG signal to the device which contains seizure-detection software. When certain EEG seizure criteria are met, the device delivers a small electrical charge to other electrodes near the epileptic focus and disrupt the seizure. The efficacy of the RNS is under current investigation with the goal of FDA approval.
Deep brain stimulation (DBS) (US manufacturer Medtronics) consists of computerized electrical device implanted in the chest in a manner similar to the VNS, but electrical stimulation is delivered to deep brain structures through depth electrodes implanted through the skull. In epilepsy, the electrode target is the anterior nucleus of the thalamus. The efficacy of the DBS in localization-related epilepsies is currently under investigation.
Noninvasive surgery- The use of the Gamma Knife or other devices used in radiosurgery are currently being investigated as alternatives to traditional open surgery in patients who would otherwise qualify for anterior temporal lobectomy[39]
Avoidance therapy- Avoidance therapy consists of minimizing or eliminating triggers in patients whose seizures are particularly susceptible to seizure precipitants (see above). For example, sunglasses that counter exposure to particular light wavelengths can improve seizure control in certain photosensitive epilepsies[40]
Warning systems- A seizure response dog is a form of service dog that is trained to summon help or ensure personal safety when a seizure occurs. These are not suitable for everybody and not all dogs can be so trained. Rarely, a dog may develop the ability to sense a seizure before it occurs.[41]. Development of electronic forms of seizure detection systems are currently under investigation.
Alternative or complementary medicine- A number of systematic reviews by the Cochrane Collaboration into treatments for epilepsy looked at acupuncture,[42] psychological interventions,[43] vitamins[44] and yoga[45] and found there is no reliable evidence to support the use of these as treatments for epilepsy.
Pathophysiology
Mutations in several genes have been linked to some types of epilepsy. Several genes that code for protein subunits of voltage-gated and ligand-gated ion channels have been associated with forms of generalized epilepsy and infantile seizure syndromes.[46] Several ligand-gated ion channels have been linked to some types of frontal and generalized epilepsies. Epilepsy-related mutations in some non-ion channel genes have also been identified.
Epileptogenesis is the process by which a normal brain develops epilepsy after an insult. One interesting finding in animals is that repeated low-level electrical stimulation to some brain sites can lead to permanent increases in seizure susceptibility: in other words, a permanent decrease in seizure "threshold." This phenomenon, known as kindling (by analogy with the use of burning twigs to start a larger fire) was discovered by Dr. Graham Goddard in 1967. Chemical stimulation can also induce seizures; repeated exposures to some pesticides have been shown to induce seizures in both humans and animals. One mechanism proposed for this is called excitotoxicity. The roles of kindling and excitotoxicity, if any, in human epilepsy are currently hotly debated.
Other causes of epilepsy are brain lesions, where there is scar tissue or another abnormal mass of tissue in an area of the brain.
History and stigma
The word epilepsy is derived from the Greek epilepsia, which in turn can be broken into epi- (upon) and lepsis (to take hold of, or seizure)[47] In the past, epilepsy was associated with religious experiences and even demonic possession. In ancient times, epilepsy was known as the "Sacred Disease" because people thought that epileptic seizures were a form of attack by demons, or that the visions experienced by persons with epilepsy were sent by the gods. Among animist Hmong families, for example, epilepsy was understood as an attack by an evil spirit, but the affected person could become revered as a shaman through these otherworldly experiences.[48]
However, in most cultures, persons with epilepsy have been stigmatized, shunned, or even imprisoned; in the Salpêtrière, the birthplace of modern neurology, Jean-Martin Charcot found people with epilepsy side-by-side with the mentally retarded, those with chronic syphilis, and the criminally insane. In Tanzania to this day, as with other parts of Africa, epilepsy is associated with possession by evil spirits, witchcraft, or poisoning and is believed by many to be contagious.[49] In ancient Rome, epilepsy was known as the Morbus Comitialis ('disease of the assembly hall') and was seen as a curse from the gods.
Stigma continues to this day, in both the public and private spheres, but polls suggest it is generally decreasing with time, at least in the developed world; Hippocrates remarked that epilepsy would cease to be considered divine the day it was understood.[50]
Notable people with epilepsy
Many notable people, past and present, have carried the diagnosis of epilepsy. In many cases, their epilepsy is a footnote to their accomplishments; for some, it played an integral role in their fame. Historical diagnoses of epilepsy are not always certain; there is controversy about what is considered an acceptable amount of evidence in support of such a diagnosis.
