Echocardiography
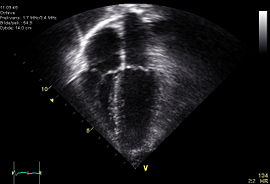

An echocardiogram, often referred to in the medical community as an ECHO, is a sonogram of the heart. Also known as a cardiac ultrasound, it uses standard ultrasound techniques to image two-dimensional slices of the heart. The latest ultrasound systems now employ 3D real-time imaging.
In addition to creating two-dimensional pictures of the cardiovascular system, an echocardiogram can also produce accurate assessment of the velocity of blood and cardiac tissue at any arbitrary point using pulsed or continuous wave Doppler ultrasound. This allows assessment of cardiac valve areas and function, any abnormal communications between the left and right side of the heart, any leaking of blood through the valves (valvular regurgitation), and calculation of the cardiac output as well as the Ejection fraction.
Echocardiography was an early medical application of ultrasound. Echocardiography was also the first application of intravenous contrast-enhanced ultrasound. This technique injects gas-filled microbubbles into the venous system to improve tissue and blood delineation. Contrast is also currently being evaluated for its effectiveness in evaluating myocardial perfusion. It can also be used with Doppler ultrasound to improve flow-related measurements (see Doppler echocardiography).
Echocardiography is usually performed by cardiac sonographers and interpreted by a cardiologist.
Contents |
Purpose
Echocardiography is used to diagnose cardiovascular diseases. In fact, it is one of the most widely used diagnostic tests for heart disease. It can provide a wealth of helpful information, including the size and shape of the heart, its pumping capacity and the location and extent of any damage to its tissues. It is especially useful for assessing diseases of the heart valves. It not only allows doctors to evaluate the heart valves, but it can detect abnormalities in the pattern of blood flow, such as the backward flow of blood through partly closed heart valves, known as regurgitation. By assessing the motion of the heart wall, echocardiography can help detect the presence and assess the severity of coronary artery disease, as well as help determine whether any chest pain is related to heart disease. Echocardiography can also help detect hypertrophic cardiomyopathy, in which the walls of the heart thicken in an attempt to compensate for heart muscle weakness. The biggest advantage to echocardiography is that it is noninvasive (doesn't involve breaking the skin or entering body cavities) and has no known risks or side effects.
Transthoracic echocardiogram
A standard echocardiogram is also known as a transthoracic echocardiogram (TTE), or cardiac ultrasound. In this case, the echocardiography transducer (or probe) is placed on the chest wall (or thorax) of the subject, and images are taken through the chest wall. This is a non-invasive, highly accurate and quick assessment of the overall health of the heart. A cardiologist can quickly assess a patient's heart valves and degree of heart muscle contraction (an indicator of the ejection fraction). The images are displayed on a monitor, and are recorded either by videotape (analog) or by digital techniques.
An echocardiogram can be used to evaluate all four chambers of the heart. It can determine strength of the heart, the condition of the heart valves, the lining of the heart (the pericardium), and the aorta. It can be used to detect a heart attack, enlargement or hypertrophy of the heart, infiltration of the heart with an abnormal substance. Weakness of the heart, cardiac tumors, and a variety of other findings can be diagnosed with an echocardiogram. With advanced measurements of the movement of the tissue with time (tissue doppler), it can measure diastolic function, fluid status[1], and dys-synchrony.
The TTE is highly accurate for identifying vegetations (masses consisting of a mixture of bacteria and blood clots), but the accuracy can be reduced in up to 20% of adults because of obesity, chronic obstructive pulmonary disease, chest-wall deformities, or otherwise technically difficult patients. TTE in adults is also of limited use for the structures at the back of the heart, such as the left atrial appendage. Transesophageal echocardiography may be more accurate than TTE because it excludes the variables previously mentioned and allows closer visualization of common sites for vegetations and other abnormalities. Transesophageal echocardiography also affords better visualization of prosthetic heart valves.
