Emergency medical services


Emergency medical services (abbreviated to the initialism "EMS" in some countries) are a branch of Emergency services dedicated to providing out-of-hospital acute medical care and/or transport to definitive care, to patients with illnesses and injuries which the patient, or the First responder, believes constitutes a medical emergency.[1]
Emergency medical services may also be locally known as: First aid squad,[2] Emergency squad,[3] Rescue squad,[4] Ambulance squad,[5] Ambulance service,[6] Ambulance corps[7] or Life squad.[8]
The goal of most emergency medical services is to either provide treatment to those in need of urgent medical care, with the goal of satisfactorily treating the malady, or arranging for timely removal of the patient to the next point of definitive care. This is most likely an emergency department at a hospital or another place where physicians are available. The term Emergency Medical Service evolved to reflect a change from a simple transportation system (ambulance service) to a system in which actual medical care occurred in addition to transportation. In some developing regions, the is not used, or may be used inaccurately, since the service in question does not provide treatment to the patients, but only the provision of transport to the point of care.[9]
In most places in the world, the EMS is summoned by members of the public (or other emergency services, businesses or authority) via an emergency telephone number which puts them in contact with a control facility, which will then dispatch a suitable resource to deal with the situation.[10]
In some parts of the world, the term EMS also encompasses services developed to move patients from one medical facility to an alternative one; inferring transfer a higher level of care. In such services, the EMS is not summoned by members of the public but by clinical professionals (eg. physicians or nurses) in the referring facility. Specialized hospitals that provide higher levels of care may include services such as neonatal intensive care (NICU),[11], pediatric intensive care (PICU), state regional burn centers,[12] specialized care for spinal injury and/or neurosurgery,[13] regional stroke centers,[14] specialized cardiac care[15][16] (cardiac catherization[17]), and specialized/regional trauma care.[18]
In some jurisdictions, EMS units may handle technical rescue operations such as extrication, water rescue, and search and rescue.[19] Training and qualification levels for members and employees of emergency medical services vary widely throughout the world. In some systems, members may be present who are qualified only to drive the ambulance, with no medical training.[9] In contrast, most systems have personnel that retain, at a minimum, a basic first aid certificate (Basic Life Support (BLS)), additionally many EMS systems are staffed with Advanced Life Support (ALS) personnel, including fully qualified paramedics, nurses, or, less commonly, physicians.[20]
Contents |
History
Emergency care in the field has been rendered in different forms since the beginning of recorded history. The New Testament contains the parable of the Good Samaritan, where a man who was beaten is cared for by a Samaritan. Luke 10:34 (NIV) - "He went to him and bandaged his wounds, pouring on oil and wine. Then he put the man on his own donkey, took him to an inn and took care of him." Also during the Middle Ages, the Knights Hospitaller were known for rendering assistance to wounded soldiers in the battlefield.[21]

The first use of the ambulance as a specialized vehicle, in battle came about with the ambulances volantes designed by Dominique Jean Larrey (1766–1842), Napoleon Bonaparte’s chief physician.[22][23] Larrey was present at the battle of Spires, between the French and Prussians, and was distressed by the fact that wounded soldiers were not picked up by the numerous ambulances (which Napoleon required to be stationed two and half miles back from the scene of battle) until after hostilities had ceased, and set about developing a new ambulance system.[24][22][23] Having decided against using the Norman system of horse litters, he settled on two- or four-wheeled horse-drawn wagons, which were used to transport fallen soldiers from the (active) battlefield after they had received early treatment in the field.[23] These 'flying ambulances' were first used by Napoleon's Army of the Rhine is 1793. Larrey subsequently developed similar services for Napoleon's other armies, and adapted his ambulances to the conditions, including developing a litter which could be carried by a camel for a campaign in Egypt.[23]
In civilian ambulances, a major advance was made (which in future years would come to shape policy on hospitals and ambulances) with the introduction of a transport carriage for cholera patients in London during 1832.[25] The statement on the carriage, as printed in The Times, said "The curative process commences the instant the patient is put in to the carriage; time is saved which can be given to the care of the patient; the patient may be driven to the hospital so speedily that the hospitals may be less numerous and located at greater distances from each other".[24] This tenet of ambulances providing instant care, allowing hospitals to be spaced further apart, displays itself in modern emergency medical planning.