Legal implications
Most people diagnosed with epilepsy are forbidden by their local laws from operating vehicles. However, there are usually exceptions for those who can prove that they have stabilized their condition. Those few whose seizures do not cause impairment of consciousness, or whose seizures only arise from sleep, may be exempt from such restrictions, depending on local laws. There is an ongoing debate in bioethics over who should bear the burden of ensuring that an epilepsy patient does not drive a car or fly an airplane.
In the U.S., people with epilepsy can drive if their seizures are controlled with treatment and they meet the licensing requirements in their state. How long they have to be free of seizures varies in different states, but it is most likely to be between three months and a year.[51][52] The majority of the 50 states place the burden on patients to report their condition to appropriate licensing authorities so that their privileges can be revoked where appropriate. A minority of states place the burden of reporting on the patient's physician. After reporting is carried out, it is usually the driver's licensing agency that decides to revoke or restrict a driver's license.
In the UK, it is the responsibility of the patients to inform the Driver and Vehicle Licensing Agency (DVLA) if they have epilepsy.[53] The DVLA rules are quite complex,[54] but in summary,[55] those continuing to have seizures or who are within 6 months of medication change may have their licence revoked. A doctor who becomes aware that a patient with uncontrolled epilepsy is continuing to drive has, after reminding the patient of their responsibility, a duty to break confidentiality and inform the DVLA. The doctor should advise the patient of the disclosure and the reasons why their failure to notify the agency obliged the doctor to act.
The Epilepsy Foundation's Jeanne A. Carpenter Epilepsy Legal Defense Fund is dedicated to advancing the rights of people with epilepsy by changing discriminatory practices, policies and laws and to ending epilepsy-related discrimination and injustice through education and increased access to legal services for individuals with epilepsy through a system of managed referrals and legal support to a nationwide network of attorneys committed to this cause.
Additionally, the Epilepsy Foundation is a vigorous advocate for people with epilepsy. In the United States, the Foundation has been active in Congress, the executive branch, and the courts, focusing attention on the needs of those with epilepsy. Priorities for the Foundation include: the availability of affordable quality health care, the search for the cure, and the protection of civil rights for people with epilepsy.
Important investigators of epilepsy
- Jean-Martin Charcot
- John Hughlings Jackson
- Hans Berger
- Herbert Jasper
- Wilder Penfield
- H. Houston Merritt
- William G. Lennox
- Fritz E. Dreifuss
See also
- Non-epileptic seizures
- Epilepsy in animals
- Seizure response dog
- Jacksonian seizure
- Photosensitive epilepsy
- Post-traumatic epilepsy
- Temporal lobe epilepsy
- Abdominal epilepsy
- Generalised epilepsy
- ISAS (Ictal-Interictal SPECT Analysis by SPM)
- Postictal state
- Epilepsy Phenome/Genome Project
References
- ↑ Commission on Epidemiology and Prognosis, International League Against Epilepsy (1993). "Guidelines for epidemiologic studies on epilepsy. Commission on Epidemiology and Prognosis, International League Against Epilepsy". Epilepsia 34 (4): 592–6. doi:. PMID 8330566. http://www.blackwell-synergy.com/doi/pdf/10.1111/j.1528-1157.1993.tb00433.x.
- ↑ Blume W, Lüders H, Mizrahi E, Tassinari C, van Emde Boas W, Engel J (2001). "Glossary of descriptive terminology for ictal semiology: report of the ILAE task force on classification and terminology". Epilepsia 42 (9): 1212–8. doi:. PMID 11580774. http://www.blackwell-synergy.com/doi/full/10.1046/j.1528-1157.2001.22001.x.
- ↑ Fisher R, van Emde Boas W, Blume W, Elger C, Genton P, Lee P, Engel J (2005). "Epileptic seizures and epilepsy: definitions proposed by the International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE)". Epilepsia 46 (4): 470–2. doi:. PMID 15816939. http://www.blackwell-synergy.com/doi/full/10.1111/j.0013-9580.2005.66104.x.
- ↑ "Epilepsy: aetiogy [sic], epidemiology and prognosis". World Health Organization (February 2001). Retrieved on 2007-06-14.
- ↑ Cascino GD (1994). "Epilepsy: contemporary perspectives on evaluation and treatment". Mayo Clinic Proc 69: 1199-1211.
- ↑ Engel J Jr (1996). "Surgery for seizures". NEJM: 647-652.