Transesophageal echocardiogram
This is an alternative way to perform an echocardiogram. A specialized probe containing an ultrasound transducer at its tip is passed into the patient's esophagus. This allows image and Doppler evaluation which can be recorded. This is known as a transesophageal echocardiogram, or TEE (TOE in the United Kingdom). The advantage of TEE over TTE is usually clearer images, especially of structures that are difficult to view transthoracicly (through the chest wall). The explanation for this is the heart rests directly upon the esophagus leaving only millimeters in distance that the ultrasound beam has to travel. This reduces the attenuation (weakening) of the ultrasound signal, generating a stronger return signal, ultimately enhancing image and Doppler quality. Comparatively, transthoracic ultrasound must first traverse skin, fat, ribs and lungs before reflecting off the heart and back to the probe before an image can be created. All these structures, along with the increased distance the beam must travel, weaken the ultrasound signal thus degrading the image and Doppler quality.
In adults, several structures can be evaluated and imaged better with the TEE, including the aorta, pulmonary artery, valves of the heart, both atria, atrial septum, left atrial appendage, and coronary arteries. TEE has a very high sensitivity for locating a blood clot inside the left atrium (www.heartsite.com). While TTE can be performed quickly, easily and without pain to the patient, TEE requires a fasting patient,(a person who is unable to eat or drink after midnight on the day before the procedure), a team of medical personnel, takes longer to perform, is uncomfortable for the patient and has some risks associated with the procedure (esophageal perforation--1 in 10,000, and adverse reactions to the medication).
Before inserting the probe, conscious sedation is induced with the patient to ease the discomfort of the individual and to decrease the gag reflex, thus making the ultrasound probe easier to pass into the esophagus. Conscious sedation is a light sedation usually using the medications midazolam (a benzodiazepine with sedating, amnesiac qualities) and fentanyl. Sometimes a local anesthetic spray is used for the back of the throat, such a xylocaine and/or a jelly/lubricant anesthetic for the esophagus. Children are anesthetized. Unlike the TTE, the TEE is considered an invasive procedure and is thus performed by physicians in the U.S., not sonographers.
3-dimensional echocardiography

3-D echocardiography is now possible, using an ultrasound probe with an array of transducers and an appropriate processing system. This enables detailed anatomical assessment of cardiac pathology, particularly valvular defects,[2] and cardiomyopathies.[3]. The possibility of slicing the virtual heart in infinite planes in anatomically appropriate manner and reconstruct 3dimensional images of anatomic structures make 3D echocardiography unique for understanding the congenitally malformed heart. (Ref: Impact of Multiplanar Review of Three-Dimensional Echocardiographic Data on Management of Congenital Heart Disease. Ann. Thorac. Surg., September 2008; 86: 875 - 881).
Accreditation
The "Intersocietal Commission for the Accreditation of Echocardiography Laboratories" (ICAEL) sets standards for the echo labs, cardiologists and technologists in the US to comply to. Once all requirements have been met, the lab will receive ICAEL certification. A lab that has received the certification may also receive higher reimbursement from insurance companies such as Medicare and United Healthcare. http://www.icael.org/icael/index.htm
In the UK, accreditation is done by the British Society of Echocardiography. Accredited technologists or other professionals from the echocardiography field will have completed a logbook and passed an exam.
See also
- Angiogram
- Aortic valve area calculation
- Electrocardiogram
- Fetal echocardiography
References
- ↑ Ommen SR, Nishimura RA, Appleton CP, Miller FA, Oh JK, Redfield MM, Tajik AJ. (2000). "Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: A comparative simultaneous Doppler-catheterization study" (PDF). Circulation 102 (15): 1788–94. PMID 11023933. http://circ.ahajournals.org/cgi/reprint/102/15/1788.pdf.
- ↑ Poh KK, Levine RA, Solis J, Shen L, Flaherty M, Kang YJ, Guerrero JL, Hung J. (2008). "Assessing aortic valve area in aortic stenosis by continuity equation: a novel approach using real-time three-dimensional echocardiography". Eur Heart J. doi:. PMID 18263866.
- ↑ Goland S, Czer LS, Luthringer D, Siegel RJ. (2008). "A case of arrhythmogenic right ventricular cardiomyopathy". Can J Cardiol 24 (1): 61–2. PMID 18209772.