The first known hospital-based ambulance service operated out of Commercial Hospital, Cincinnati, Ohio (now the Cincinnati General) by 1865.[24] This was soon followed by other services, notably the New York service provided out of Bellevue Hospital which started in 1869 with ambulances carrying medical equipment, such as splints, a stomach pump, morphine, and brandy, reflecting contemporary medicine.

Also in the late 19th century, the automobile was being developed, and in addition to horse-drawn models, early 20th century ambulances were powered by steam, gasoline, and electricity, reflecting the competing automotive technologies then in existence. However, the first motorized ambulance was brought into service in the last year of the 19th century, with the Michael Reese Hospital, Chicago, taking delivery of the first automobile ambulance, donated by 500 prominent local businessmen, in February 1899.[24] This was followed in 1900 by New York city, who extolled its virtues of greater speed, more safety for the patient, faster stopping and a smoother ride. These first two automobile ambulances were electrically powered with 2hp motors on the rear axle.[24]
During World War One, further advances were made in providing care before and during transport – traction splints were introduced during World War I, and were found to have a positive effect on the morbidity and mortality of patients with leg fractures.[26] Two-way radios became available shortly after World War I, enabling for more efficient radio dispatch of ambulances in some areas. Shortly before World War II, then, a modern ambulance carried advanced medical equipment, was staffed by a physician, and was dispatched by radio. In many locations, however, ambulances were hearses - the only available vehicle that could carry a recumbent patient - and were thus frequently run by funeral homes. These vehicles, which could serve either purpose, were known as combination cars.[27][28]
Advances in the 1960s, especially the development of CPR & defibrillation as the standard form of care for out-of-hospital cardiac arrest, along with new pharmaceuticals, led to changes in the tasks of the ambulances.[29] In Belfast, Northern Ireland the first experimental mobile coronary care ambulance successfully resuscitated patients using these technologies. One well-known report in the USA during that time was Accidental Death and Disability: The Neglected Disease of Modern Society. This report is commonly known as The White Paper.[30] These studies, along with the White Paper report, placed pressure on governments to improve emergency care in general, including the care provided by ambulance services. Part of the result was the creation of standards in ambulance construction concerning the internal height of the patient care area (to allow for an attendant to continue to care for the patient during transport), in the equipment (and thus weight) that an ambulance had to carry, and several other factors.
The purpose of EMS
Emergency medical services exists to fulfill the basic principles of first aid, which are to Preserve Life, Prevent Further Injury, and Promote Recovery.
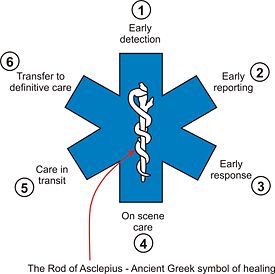
This common theme in medicine is demonstrated by the star of life. The Star of Life shown here, where each of the 'arms' to the star represent one of the 6 points. These 6 points are used to represent the six stages of high quality pre-hospital care, which are:[31]
- Early Detection[31] - Members of the public, or another agency, find the incident and understand the problem
- Early Reporting[31] - The first persons on scene make a call to the emergency medical services and provide details to enable a response to be mounted
- Early Response[31] - The first professional (EMS) rescuers arrive on scene as quickly as possible, enabling care to begin
- Good On Scene Care[31] - The emergency medical service provides appropriate and timely interventions to treat the patient at the scene of the incident
- Care in Transit[31] - the emergency medical service load the patient in to suitable transport and continue to provide appropriate medical care throughout the journey
- Transfer to Definitive Care[31] - the patient is handed over to an appropriate care setting, such as the emergency department at a hospital, in to the care of physicians
Levels of care in EMS



Emergency Medical Service is provided by a variety of individuals, using a variety of methods. To some extent, these will be determined by country and locale, with each individual country having its own 'approach' to how EMS should be provided, and by whom. In some parts of Europe, for example, legislation insists that efforts at providing advanced life support (ALS) services must be physician-led, while other permit some elements of that skill set to specially trained nurses, but have no paramedics. Elsewhere, as in North America, the UK and Australia, ALS services are performed by paramedics, but rarely with the type of direct "hands-on" physician leadership seen in Europe. Increasingly, particularly in the UK and in South Africa, the role is being provided by specially-trained paramedics who are independent practitioners in their own right. Beyond the national model of care, the type Emergency Medical Service will be determined by local jurisdictions and medical authorities, based upon the needs of the community, and the economic resources to support it.