- ↑ "Proposal for revised clinical and electroencephalographic classification of epileptic seizures. From the Commission on Classification and Terminology of the International League Against Epilepsy". Epilepsia 22 (4): 489–501. 1981. doi:. PMID 6790275.
- ↑ 8.0 8.1 "Proposal for revised classification of epilepsies and epileptic syndromes. Commission on Classification and Terminology of the International League Against Epilepsy". Epilepsia 30 (4): 389–99. 1989. doi:. PMID 2502382.
- ↑ Jerome Engel. "A Proposed Diagnostic Scheme For People With Epileptic Seizures And With Epilepsy: Report Of The Ilae Task Force On Classification And Terminology". ILAE. Retrieved on 2006-07-18.
- ↑ C P Panayiotopoulos and M Koutroumanidis (September 2005). "The significance of the syndromic diagnosis of the epilepsies". National Society for Epilepsy.
- ↑ "Some Canadians may be unknowingly living with epilepsy", CTV.ca (2008-11-30). Retrieved on 2008-12-01.
- ↑ Frucht MM, Quigg M, Schwaner C, Fountain NB. (2000). "Distribution of seizure precipitants among epilepsy syndromes.". Epilepsia 41 (12): 1534–1539..
- ↑ Herzog AG, Harden CL, Liporace J, Pennell P, Schomer DL, Sperling M, et al. (2004). "Frequency of catamenial seizure exacerbation in women with localization-related epilepsy". Annals Neurology 56 (3): 431–34. PMID 15349872.
- ↑ Hirtz D, Thurman DJ, Gwinn-Hardy K, Mohamed M, Chaudhuri AR, Zalutsky R (2007-01-30). "How common are the 'common' neurologic disorders?". Neurology 68 (5): 326–37. doi:. PMID 17261678.
- ↑ Sander JW (2003). "The epidemiology of epilepsy revisited". Curr Opin Neurol 16 (2): 165–70. doi:. PMID 12644744.
- ↑ Walczak TS, Leppik IE, D'Amelio M, Rarick J, So E, Ahman P, Ruggles K, Cascino GD, Annegers JF, Hauser WA (2001). "SIncidence and risk factors in sudden unexpected death in epilepsy: a prospective cohort study.". Neurology 56: 519-525.
- ↑ Lathers, C. and P. Schraeder (1990). Epilepsy and Sudden Death. Dekker, NY, NY..
- ↑ Hitiris, N., R. Mohanraj, J. Norrie and M. J. Brodie (2007). "Mortality in epilepsy". Epilepsy Behavior 10: 363-376.
- ↑ Plioplys S, Dunn DW, Caplan R (2007). "10-year research update review: psychiatric problems in children with epilepsy". J Am Acad Child Adolesc Psychiatry 46 (11): 1389–402. doi:. PMID 18049289.
- ↑ Levisohn PM (2007). "The autism-epilepsy connection". Epilepsia 48 (Suppl 9): 33–5. PMID 18047599.
- ↑ Loiseau P, Duche B, Cordova S, et al (1988). "Prognosis of benign childhood epilepsy with centro-temporal spikes. A follow-up of 168 patients". Epilepsia 29: 229–235.
- ↑ Panayiotopolous CP (2000). "Benign childhood epileptic syndromes with occipital spikes: New classification proposed by the ILAE". J Child Neurol 15: 548-552.
- ↑ Bertrand D, Picard F, Le Hellard S, Weiland S, Favre I, Phillips H, et al. (2002). "How mutations in the nAChRs can cause ADNFLE epilepsy.". Epilepsia 43 Supple 5: 112-122.
- ↑ Koutroumanidis M, Koepp MJ, Richardson MP, Camfield C, Agathonikou A, Ried S, et al (1998). "The variants of reading epilepsy. A clinical and video-EEG study of 17 patients with reading-induced seizures". Brain 121: 1409–1427.
- ↑ Rogers et al (1994). "Autoantibodies to glutamate receptor GluR3 in Rasmussen's encephalitis". Science 265: 648-651.
- ↑ "Dravet Syndrome". Retrieved on 2007-12-16.
- ↑ Eadie MJ, Bladin PF (2001). A Disease Once Sacred: a History of the Medical Understanding of Epilepsy.
- ↑ Cascino GD (1994). "Epilepsy: contemporary perspectives on evaluation and treatment". Mayo Clinic Proc 69: 1199-1211.