A category of emergency medical service which is known as 'medical retrieval' in some countries (Australia, NZ, Britain) refers to critical care transport of patients between hospitals (as opposed to pre-hospital). Such services are a key element in regionalised systems of hospital care where intensive care services are centralised to a few specialist hospitals.
Generally speaking, the levels of service available will fall into one of three categories; Basic Life Support (BLS), Advanced Life Support (ALS), and care by traditional healthcare professionals, meaning nurses and/or physicians working in the pre-hospital setting and even on ambulances. In some jurisdictions, a fourth level, Intermediate Life Support (ILS), which is essentially a BLS provider with a moderately expanded skill set, may be present, but this level rarely functions independently, and where it is present may replace BLS in the emergency part of the service. When this occurs, any remaining staff at the BLS level is usually relegated to the non-emergency transportation function. Job titles typically include Emergency Medical Technician, Ambulance Technician, or Paramedic. While these job titles are protected by legislation in some countries, this protection is by no means universal, and anyone might, for example, call themselves an 'EMT' or a 'paramedic', regardless of their training, or the lack of it.[32] In some jurisdictions, both technicians and paramedics may be further defined by the environment in which they operate, including such designations as 'Wilderness', 'Tactical', and so on.
Basic Life Support
First Responder
A first responder person who arrives first at the scene of an incident, and whose job is to provide early critical care such as CPR or using an AED.[33] First responders may be dispatched by the ambulance service, may be passers-by, citizen volunteers, or may be members of other agencies such as the police, fire department, or search and rescue.[34]
Ambulance Driver
Some jurisdictions separate the 'driver' and 'attendant' functions, employing ambulance driving staff with no medical qualification (or just a first aid certificate), whose job is to drive the ambulance. While this approach persists in some countries, such as Italy and India, it is generally becoming increasingly rare. Ambulance drivers may be trained in radio communications, ambulance operations and emergency response driving skills.[35]
Ambulance Care Assistant (ACA)
Ambulance Care Assistants have varying levels of training across the world. In many countries, such staff are usually only required to perform patient transport duties (which can include stretcher or wheelchair cases), rather than acute care. However, there remain both countries and individual jurisdictions in which economics will not support ALS service, and the efforts of such individuals may represent the only EMS available. Dependent on the provider (and resources available), they may be trained in first aid or extended skills such as use of an AED, oxygen therapy and other live-saving or palliative skills. In some services, they may also provide emergency cover when other units are not available, or when accompanied by a fully qualified technician or paramedic.[36][37]

Emergency Medical Technician (EMT)
Emergency medical technicians, also known as Ambulance Technicians in the UK and EMT in the United States. Now known as Primary Care Paramedics in parts of Canada. Technicians are usually able to perform a wide range of emergency care skills, such as defibrillation, care of spinal injuries and oxygen therapy.[38][39] In some jurisdictions, some EMTs are able to perform duties as IV and IO cannulation, administration of a limited number of drugs, more advanced airway procedures, CPAP, Analgesic Administration, and limited cardiac monitoring and manual defibrillator capabilities.[40] Most advanced procedures and skills are not within the national scope of practice for an EMT-B.[41] As such most states require additional training and certifications to perform above the national curriculum standards.[42][43]
Advanced Life Support (ALS)
Paramedic (EMT-P)
A paramedic has a high level of prehospital medical training and usually involves key skills not performed by technicians, often including cannulation (and with it the ability to use a range of drugs such as morphine), cardiac monitoring, intubation and other skills such as performing a cricothyrotomy.[44] In many countries, this is a protected title, and use of it without the relevant qualification may result in criminal prosecution.[45] In the United States, paramedics represent the highest licensure level of prehospital emergency care. In addition, several certifications exist for Paramedics such as Wilderness ALS Care,[46] Flight Paramedic Certification (FP-C),[47] and Critical Care EMT-Paramedic.[48]
Critical Care Paramedic (CCEMTP)
A critical care paramedic, also called an advanced practice Paramedic in some US States, represents a higher level of licensure above that of the DOT and NREMT-Paramedic curriculum.[48] These Paramedics receive at least six months of additional training beyond normal EMS medicine in a Critical Care Emergency Medical Transport Program,[48] including critical care use of devices and life support systems normally restricted to the ICU or critical care hospital setting, placement and use of UVCs, UACs, surgical airways, Rapid Sequence Intubation (RSI) intubation, blood administration, and chest tube insertion. The Critical Care Transport role exists in the U.S., and also in a number of other countries (including Canada). The training, permitted skills, and certification requirements vary from one jurisdiction to the next.
Paramedic Practitioner or Emergency Care Practitioner
In the United Kingdom and South Africa, some serving paramedics receive additional university education to become practitioners in their own right, which gives them absolute responsibility for their clinical judgement, including the ability to autonomously prescribe medications, including drugs usually reserved for doctors, such as courses of antibiotics. An emergency care practitioner is a position sometimes referred to as a 'super paramedic' and is designed to bridge the link between ambulance care and the care of a general practitioner. ECPs are university graduates in Emergency Medical Care or qualified paramedics who have undergone further training,[49] and are authorized to perform specialized techniques. Additionally some may prescribe medicines (from a limited list) for longer term care, such as antibiotics. With respect to a Primary Health Care setting, they are also educated in a range of Diagnostic techniques.
'Traditional' Healthcare Professions
Registered Nurse (RN)
The use of registered nurses in the pre-hospital setting is more common in countries that have a limited EMS infrastructure in place. Some European countries such as France or Italy, which do not use paramedics as we understand them, also use nurses as a means of providing ALS services. These nurses may work under the direct supervision of a physician, or, in rarer cases, independently. In some places in Europe, notably Norway, paramedics do exist, but the role of the 'ambulance nurse' continues to be developed,[50] as it is felt that nurses may bring unique skills to some situations encountered by ambulance crews. In North America, and to a lesser extent elsewhere in the English-speaking world, some jurisdictions use specially trained nurses for medical transport work. These are mostly air-medical personnel or critical care transport providers, often working in conjunction with a technician or paramedic or physician on emergency interfacility transports. In the United States, the most common uses of ambulance-based Registered nurses is in the Critical Care/Mobile Intensive Care transport, and in Aeromedical EMS. Such nurses are normally required by their employers (in the US) to seek additional certifications beyond basic nursing registration.
Physician (MD or DO)
There are many places in Europe, most notably in France, Italy, and the German-speaking countries (Germany, Switzerland, Austria) where the model of EMS is different, and physicians take a more direct, 'hands-on' approach to pre-hospital care. In France and Italy, response to high-acuity emergency calls is physician-led, as with the French SMUR teams. Paramedics do not exist within those systems, and most ALS is performed by physicians. In the German-speaking countries, paramedics DO exist, but special physicians (called Notarzt) respond directly to high-acuity calls, supervising the paramedics ALS procedures directly. Indeed, in these countries paramedics are not typically legally permitted to practice their ALS procedures unless the physician is physically present, except in immediately life-threatening emergencies.[51] Some systems - most notably air ambulances in the UK.[52][53] will employ physicians to take the clinical lead in the ambulance; bringing a full range of additional skills such as use of medications that are beyond the paramedic skill set. The response of physicians to emergency calls is routine in many parts of Europe, and not uncommon in the UK..
This 'hands-on' approach is less common in the United States. While one will occasionally see a physician with an ambulance crew on an emergency call, this is much more likely to be the Medical Director or and associate, precepting newly trained paramedics, or performing routine medical quality assurance. In some jurisdictions adult or pediatric critical care transports sometimes use physicians, but generally only when it appears likely that the patient may require surgical or advanced pharmacologic intervention beyond the skills of an EMT, paramedic or nurse during transport. Physicians are leaders of medical retrieval teams in many western countries, where they may assist with the transport of a critically ill, injured, or special needs patient to a tertiary care hospital, particularly when longer transport times are involved.

Prehospital Delivery of care
Depending on country, area within in country, or clinical need, emergency medical services may be provided by one or more different types of organisation. This variation may lead to large differences in levels of care and expected scope of practice.
The most basic emergency medical services are provided as a transport operation only, simply to take patients from their location to the nearest medical treatment. This was often the case in a historical context, and is still true in the developing world, where operators as diverse as taxi drivers[9] and undertakers may operate this service.