- ↑ Engel J Jr (1996). "Surgery for seizures". NEJM: 647-652.
- ↑ Baker GA, Jacoby A, Buck D, et al (1997). "Quality in life in people with epilepsy: a European study". Epilepsia 38: 353–362.
- ↑ Camfiled C, Camfield P, Smith E, et al. (1986). "Asymptomatic children with epilepsy: little benefit from screening for anticonvulsant-induced liver, blood, or renal damage.". Neurology 36: 838-841.
- ↑ mattson RH, Cramer J, COllins JF. (1985). "Comparison of carbemazipine, phenobarbital, phenytoin, and primidone in complex partial seizures.". NEJM 313: 145-151.
- ↑ Kwan P, Brodie MJ. (2000). "Early identification of refractory epilepsy.". NEJM 342: 314-319.
- ↑ Birbeck GL, Hays RD, Cui X, Vickrey BG. (2002). "Seizure reduction and quality of life improvements in people with epilepsy". Epilepsia 43: 535-538.
- ↑ Berg AT, Langfitt JT, Spencer SS, Vickrey BG. (2007). "Stopping antiepileptic drugs after epilepsy surgery: a survey of U.S. epilepsy center neurologists". Epilepsy Behav 10: 219-222.
- ↑ Kelley K, Theodore WH (2005). "Prognosis 30 years after temporal lobectomy". Neurology 64 (11): 1974–6.
- ↑ Wiebe S, Blume WT, Girvin JP, Eliasziw M. (2001). "A randomized, controlled trial of surgery for temporal-lobe epilepsy". N Engl J Med 345: 311-318.
- ↑ Theodore WH, Fisher RS (2004). "Brain stimulation for epilepsy". Lancet Neurol 3: 111-118.
- ↑ Regis, J., M. Rey, F. Bartolomei, V. Vladyka, R. Liscak, O. Schrottner and G. Pendl (2004). "Gamma knife surgery in mesial temporal lobe epilepsy: a prospective multicenter study". Epilepsia 45: 504-515.
- ↑ Takahashi, T. and Y. Tsukahara (1992). "Usefulness of blue sunglasses in photosensitive epilepsy". Epilepsia 33: 517-521.
- ↑ Barriaux, Marianne (2006-10-16). "Dogs trained to warn of an imminent epileptic fit", The Guardian. Retrieved on 2006-11-24.
- ↑ Cheuk D, Wong V (2006). "Acupuncture for epilepsy". Cochrane Database Syst Rev (2): CD005062. doi:. PMID 16625622.
- ↑ Ramaratnam S, Baker GA, Goldstein LH (2005). "Psychological treatments for epilepsy". Cochrane Database Syst Rev (4): CD002029. doi:. PMID 16235293.
- ↑ Ranganathan LN, Ramaratnam S (2005). "Vitamins for epilepsy". Cochrane Database Syst Rev (2): CD004304. doi:. PMID 15846704.
- ↑ Ramaratnam S, Sridharan K (2000). "Yoga for epilepsy". Cochrane Database Syst Rev (3): CD001524. doi:. PMID 10908505.
- ↑ Miriam H. Meisler and Jennifer A. Kearney (2005). "Sodium channel mutations in epilepsy and other neurological disorders". Journal of Clinical Investigation 115 (8): 2010–2017. doi:. PMID 16075041 doi:10.1172/JCI25466.
- ↑ Harper, Douglas (2001). "epilepsy". Online Etymological Dictionary. Retrieved on 2005-06-05.
- ↑ When Epilepsy Goes By Another Name | epilepsy.com
- ↑ Morbus sacer in Africa: some religious aspects of epilepsy in traditional cultures. Jilek-Aall L. PMID: 10080524 Retrieved 8 October 2006.
- ↑ Hippocrates quotes
- ↑ Epilepsy Foundation Driving and You - Can you drive an automobile if you have epilepsy?.
- ↑ Epilepsy Foundation Driver Information by State
- ↑ UK Epilepsy Action: Driving and Epilepsy, I've had a seizure. What should I do?
- ↑ UK Driver and Vehicle Licensing Agency Guide to the Current Medical Standards Of Fitness to Drive. Full details for doctors regarding epilepsy are given in the Appendix. Information for drivers can be found in Medical Rules - Group 1 Licence Holders
- ↑ UK Epilepsy Action: booklet with further details about driving PDF
External links
- Epilepsy at the Open Directory Project
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||