Most developed countries now provide a government funded emergency medical service, which can be run on a national level, as is the case in the United Kingdom, where a national network of ambulance trusts operate an emergency service, paid for through central taxation, and available to anyone in need,[54] or can be run on a more regional model, as is the case in the United States, where individual authorities have the responsibility for providing these services.

Ambulance services can be stand alone organisations, but in some cases, the emergency medical service is operated by the local fire[55] or police[56] service. This is particularly common in rural areas, where maintaining a separate service is not necessarily cost effective. This can lead, in some instances, to an illness or injury being attended by a vehicle other than an ambulance, such as fire truck.[57][58][59] In some locales, firefighters are the first responders to calls for emergency medical aid, with separate ambulance services providing transportation to hospitals when necessary.[60]
Some charities or non-profit companies also operate emergency medical services, often alongside a patient transport function.[61] These often focus on providing ambulances for the community, or for cover at private events, such as sports matches. The Red Cross provides this service in many countries across the world on a volunteer basis (and in others as a Private Ambulance Service), as do some other smaller organizations such as St John Ambulance.[62] and the Order of Malta Ambulance Corps.[63] In some countries, these volunteer ambulances may be seen providing support to the full time ambulance crews during times of emergency, or simply to help cover busy periods.[64]
There are also private ambulance companies, with paid employees, but often on contract to the local or national government. Many private companies provide only the patient transport elements of ambulance care (i.e. non urgent), although in some places these private services are contracted to provide emergency care, or to form a 'second tier' response, where they only respond to emergencies when all of the full-time emergency ambulance crews are busy or to respond to non-emergency home calls. Private companies are often contracted by private clients to provide event specific cover, as is the case with voluntary EMS crews.[65]
Strategies for delivering care
The essential decision in prehospital care is whether the patient should be immediately taken to the hospital, or advanced care resources are taken to the patient where they lie. The "scoop and run" approach is exemplified by the MEDEVAC aeromedical evacuation helicopter, where the "stay and play" is exemplified by the French SMUR emergency mobile resuscitation unit.
The strategy developed for prehospital trauma care in North America is based on the Golden Hour theory, i.e., that a trauma victim's best chance for survival is in an operating room, with the goal of having the patient in surgery within an hour of the traumatic event. This appears to be true in cases of internal bleeding, especially penetrating trauma such as gunshot or stab wounds. Thus, minimal time is spent providing prehospital care ("ABCs", i.e. ensure airway, breathing and circulation; external bleeding control; spine immobilization; endotracheal intubation) and the victim is transported as fast as possible to a trauma center.[66]
The aim in "Scoop and Run" treatment is generally to transport the patient within ten minutes of arrival, hence the birth of the phrase, "the platinum ten minutes" (in addition to the "golden hour"), now commonly used in EMT training programs. The "Scoop and Run" is a method developed to deal with trauma, rather than strictly medical situations (e.g. cardiac or respiratory emergencies), however, this may be changing. Increasingly, research into the management of S-T segment elevation myocardial infarctions (STEMI) occurring outside of the hospital, or even inside community hospitals without their own PCI labs, suggests that time to treatment is a clinically significant factor in heart attacks, and that trauma patients may not be the only patients for whom 'load and go' is clinically appropriate. In such conditions, the gold standard is the door to balloon time. The longer the time interval, the greater the damage to the myocardium, and the poorer the long-term prognosis for the patient.[67] Current research in Canada has suggested that door to balloon times are significantly lower when appropriate patients are identified by paramedics in the field, instead of the emergency room, and then transported directly to a waiting PCI lab.[68] In a related program in Toronto, EMS has begun to use a procedure of 'rescuing' STEMI patients from the Emergency Rooms of hospitals without PCI labs, and transporting them, on an emergency basis, to waiting PCI labs in other hospitals.[69]
Models of care
Although a variety of differing philosophical approaches are used in the provision of EMS care around the world, they can generally be placed into one of two categories; one physician-led and the other paramedic-led with accompanying physician oversight. These models are typically identified by their locations of origin.[70] The Franco-German model is physician-led, with doctors responding directly to all major emergencies requiring more than simple first aid. In some cases in this model, such as France, paramedics, as we understand them, do not exist at all. The term 'paramedic' is used generically in France, and those with that designation have training that is similar to an U.S. EMT-B.[71] The team's physicians and in some cases, nurses, provide all medical interventions for the patient, and non-medical members of the team simply provide the driving and heavy lifting services. In other applications of this model, as in Germany, a paramedic equivalent does exist, but is sharply restricted in terms of scope of practice; often not permitted to perform Advanced Life Support (ALS) procedures unless the physician is physically present, except in cases of immediate life-threat.[72] Ambulances in this model tend to be better equipped with more advanced medical devices, in essence, bringing the emergency department to the patient. High-speed transport to hospitals is considered, in most cases, to be unnecessarily unsafe, and the preference is to remain and provide definitive care to the patient until they are medically stable, and then accomplish transport. In this model, the physician and nurse may actually staff an ambulance along with a driver, or may staff a rapid response vehicle instead of an ambulance, providing medical support to multiple ambulances.
The second model, the Anglo-American model, utilizes trained technicians, usually referred to as paramedics, to staff ambulances, which may be classified according to the varying skill levels of the crews. In this model it is rare to find a physician actually working in the pre-hospital setting. More typically, they provide medical oversight for the work of emergency medical technicians and paramedics, which may be accomplished in terms of off-line medical control, with protocols or 'standing orders' for certain types of medical procedures or care, or on-line medical control, in which the technician must establish contact with the physician, usually at the hospital, and receive direct orders for various types of medical interventions. Patients may be treated at the scene up to the level of the technician's skill set, and then transported to hospital, but in many cases, the limited skill set of the technician and the needs of the patient will result in the rapid and timely transport of the patient to a hospital, at which point definitive care will begin. As a new development in the Anglo-American model, some paramedics in some jurisdictions (U.K., South Africa, Australia) are evolving beyond the level of technician, and being permitted to provide more definitive primary care to patients, often including suturing, detailed assessment, in some cases limited authority to prescribe medications (usually from a limited list), and to function as independent practitioners in their own right.[73]
Clinical governance
Paramedics normally function under the authority (medical direction) of one or more physicians charged with legally establishing the emergency medical directives for a particular region. Paramedics are credentialed and authorized by these physicians to use their own clinical judgment and diagnostic tools to identify medical emergencies and to administer the appropriate treatment, including drugs that would normally require a physician order. Credentialing may occur as the result of a State Medical Board examination (U.S.) or the National Registry of Emergency Medical Technicians (U.S.). In England, and in some parts of Canada, credentialing may occur by means of a College of Paramedicine.[74] In these cases, paramedics are regarded as a self-regulating health profession. The final common method of credentialing is through certification by a Medical Director and permission to practice as an extension of the Medical Director's license to practice medicine. The authority to practice in this semi-autonomous manner is granted in the form of standing order protocols (off-line medical control) and in some cases direct physician consultation via phone or radio (on-line medical control). Under this paradigm, paramedics effectively assume the role of out-of-hospital field agents to regional emergency physicians, with independent clinical decision-making authority that is typically enjoyed only by expert clinicians within the hospital setting. In some parts of Europe, most notably in Germany, those in the paramedic role are only permitted to practise many of their advanced skills while assisting a physician who is physically present, except in cases of immediately life-threatening emergencies.[75] In other parts of Europe, most notably in France, all ALS skills in the pre-hospital setting are performed by physicians and nurses, and the role of paramedic is unknown. In certain other jurisdictions, such as the United Kingdom and South Africa, paramedics may be entirely autonomous practitioners capable of prescribing medications.[76] In other jurisdictions, such as Australia and Canada this expanded scope of practice is under active consideration and discussion[77]
Organization in different countries
- Emergency Medical Services in the United States
- Emergency Medical Services in Canada
- Emergency Medical Services in France
- Emergency Medical Services in the United Kingdom
- Emergency Medical Services in Germany
- Emergency Medical Services in Italy
- Emergency Medical Services in Norway
- Emergency medical services in Australia
- Emergency medical services in South Africa
- Magen David Adom the Israeli ambulance service
See also
- Ambulance
- Wilderness Emergency Medical Technician
- Wilderness First Responder
- 9-1-1
- Battlefield medicine
- Prehospital Medicine
- Emergency medicine
- The White Paper
- Good Samaritan law
- Cardiopulmonary resuscitation
- CEN 1789
References
- ↑ "What is EMS?". NHTSA. Retrieved on 3008-08-09.
- ↑ "Long Hill Township First Aid Squad". Retrieved on 2007-06-18.
- ↑ "Hennepin County Emergency Squad". Retrieved on 2007-06-18.
- ↑ "South Plainfield Rescue Squad". Retrieved on 2007-06-18.
- ↑ "Nottingham Ambulance Squad". Retrieved on 2007-06-18.
- ↑ "Scottish Ambulance Service". Retrieved on 2007-06-18.
- ↑ "Valhalla Volunteer Ambulance Corps". Retrieved on 2007-06-18.
- ↑ "Sardinia Life Squad". Retrieved on 2007-06-18.
- ↑ 9.0 9.1 9.2 "Motorcycle Ambulance Trailer Project Gets Off The Ground With MAN ERF UK", Transport News Network (2006-07-04). Retrieved on 2008-08-07.
- ↑ "EU document on European adoption of 112 emergency number". Retrieved on 2007-06-29.
- ↑ "Crouse-Irving NICU". Retrieved on 2008-08-09.
- ↑ "Strong Memorial Burn Center". Retrieved on 2008-08-09.
- ↑ "Avera Neurosciences Institute". Retrieved on 2008-08-09.
- ↑ "NYS DOH Regional Stroke Centers". Retrieved on 2008-08-09.
- ↑ "Cath Labs". Retrieved on 2008-08-09.
- ↑ "NHS Heart Hospital". Retrieved on 2008-08-11.
- ↑ "AHA Cath Lab Definition". Retrieved on 2008-08-09.
- ↑ "Maryland Shock Trauma". Retrieved on 2008-08-09.
- ↑ "EMS Special Operations". Town of Colonie EMS. Retrieved on 2007-06-29.
- ↑ "Difference between EMT (BLS and Paramedic (ALS)". Retrieved on 2008-08-20.
- ↑ "Knights Hspitaller's". Retrieved on 2008-08-20.
- ↑ 22.0 22.1 Skandalakis, PN; Lainas, P; Zoras, O; Skandalakis, JE; Mirilas, P (August 2006). ""To afford the wounded speedy assistance": Dominique Jean Larrey and Napoleon". World Journal of Surgery 30 (8). http://www.ncbi.nlm.nih.gov/pubmed/16850154.
- ↑ 23.0 23.1 23.2 23.3 Ortiz, Captain Jose M (October-December 1998). The Revolutionary Flying Ambulance of Napoleon's Surgeon. pp. 17-25. http://napoleonic-literature.com/Flying_Ambulance.htm.
- ↑ 24.0 24.1 24.2 24.3 24.4 Barkley, Katherine (1978). The ambulance: the story of emergency transportation of sick and wounded through the centuries. New York: Exposition Press. ISBN 0-682-48983-2.
- ↑ "Cholera carriages". Retrieved on 2008-08-09.
- ↑ "Traction splint history". Retrieved on 2008-08-08.
- ↑ Kuehl, Alexander E. (Ed.). Prehospital Systems and Medical Oversight, 3rd edition. National Association of EMS Physicians. 2002. @ ch. 1.
- ↑ "Miller-Meteor History". Miller-Meteor. n.d. Retrieved 23 February 2007
- ↑ Kouwenhoven WB, Jude JR, Knickerbocker GG. Closed-chest cardiac massage, JAMA. 1960;173:94-97.
- ↑ "EMS History". Retrieved on 2008-08-20.
- ↑ 31.0 31.1 31.2 31.3 31.4 31.5 31.6 "Design, Origin and Meaning of the Star of Life". NHTSA. Retrieved on 2008-08-09.
- ↑ "Great Britain EMT". Retrieved on 2008-08-20.
- ↑ "Resuscitation Council UK First Responders". Retrieved on 2008-08-20.
- ↑ "Flesueur Police Department". Retrieved on 2008-08-20.
- ↑ "Union EMS". Retrieved on 2008-08-20.
- ↑ "NHS Careers". Retrieved on 2008-08-20.
- ↑ "ACA job description". Retrieved on 2008-08-20.
- ↑ "Dept. of Labor EMT Job Description". Retrieved on 2008-08-20.
- ↑ "NYS EMT-B Job Description". Retrieved on 2008-08-20.
- ↑ "North Dakota EMT-B Scope of Practice". Retrieved on 2008-08-20.
- ↑ "NHTSA EMT-B Scope of Practice". Retrieved on 2008-08-20.
- ↑ "EMT-B additional skills". Retrieved on 2008-08-20.
- ↑ "Colorado EMT-B IV Certification". Retrieved on 2008-08-20.
- ↑ "Paramedic: Job description". Retrieved on 2008-08-20.
- ↑ "HPC - Health Professions Council - Protected titles". Retrieved on 2008-08-20.
- ↑ "Wilderness RAT ALS team". Retrieved on 2008-08-20.
- ↑ "Flight Paramedic Certification". Retrieved on 2008-08-20.
- ↑ 48.0 48.1 48.2 "CCEMTP". Retrieved on 2008-08-20.
- ↑ "South Western Ambulance Service NHS Trust". Retrieved on 2008-08-20.
- ↑ http://cat.inist.fr/?aModele=afficheN&cpsidt=17099575
- ↑ http://www.bundesaerztekammer.de/page.asp?his=0.7.47.3222
- ↑ "Londons Air Ambulance". Retrieved on 2007-06-18.
- ↑ "Surrey Air Ambulance". Retrieved on 2007-06-18.
- ↑ "UK NHS Ambulance Service Information". Retrieved on 2007-06-02.
- ↑ "Fire Service Based EMS advocates ruffle some feathers!". Retrieved on 2008-08-09.
- ↑ http://www.police.co.nassau.ny.us/eab.htm
- ↑ "Hillside Fire Department". Retrieved on 2008-08-20.
- ↑ "Why does a fire truck come to my house when I call 911 for an ambulance?".
- ↑ "Our lazy firemen must make a radical change". Retrieved on 2008-08-09.
- ↑ "Success hat-trick underlines firefighters community commitment". West Sussex County Council. Retrieved on 2008-08-09.
- ↑ "British Red Cross Voluntary Ambulance Service". Retrieved on 2007-06-02.
- ↑ "St John Ambulance First Aid Cover for Events". Retrieved on 2007-06-02.
- ↑ "Order of Malta Ambulance Corps". Retrieved on 2007-06-02.
- ↑ "Volunteers on hand for flood help". Retrieved on 2008-01-21.
- ↑ "WANT Medical Service". Retrieved on 2008-08-20.
- ↑ Accidental Death and Disability: The Neglected Disease of Modern Society, (1966), National Academy of Sciences (White Paper)
- ↑ Nallamothu BK, Bates ER. Percutaneous coronary intervention versus fibrinolytic therapy in acute myocardial infarction: Is timing (almost) everything? Am J Cardiol 2003;92:824-6.
- ↑ Bogaty P, Buller CE, Dorian P, O'Neill BJ, Armstrong PW. Applying the new STEMI guidelines: 1. Reperfusion in acute ST-segment elevation myocardial infarction. CMAJ 2004;171(9):1039-41.
- ↑ Cantor, W.J., Morrison, L.J., Guidelines for STEMI (correspondence). CMAJ 2005; 172 (11).
- ↑ Dick WF (2003). "Anglo-American vs. Franco-German emergency medical services system". Prehosp Disaster Med 18 (1): 29–35; discussion 35–7. PMID 14694898.
- ↑ "SAMU de France website". Retrieved on 2008-09-19.
- ↑ German Federal Board of Physicians: Directives regarding emergency powers for Paramedics
- ↑ "What Does a Super Paramedic Do? (BBC News website)". Retrieved on 2008-09-19.
- ↑ http://www.britishparamedic.org
- ↑ http://www.bundesaerztekammer.de/page.asp?his=0.7.47.3222 (In German)
- ↑ Cooper S, Barrett B, Black S, et al. The emerging role of the emergency care practitioner, Emerg Med J, 2004;21(5):614-8
- ↑ http://www.acap.org.au/tas/documents/reports/issues_report.htm.
Further reading
- Planning Emergency Medical Communications: Volume 2, Local/Regional Level Planning Guide, (Washington, D.C.: National Highway Traffic Safety Administration, US Department of Transportation, 1995).
External links
- National Association of Emergency Medical Technicians Homepage
- National Collegiate Emergency Medical Services Foundation Homepage
- National EMS Memorial Service Webpage
- National Registry of Emergency Medical Technicians
- Emergency Medical Services at the Open Directory Project
- National Rural and Frontier Emergency Medical Services Agenda for the Future
|
||||||||
|
|||||||||||||||||
|
|||||